You might also like
- Therapeutinc Execise - Low Back PainDocument200 pagesTherapeutinc Execise - Low Back PainMihaela Pirosca100% (5)
- Research Report: Effect of Neck Exercise On Sitting Posture in Patients With Chronic Neck PainDocument10 pagesResearch Report: Effect of Neck Exercise On Sitting Posture in Patients With Chronic Neck Painapi-2368197No ratings yet
- Cervical Proprioception Impairment in Neck Pain-Pathophysiology, Clinical Evaluation, and Management: A Narrative ReviewDocument22 pagesCervical Proprioception Impairment in Neck Pain-Pathophysiology, Clinical Evaluation, and Management: A Narrative ReviewsoylahijadeunvampiroNo ratings yet
- With Chronic Neck Pain Effect of Neck Exercise On Sitting Posture in PatientsDocument12 pagesWith Chronic Neck Pain Effect of Neck Exercise On Sitting Posture in PatientsagungNo ratings yet
- A Comparative Study To Find Out The Effects of Capsular Stretching Over Muscle Energy Technique in The Management of Frozen ShoulderDocument50 pagesA Comparative Study To Find Out The Effects of Capsular Stretching Over Muscle Energy Technique in The Management of Frozen ShoulderjojiNo ratings yet
- Buyukturan 2017Document11 pagesBuyukturan 2017Lore OrdoricaNo ratings yet
- Falla 2004Document7 pagesFalla 2004Martín Seijas GonzálezNo ratings yet
- Short-term effects of the suboccipital muscle inhibition technique and cranio-cervical flexion exercise on hamstring flexibility, cranio-vertebral angle, and range of motion of the cervical spine in subjects with neck pain: A randomized controlled trialDocument10 pagesShort-term effects of the suboccipital muscle inhibition technique and cranio-cervical flexion exercise on hamstring flexibility, cranio-vertebral angle, and range of motion of the cervical spine in subjects with neck pain: A randomized controlled trialJonathan BaldeonNo ratings yet
- Masterclass OverviewDocument9 pagesMasterclass OverviewJavierAdalCasignaNo ratings yet
- 2055 2386 5 14 PDFDocument8 pages2055 2386 5 14 PDFrima rizky nourliaNo ratings yet
- Vikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundDocument8 pagesVikranth .G .R Lawrence Mathias Mohd Meraj Ghori: BackgroundSekar AyuNo ratings yet
- Rossi2014 PDFDocument8 pagesRossi2014 PDFDiana Magnavita MouraNo ratings yet
- Manual Therapy: Jochen Schomacher, Joachim Erlenwein, Angela Dieterich, Frank Petzke, Deborah FallaDocument9 pagesManual Therapy: Jochen Schomacher, Joachim Erlenwein, Angela Dieterich, Frank Petzke, Deborah FallaFrancisco Javier Luza RamosNo ratings yet
- The Adversity of Kinesiology Taping and The Biomechanical Effects It HasDocument8 pagesThe Adversity of Kinesiology Taping and The Biomechanical Effects It Hasapi-356704317No ratings yet
- Effect of Mckenzie Self-Therapy Protocol On Forward Head Posture and Respiratory Functions of School Going Adolescent GirlsDocument6 pagesEffect of Mckenzie Self-Therapy Protocol On Forward Head Posture and Respiratory Functions of School Going Adolescent GirlsBennat RajNo ratings yet
- Torticolis ArticuloDocument6 pagesTorticolis ArticuloCarolina Bejarano GonzalezNo ratings yet
- The Role of Muscle Strength & Activation Patterns in Patellofemoral PainDocument5 pagesThe Role of Muscle Strength & Activation Patterns in Patellofemoral Paincristian fabian perez romeroNo ratings yet
- PhysicalTreatments v4n1p25 en PDFDocument9 pagesPhysicalTreatments v4n1p25 en PDFFadma PutriNo ratings yet
- The Effect of Cervical Traction Combined With Neural Mobilization On Pain and Disability in Cervical RadiculopathyDocument5 pagesThe Effect of Cervical Traction Combined With Neural Mobilization On Pain and Disability in Cervical RadiculopathyJORGE MANÇONo ratings yet
