You might also like
- Multiple Choice Questions in Paediatric SurgeryFrom EverandMultiple Choice Questions in Paediatric SurgeryRating: 1 out of 5 stars1/5 (1)
- Multiple Choice Questions in Clinical Radiology: For Medical Practitioners and Medical StudentsFrom EverandMultiple Choice Questions in Clinical Radiology: For Medical Practitioners and Medical StudentsRating: 5 out of 5 stars5/5 (1)
- Endocrine, Head, and NeckDocument18 pagesEndocrine, Head, and NeckFarhin100% (1)
- Thyroid Notes: Key ConceptsDocument21 pagesThyroid Notes: Key ConceptsDaniel Rstom100% (1)
- Surgical Tutor MCQDocument2 pagesSurgical Tutor MCQfreeuser3100% (8)
- 1 - The Following Are Absorbable SuturesDocument15 pages1 - The Following Are Absorbable SuturesKhaled ShaheenNo ratings yet
- Mcqs Mock Exams For General Surgery Board ExamDocument7 pagesMcqs Mock Exams For General Surgery Board ExamSergiu CiobanuNo ratings yet
- Surgery 3 White Part 1Document87 pagesSurgery 3 White Part 1Håíthãm KhãtïßNo ratings yet
- 100Document17 pages100Dr-Wisam Mhmd Ali100% (1)
- Ped Surg Mcqs 2Document24 pagesPed Surg Mcqs 2abdurrahman100% (1)
- Mcqs Mock Exams For General Surgery Board ExamDocument7 pagesMcqs Mock Exams For General Surgery Board ExamSergiu CiobanuNo ratings yet
- Medcosmos Surgery: Spleen MCQDocument19 pagesMedcosmos Surgery: Spleen MCQSajag GuptaNo ratings yet
- Breast Extra Questions 601Document22 pagesBreast Extra Questions 601aminmofrehNo ratings yet
- MCH UrologyDocument20 pagesMCH UrologySholayMeiteiKangjamNo ratings yet
- T Dr. Gharama Al-Shehri: Asir Surgical Residency ProgramDocument3 pagesT Dr. Gharama Al-Shehri: Asir Surgical Residency ProgramKhaled Shaheen100% (1)
- MCQ in SurgeryDocument2 pagesMCQ in SurgeryTahirNo ratings yet
- Best operative approach for choledochal cyst MCQ quizDocument19 pagesBest operative approach for choledochal cyst MCQ quizKarem MaaliNo ratings yet
- Экз. воп для 5-го курса на англ. 200 вопросовDocument32 pagesЭкз. воп для 5-го курса на англ. 200 вопросовKumar AdityaNo ratings yet
- Breast - Dr. HammouriDocument12 pagesBreast - Dr. HammouriMohammad PropensityNo ratings yet
- Colon Cancer Risk Factors and Precancerous LesionsDocument14 pagesColon Cancer Risk Factors and Precancerous LesionsEssam ZayedNo ratings yet
- AIIMS PG Solved Paper 2001Document23 pagesAIIMS PG Solved Paper 2001shaffeque0% (1)
- Nims MCQ PaperDocument42 pagesNims MCQ PaperShankar Deshmukh50% (2)
- Surgery I MCQDocument2 pagesSurgery I MCQjoijo2009No ratings yet
- Screenshot 2023-01-22 at 19.25.23Document49 pagesScreenshot 2023-01-22 at 19.25.23Lika BukhaidzeNo ratings yet
- test1 محولDocument85 pagestest1 محولTojan Faisal Alzoubi100% (1)
- 2014 NBE ONELINER REVIEWDocument43 pages2014 NBE ONELINER REVIEWjcc50% (2)
- A. Paresthesia of The CheckDocument26 pagesA. Paresthesia of The Checkadham bani younesNo ratings yet
- Live Course Handout - CFMDocument39 pagesLive Course Handout - CFMDrMohamed Elsonosy100% (1)
- 2013 ExamDocument32 pages2013 ExamJohn M. HemsworthNo ratings yet
- Surgery McqsDocument8 pagesSurgery McqsZahra Gurmani100% (3)
- 40 Qs Uro AnsweredDocument6 pages40 Qs Uro AnsweredDr-Sulaiman Bani Abdel-rahmanNo ratings yet
- Gastric Surgery MCQDocument6 pagesGastric Surgery MCQSajag GuptaNo ratings yet
