You might also like
- Esophageal Varices, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandEsophageal Varices, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- CME Upper GI BleedDocument46 pagesCME Upper GI Bleedfarah fadzilNo ratings yet
- Lower GI BleedingDocument3 pagesLower GI BleedingTaleb AliNo ratings yet
- Hematochezia: Dr. Lianda Siregar, SP - PD Fakultas Kedokteran UNMUL, Bagian Ilmu Penyakit DalamDocument33 pagesHematochezia: Dr. Lianda Siregar, SP - PD Fakultas Kedokteran UNMUL, Bagian Ilmu Penyakit DalamMink M SarjanaNo ratings yet
- GI BleedDocument28 pagesGI BleedAnn Lan100% (1)
- GI Bleeding 20-21Document38 pagesGI Bleeding 20-212859bathinaNo ratings yet
- 5 MED 4 - Approach To GI BleedingDocument6 pages5 MED 4 - Approach To GI BleedingIan CruzNo ratings yet
- Group 1 Fadzliana Yamuna Atirah Siti RohaniDocument21 pagesGroup 1 Fadzliana Yamuna Atirah Siti RohaniWan Mastura Wan MusaludinNo ratings yet
- Upper Gi BleedingDocument37 pagesUpper Gi Bleedingfathima AlfasNo ratings yet
- Acute GI Bleeding: Louis Chaptini MDDocument67 pagesAcute GI Bleeding: Louis Chaptini MDSiti RahayuNo ratings yet
- GIT BleedingDocument7 pagesGIT Bleedingفاطمة عبدالخالقNo ratings yet
- Day 10. Choledocholitiasis, CholangitisDocument26 pagesDay 10. Choledocholitiasis, Cholangitisهنادي رازمNo ratings yet
- Gastro POMDocument63 pagesGastro POMLionell Castillo100% (1)
- Esophageal VaricesDocument4 pagesEsophageal Varicesbrian3442No ratings yet
- Blood in Urine/blood in Stool/blood From Any Site: Dr. Bhavesh KhandharDocument18 pagesBlood in Urine/blood in Stool/blood From Any Site: Dr. Bhavesh KhandharDeep ShahNo ratings yet
- 105 116 Acute Gastrointestinal BleedingDocument12 pages105 116 Acute Gastrointestinal Bleedingmonia agni wiyatamiNo ratings yet
- Gastrointestinal BleedingDocument57 pagesGastrointestinal Bleedingapi-1964133767% (3)
- Gastrointestinal Bleeding - StatPearls - NCBI BookshelfDocument7 pagesGastrointestinal Bleeding - StatPearls - NCBI BookshelfAdam GenturNo ratings yet
- ULGIBDocument31 pagesULGIBEzraNo ratings yet
- Prepared by Inzar Yasin Ammar LabibDocument47 pagesPrepared by Inzar Yasin Ammar LabibdiaNo ratings yet
- Lower GIT BleedingDocument30 pagesLower GIT BleedingRonald Joy DatuNo ratings yet
- Upper Gastrointestinal BleedingDocument46 pagesUpper Gastrointestinal BleedingRashed ShatnawiNo ratings yet
- Prepared by Inzar Yasin Ammar LabibDocument47 pagesPrepared by Inzar Yasin Ammar LabibJohn Clements Galiza100% (1)
- Small Bowel Obstruction &post Operative IleusDocument62 pagesSmall Bowel Obstruction &post Operative IleusMamanya Fadhil HaniNo ratings yet
- 5 - Gastrointestinal Bleeding (AMBOSS) ?Document6 pages5 - Gastrointestinal Bleeding (AMBOSS) ?Rawabi rawabi1997No ratings yet
- Lower Gastrointestinal Bleeding (LGIB)Document41 pagesLower Gastrointestinal Bleeding (LGIB)api-196413370% (1)
- UgumDocument50 pagesUgumhailu henockNo ratings yet
- LP Hematesis MelenaDocument30 pagesLP Hematesis MelenaDimaz Al AzharNo ratings yet
- Upper Gastrointestinal Haemorrhage: S5 Unit 2006 Mbbs Batch Trivandrum Medical CollegeDocument194 pagesUpper Gastrointestinal Haemorrhage: S5 Unit 2006 Mbbs Batch Trivandrum Medical CollegeSrini VasanNo ratings yet
- Bowel Obstruction Vs IleusDocument62 pagesBowel Obstruction Vs IleusSandra SuryariniNo ratings yet
- Ugib &lgibDocument41 pagesUgib &lgibDawex IsraelNo ratings yet
- Hematemesis Melena (Upper Gi Bleeding)Document134 pagesHematemesis Melena (Upper Gi Bleeding)Mardoni Efrijon100% (1)
- Peptic Ulcer ComplicationsDocument9 pagesPeptic Ulcer Complicationskhaled alsulaimNo ratings yet
- Acute AbdomenDocument56 pagesAcute AbdomenponekNo ratings yet
- Diverticular Disease: Qbank Session Clinical Sciences LearnedDocument11 pagesDiverticular Disease: Qbank Session Clinical Sciences LearnedMike GNo ratings yet