- Syrgery Mock 2Document8 pagesSyrgery Mock 2aa.No ratings yet
- MCQ SurgeryDocument19 pagesMCQ SurgeryOmar Mohammed100% (1)
- General Surgery MCQDocument190 pagesGeneral Surgery MCQلمسة مصمم100% (1)
- MCQ PancreasDocument1 pageMCQ Pancreassekhar100% (1)
- WWW Mcqsurgery ComDocument3 pagesWWW Mcqsurgery ComSajag GuptaNo ratings yet
- 017 UrologyDocument544 pages017 UrologyNashaat H. Alshawabkeh100% (1)
- Surgery Paper 1-1Document16 pagesSurgery Paper 1-1Mehak Shafi ChandioNo ratings yet
- MCQ Surgery 12-2014Document10 pagesMCQ Surgery 12-2014Dr-Shadi MeteirNo ratings yet
- Pterygomandibular space boundaries and contentsDocument8 pagesPterygomandibular space boundaries and contentsAhmad Mohammed KNo ratings yet
- Arab Board Exam Nov 2014Document5 pagesArab Board Exam Nov 2014Firyal Balushi100% (4)
- 08.blueprints Surgery 5th EdDocument70 pages08.blueprints Surgery 5th EdFadi AlkhassawnehNo ratings yet
- V.I. Vernadsky Crimean Federal University Medical Academy named after S.I. Georgievsky Chair of Surgery No1 Objectives for Intermediate Certification 6 yearDocument49 pagesV.I. Vernadsky Crimean Federal University Medical Academy named after S.I. Georgievsky Chair of Surgery No1 Objectives for Intermediate Certification 6 yearjhuiNo ratings yet
- FCPS Oct 2015-1Document9 pagesFCPS Oct 2015-1Kahkashan HameedNo ratings yet
- Breast Cancer Screening and Diagnosis GuideDocument261 pagesBreast Cancer Screening and Diagnosis Guidedocmaaas100% (2)
- 1000 Mcqs - General Medicine & Medical Emergencies Plus September 2014 McqsDocument18 pages1000 Mcqs - General Medicine & Medical Emergencies Plus September 2014 McqsSelvaArockiamNo ratings yet
- 1st Part Arab Board Exam in General Surgery, June 2007Document18 pages1st Part Arab Board Exam in General Surgery, June 2007Rahmah Shah Bahai50% (4)
- Sample Surgery QuestionsDocument98 pagesSample Surgery QuestionspandaNo ratings yet
- Matary MCQ - 2011 (WWW - Afriqa Sat - Com)Document198 pagesMatary MCQ - 2011 (WWW - Afriqa Sat - Com)Ahmed Attia100% (1)
- MCQ Explainatory Answer: According To TNM Criteria, T2: Tumor 2 CM But 5 CM inDocument3 pagesMCQ Explainatory Answer: According To TNM Criteria, T2: Tumor 2 CM But 5 CM inAbhishiktaAbhiNo ratings yet
- Urology DNB Old QuestionsDocument8 pagesUrology DNB Old QuestionssjulurisNo ratings yet
- Professionalism in Surgery QuizDocument29 pagesProfessionalism in Surgery QuizRichard100% (1)
- A) Basic Surgical SciencesDocument27 pagesA) Basic Surgical SciencessalamredNo ratings yet
- MCI FMGE Previous Year Solved Question Paper 2005 MarchDocument0 pagesMCI FMGE Previous Year Solved Question Paper 2005 MarchSharat Chandra0% (1)
- Final Surgery Exam-4 Year Medical StudentsDocument15 pagesFinal Surgery Exam-4 Year Medical Studentsmotasem alsharifNo ratings yet
- All ExamsDocument679 pagesAll ExamsYasir Saani100% (2)
- GastroenterologyDocument8 pagesGastroenterologyRumana AliNo ratings yet
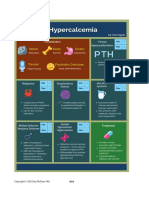
- HypercalcemiaDocument1 pageHypercalcemiaMike GNo ratings yet
- CBC DiffDocument8 pagesCBC DiffMike GNo ratings yet
- Differential Diagnosis of Neck Swellings PDFDocument3 pagesDifferential Diagnosis of Neck Swellings PDFSiddharth KatyalNo ratings yet
- Chronic Mesenteric IschaemiaDocument2 pagesChronic Mesenteric IschaemiaMike GNo ratings yet
- 2.15 Interpretasi Darah 3 Sudah Di Stabilo PDFDocument1 page2.15 Interpretasi Darah 3 Sudah Di Stabilo PDFalodiaNo ratings yet
- Neuro Dementia 2022Document5 pagesNeuro Dementia 2022Mike GNo ratings yet
- Immediate management of life-threatening abdominal problemsDocument3 pagesImmediate management of life-threatening abdominal problemsMike GNo ratings yet
- Antaomy of GITDocument5 pagesAntaomy of GITMike GNo ratings yet
- Stomach-Esophagus MedCosmos Surgery - MCQDocument39 pagesStomach-Esophagus MedCosmos Surgery - MCQMike G100% (1)
- Acute Coronary SyndromeDocument1 pageAcute Coronary SyndromeMike GNo ratings yet
- Thyroid Gland MCQ: The Ultimate QuizDocument17 pagesThyroid Gland MCQ: The Ultimate QuizMike GNo ratings yet
- Solid Visceral Injuries Solid Visceral Injuries Solid Visceral InjuriesDocument2 pagesSolid Visceral Injuries Solid Visceral Injuries Solid Visceral InjuriesMike GNo ratings yet
- Gastrointestinal Bleeding PDFDocument1 pageGastrointestinal Bleeding PDFYogi drNo ratings yet
- Classification of ShockDocument3 pagesClassification of ShockYogi drNo ratings yet
- Trauma and Burns MedCosmos Surgery - MCQDocument32 pagesTrauma and Burns MedCosmos Surgery - MCQMike GNo ratings yet
- Approach To Jundiced PatientDocument2 pagesApproach To Jundiced Patientmelinda SilalahiNo ratings yet
- Vascular Surgery MedCosmos Surgery - MCQDocument34 pagesVascular Surgery MedCosmos Surgery - MCQMike GNo ratings yet
- Chapter 34 Pediatric SurgeryDocument11 pagesChapter 34 Pediatric SurgeryMike G100% (1)
- Chapter 36 Intracranial and Spinal TraumaDocument5 pagesChapter 36 Intracranial and Spinal TraumaMike GNo ratings yet
- Spleen MedCosmos Surgery - MCQDocument11 pagesSpleen MedCosmos Surgery - MCQMike GNo ratings yet
- Chapter 35 NeurosurgeryDocument11 pagesChapter 35 NeurosurgeryMike GNo ratings yet
- Chapter 33 Plastic and Reconstructive SurgeryDocument4 pagesChapter 33 Plastic and Reconstructive SurgeryMike GNo ratings yet
- Chapter 2 Surgical NutritionDocument3 pagesChapter 2 Surgical NutritionMike GNo ratings yet
- Chapter 60: Headache: Section 10: NeurologyDocument16 pagesChapter 60: Headache: Section 10: NeurologyAnonymous Xmb6QQvRNo ratings yet
- Chapter 1 Cell Physiology and StructureDocument4 pagesChapter 1 Cell Physiology and StructureMike GNo ratings yet
- Hopkins Medicine Review Oncology Section PDFDocument39 pagesHopkins Medicine Review Oncology Section PDFaliaaNo ratings yet
- Chapter 39 Obstetrics and GynecologyDocument3 pagesChapter 39 Obstetrics and GynecologyMike GNo ratings yet
- Hopkins Medicine Review HematologyDocument35 pagesHopkins Medicine Review HematologyGuna Babu100% (1)
- Section 11 - Selected Topics in General and Internal MedicineDocument65 pagesSection 11 - Selected Topics in General and Internal MedicineMike GNo ratings yet
- CH16 Patho D&R AgamDocument29 pagesCH16 Patho D&R AgamBio CheNo ratings yet
- Paraneoplastic Syndromes Associated With LaryngealDocument15 pagesParaneoplastic Syndromes Associated With Laryngealandre halimNo ratings yet
- 1 Klöppel Vortrag GEP NET The NE System 120217Document32 pages1 Klöppel Vortrag GEP NET The NE System 120217soledad88No ratings yet
- Small IntestineDocument4 pagesSmall IntestineSiruNo ratings yet