- What Are The Signs of Bleeding in The Digestive Tract?Document6 pagesWhat Are The Signs of Bleeding in The Digestive Tract?draganNo ratings yet
- Upper Gastrointestinal Bleeding: EL IlcoxDocument1 pageUpper Gastrointestinal Bleeding: EL IlcoxdaisyNo ratings yet
- Blood in StoolDocument3 pagesBlood in StoolRae RayNo ratings yet
- Surgery Lect 5 LiverDocument39 pagesSurgery Lect 5 Liveraparna shamaNo ratings yet
- CholangitisDocument19 pagesCholangitisJohn mvulaNo ratings yet
- Esophageal VaricesDocument9 pagesEsophageal VaricesErina WahyuniNo ratings yet
- Gastrointestinal BleedingDocument35 pagesGastrointestinal Bleedingtheeba 19No ratings yet
- Acute GI BleedingDocument35 pagesAcute GI BleedingGalih GimastiarNo ratings yet
- Upper Gastrointestinal Bleeding 4 Juni 2009Document36 pagesUpper Gastrointestinal Bleeding 4 Juni 2009YennySuryaniNo ratings yet
- Gastric VaricesDocument5 pagesGastric VaricesNadzarul AfizanNo ratings yet
- Intestinal ObstructionDocument15 pagesIntestinal ObstructionEmmeline Dycangchon-GarmaNo ratings yet
- Acute Gi Bleeding: Rohman AzzamDocument34 pagesAcute Gi Bleeding: Rohman AzzamgebyarayuNo ratings yet
- 16-GIT BleedingDocument6 pages16-GIT Bleedings2111110520No ratings yet
- Gastrointestinal Bleeding Aug 24-1Document82 pagesGastrointestinal Bleeding Aug 24-1xiongmao2389No ratings yet
- 25.gastrointestinal BleedingDocument12 pages25.gastrointestinal BleedingJayanthNo ratings yet
- Management of Upper Gi BleedingDocument41 pagesManagement of Upper Gi Bleedingkaukab azimNo ratings yet
- Surgery - Oral ExamDocument37 pagesSurgery - Oral ExamShidev100% (1)
- Materi Kep. Kritis Acute GI BleedingDocument35 pagesMateri Kep. Kritis Acute GI Bleedingharsani auroraNo ratings yet
- Gastroesophageal Reflux DiseaseDocument11 pagesGastroesophageal Reflux DiseaseMike GNo ratings yet
- Congested Mucosal Subepithelial Vascular Cushions: 3, 7 & 11 O'clockDocument55 pagesCongested Mucosal Subepithelial Vascular Cushions: 3, 7 & 11 O'clockAlNo ratings yet
- Upper Gi BleedDocument43 pagesUpper Gi BleedPreethi GudipalliNo ratings yet
- Ascending CholangitisDocument7 pagesAscending CholangitisAmar HasanNo ratings yet
- Divisi Gastroentero-Hepatologi Rsup.H. Adam Malik MedanDocument23 pagesDivisi Gastroentero-Hepatologi Rsup.H. Adam Malik MedanSarachanda SallyNo ratings yet
- Intestinalobstruction 150401053831 Conversion Gate01Document65 pagesIntestinalobstruction 150401053831 Conversion Gate01Nina NoviaNo ratings yet
- Deva KGD 1 PMDocument103 pagesDeva KGD 1 PMdevaNo ratings yet
- Chronic Mesenteric IschaemiaDocument2 pagesChronic Mesenteric IschaemiaMike GNo ratings yet
- Cerebral cortex nervous system infectio...es_ Diagrams & Illustrations _ OsmosisDocument13 pagesCerebral cortex nervous system infectio...es_ Diagrams & Illustrations _ OsmosisMike GNo ratings yet
- Compartment syndromeDocument10 pagesCompartment syndromeMike GNo ratings yet
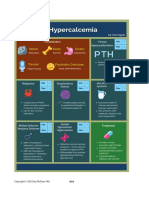
- HypercalcemiaDocument1 pageHypercalcemiaMike GNo ratings yet
- CBC DiffDocument8 pagesCBC DiffMike GNo ratings yet
- Neuro Dementia 2022Document5 pagesNeuro Dementia 2022Mike GNo ratings yet
- 2.15 Interpretasi Darah 3 Sudah Di Stabilo PDFDocument1 page2.15 Interpretasi Darah 3 Sudah Di Stabilo PDFalodiaNo ratings yet
- Acute Coronary SyndromeDocument1 pageAcute Coronary SyndromeMike GNo ratings yet
- Trauma and Burns MedCosmos Surgery - MCQDocument32 pagesTrauma and Burns MedCosmos Surgery - MCQMike GNo ratings yet
- Differential Diagnosis of Neck Swellings PDFDocument3 pagesDifferential Diagnosis of Neck Swellings PDFSiddharth KatyalNo ratings yet
- Classification of ShockDocument3 pagesClassification of ShockYogi drNo ratings yet
- Gastrointestinal Bleeding PDFDocument1 pageGastrointestinal Bleeding PDFYogi drNo ratings yet