- Diseases of The Small Intestine-1Document70 pagesDiseases of The Small Intestine-1ElvisNo ratings yet
- Small BowelDocument7 pagesSmall BowelIfeanyichukwu OgbonnayaNo ratings yet
- Gastric Neuroendocrine TumorsDocument17 pagesGastric Neuroendocrine TumorsNelsonLopezNo ratings yet
- Epidemiology, Clinical Features, and Types of Small Bowel Neoplasms - UpToDateDocument39 pagesEpidemiology, Clinical Features, and Types of Small Bowel Neoplasms - UpToDateyessyNo ratings yet
- USMLE Most Common - Adenocarcinoma - Cancer - Prova Gratuita Di 30 Giorni - ScribdDocument7 pagesUSMLE Most Common - Adenocarcinoma - Cancer - Prova Gratuita Di 30 Giorni - ScribdPaoNuNo ratings yet
- 11 AppendixDocument15 pages11 AppendixOmar MohammedNo ratings yet
- Staging of Colorectal CancerDocument47 pagesStaging of Colorectal Cancerbo gum parkNo ratings yet
- Extracted Pages From Sternberg's Diagnostic Surgical Pathology 5th EditionDocument13 pagesExtracted Pages From Sternberg's Diagnostic Surgical Pathology 5th EditionMaikka IlaganNo ratings yet
- The Flushing PatientDocument35 pagesThe Flushing Patientliu_owen17No ratings yet
- Small Bowel: Carcinoid Tumors/Neuroendocrine Tumors: Resident Teaching Conference Sept 5, 2012 Clark D. KensingerDocument32 pagesSmall Bowel: Carcinoid Tumors/Neuroendocrine Tumors: Resident Teaching Conference Sept 5, 2012 Clark D. KensingerMia DangaNo ratings yet
- Neuroendocrine TumorsDocument21 pagesNeuroendocrine TumorsAnonymous 8KN8IR1GTWNo ratings yet
- Clinical Presentation, Diagnosis, and Staging of Colorectal Cancer - UpToDate PDFDocument41 pagesClinical Presentation, Diagnosis, and Staging of Colorectal Cancer - UpToDate PDFVali MocanuNo ratings yet
- Lung CancerDocument4 pagesLung CancerÄbegail Cuanan Palang تNo ratings yet
- Astro Diagnosis VirgoDocument42 pagesAstro Diagnosis VirgoOvn Murthy100% (1)
- Canine Perineal TumoursDocument11 pagesCanine Perineal TumoursSUSANA SAM RODRIGUEZNo ratings yet
- Clinical Presentation, Diagnosis, and Staging of Colorectal CancerDocument36 pagesClinical Presentation, Diagnosis, and Staging of Colorectal CancerjjjkkNo ratings yet
- Zollinger-Ellison SyndromeDocument21 pagesZollinger-Ellison Syndromerogelio cruzNo ratings yet
- Overview Diagnosis and Treatment of GI NETSDocument73 pagesOverview Diagnosis and Treatment of GI NETSΒΑΣΙΛΗΣ ΚΟΛΙΝΤΖΙΚΗΣNo ratings yet
- TNM Classification of Malignant Tumours Website 15 MAy2011Document50 pagesTNM Classification of Malignant Tumours Website 15 MAy2011Daniel RusieNo ratings yet
- Gastrointestinal Tract PathologyDocument8 pagesGastrointestinal Tract PathologyMiguel Cuevas Dolot100% (2)
- 1.1.0.0.rel CapcpDocument15 pages1.1.0.0.rel CapcpkarimahihdaNo ratings yet
- Neuroendocrine neoplasms classification and pathologyDocument7 pagesNeuroendocrine neoplasms classification and pathologyRaniPradnyaSwariNo ratings yet
- Sesap OncologyDocument81 pagesSesap OncologyLamisNo ratings yet
- Neuroendocrine Tumor: Neuroendocrine Tumors (Nets) Are Neoplasms That AriseDocument27 pagesNeuroendocrine Tumor: Neuroendocrine Tumors (Nets) Are Neoplasms That AriseConColNo ratings yet
- Tugas Bahasa InggrisDocument14 pagesTugas Bahasa InggrisAlfin MT16No ratings yet
- Net DR MamanDocument30 pagesNet DR MamanAlma WijayaNo ratings yet