- Immediate Management of Life Iate Management of Life-Threatening Problems Threatening ProblemsDocument3 pagesImmediate Management of Life Iate Management of Life-Threatening Problems Threatening ProblemsMike GNo ratings yet
- Approach To Jundiced PatientDocument2 pagesApproach To Jundiced Patientmelinda SilalahiNo ratings yet
- Antaomy of GITDocument5 pagesAntaomy of GITMike GNo ratings yet
- Stomach-Esophagus MedCosmos Surgery - MCQDocument39 pagesStomach-Esophagus MedCosmos Surgery - MCQMike G100% (1)
- Solid Visceral Injuries Solid Visceral Injuries Solid Visceral InjuriesDocument2 pagesSolid Visceral Injuries Solid Visceral Injuries Solid Visceral InjuriesMike GNo ratings yet
- Spleen MedCosmos Surgery - MCQDocument11 pagesSpleen MedCosmos Surgery - MCQMike GNo ratings yet
- Small Intenstine MedCosmos Surgery - MCQDocument29 pagesSmall Intenstine MedCosmos Surgery - MCQMike GNo ratings yet
- Chapter 35 NeurosurgeryDocument11 pagesChapter 35 NeurosurgeryMike GNo ratings yet
- Vascular Surgery MedCosmos Surgery - MCQDocument34 pagesVascular Surgery MedCosmos Surgery - MCQMike GNo ratings yet
- Thyroid Gland MedCosmos Surgery - MCQDocument17 pagesThyroid Gland MedCosmos Surgery - MCQMike GNo ratings yet
- Chapter 34 Pediatric SurgeryDocument11 pagesChapter 34 Pediatric SurgeryMike G100% (1)
- Chapter 1 Cell Physiology and StructureDocument4 pagesChapter 1 Cell Physiology and StructureMike GNo ratings yet
- Chapter 60: Headache: Section 10: NeurologyDocument16 pagesChapter 60: Headache: Section 10: NeurologyAnonymous Xmb6QQvRNo ratings yet
- Chapter 39 Obstetrics and GynecologyDocument3 pagesChapter 39 Obstetrics and GynecologyMike GNo ratings yet
- Chapter 36 Intracranial and Spinal TraumaDocument5 pagesChapter 36 Intracranial and Spinal TraumaMike GNo ratings yet
- Chapter 33 Plastic and Reconstructive SurgeryDocument4 pagesChapter 33 Plastic and Reconstructive SurgeryMike GNo ratings yet
- Chapter 2 Surgical NutritionDocument3 pagesChapter 2 Surgical NutritionMike GNo ratings yet
- Hopkins Medicine Review Oncology Section PDFDocument39 pagesHopkins Medicine Review Oncology Section PDFaliaaNo ratings yet
- Small Intestine 2017Document78 pagesSmall Intestine 2017yasrul izadNo ratings yet
- NCPDocument11 pagesNCPPatricia VasquezNo ratings yet
- GI BLEED - Medicine - Internal MedicineDocument11 pagesGI BLEED - Medicine - Internal Medicinezezma GamingNo ratings yet
- BD Chaurasia's Human Anatomy Volume 2Document562 pagesBD Chaurasia's Human Anatomy Volume 2Hanu KrishnaNo ratings yet
- Anatomy Quiz 2Document45 pagesAnatomy Quiz 2Upscaled100% (1)
- Case Report Superior Mesenteric Artery Syndrome ADocument5 pagesCase Report Superior Mesenteric Artery Syndrome AGunduz AgaNo ratings yet
- Gastrointestinal SystemDocument109 pagesGastrointestinal SystemRaju Mehta100% (1)
- Unknown 5Document35 pagesUnknown 5Rayane NaegelsNo ratings yet
- 1985 Václav Treitz (1819-1872) Czechoslovakian Pathoanatomist and PatriotDocument6 pages1985 Václav Treitz (1819-1872) Czechoslovakian Pathoanatomist and PatriotjohnnhekoNo ratings yet
- WORKSHOP No 3Document21 pagesWORKSHOP No 3Jennifer Mabel Almeida BrionesNo ratings yet
- 171-199 Embryologic and Anatomic Basis of Duodenal Surgery PDFDocument29 pages171-199 Embryologic and Anatomic Basis of Duodenal Surgery PDFРоман МошнягаNo ratings yet
- Gastrointestinal BleedingDocument22 pagesGastrointestinal Bleedingikumushi99No ratings yet
- Anatomy and Histology Gaster - DuodenumDocument149 pagesAnatomy and Histology Gaster - DuodenumRevila AuliaNo ratings yet
- Quiz Anatomy Part 2 of 3Document45 pagesQuiz Anatomy Part 2 of 3MedShare72% (18)
- Laparoscopic Left Colectomy Modern Technique Based On Key Anatomical Landmarks Reported by Giants of The PastDocument12 pagesLaparoscopic Left Colectomy Modern Technique Based On Key Anatomical Landmarks Reported by Giants of The PastAvidesh MahabirNo ratings yet