- CallaghanDocument16 pagesCallaghanhenry EkwuemeNo ratings yet
- MPT ProjectDocument10 pagesMPT ProjectTina SanghaviNo ratings yet
- The Effect of Thoracic Spine MobilizationDocument4 pagesThe Effect of Thoracic Spine MobilizationEric SimasNo ratings yet
- Occupational Low Back Pain and The Sitting Position: Effects of Labor KinesiotherapyDocument6 pagesOccupational Low Back Pain and The Sitting Position: Effects of Labor KinesiotherapyVikas kumar SagarNo ratings yet
- Effect of Graded Plank Protocol On Core Stability in Sedentary DentistsDocument5 pagesEffect of Graded Plank Protocol On Core Stability in Sedentary DentistsVizaNo ratings yet
- Alpayci2017 2Document6 pagesAlpayci2017 2NaomiNo ratings yet
- Bauer 2019Document10 pagesBauer 2019Rafa ZalfaNo ratings yet
- Effectiveness of Isometric Neck Exercises, Stretching and Ergonomics Over Ergonomic Alone For Neck Pain in PhysiotherapistsDocument6 pagesEffectiveness of Isometric Neck Exercises, Stretching and Ergonomics Over Ergonomic Alone For Neck Pain in PhysiotherapistsAndi Riska AmirullahNo ratings yet
- Therapeutic Effects of Functional Orthodontic Appliances On Cervical Spine Posture: A Retrospective Cephalometric StudyDocument9 pagesTherapeutic Effects of Functional Orthodontic Appliances On Cervical Spine Posture: A Retrospective Cephalometric StudyJuliana ÁlvarezNo ratings yet
- Effects of Cervical Stabilisation Exercises On Respiratory Strength in Chronic Neck Pain Patients With Forward Head PostureDocument4 pagesEffects of Cervical Stabilisation Exercises On Respiratory Strength in Chronic Neck Pain Patients With Forward Head PostureMuhammad AbdullahNo ratings yet
- New Synopsis FormatDocument8 pagesNew Synopsis FormatUpadhayayAnkurNo ratings yet
- Cervical StretchingDocument5 pagesCervical StretchingSulthan PhysioNo ratings yet
- C12 Comparison of Isometric Force of The Craniocervical Flexor and Extensor Muscles Between Women With and Without Forward Head PostureDocument6 pagesC12 Comparison of Isometric Force of The Craniocervical Flexor and Extensor Muscles Between Women With and Without Forward Head PostureChing HoNo ratings yet
- Sidorkewicz 2014 - Efectos de Orientación de La Cadera en La Activación de Glúteo Medio y TFL, en Ejercicios Sin Carga de PesoDocument6 pagesSidorkewicz 2014 - Efectos de Orientación de La Cadera en La Activación de Glúteo Medio y TFL, en Ejercicios Sin Carga de PesoVanesaSandovalNo ratings yet
- 10 PDFDocument5 pages10 PDFjebabalanNo ratings yet
- Trial 1Document87 pagesTrial 1Devsya DodiaNo ratings yet
- Randomized, Controlled Clinical Trial of Treatment For Shoulder PainDocument8 pagesRandomized, Controlled Clinical Trial of Treatment For Shoulder PainRoy TukaNo ratings yet
- 7d6166c99409a11131c92f2a2febc29eDocument8 pages7d6166c99409a11131c92f2a2febc29ejsyugesh21No ratings yet
- Abhijit Dand GeetanjaliDocument8 pagesAbhijit Dand GeetanjalijunedyNo ratings yet
- Proprioception in Musculoskeletal Rehabilitation. Part 2: Clinical Assessment and InterventionDocument10 pagesProprioception in Musculoskeletal Rehabilitation. Part 2: Clinical Assessment and InterventionAlejandra VasquezNo ratings yet
- DiapositivasDocument135 pagesDiapositivasGonzalo QuiñonesNo ratings yet
- Neck Musculature Fatigue Affects Specific Frequency Bands of Postural Dynamics During Quiet StandingDocument7 pagesNeck Musculature Fatigue Affects Specific Frequency Bands of Postural Dynamics During Quiet StandingDiego Cruces OrdoñezNo ratings yet
- To Analyse The Short Term Effect of Upper Trapezius Inhibition Taping in Patients With Mechanical Neck PainDocument8 pagesTo Analyse The Short Term Effect of Upper Trapezius Inhibition Taping in Patients With Mechanical Neck PainDr. Krishna N. SharmaNo ratings yet
- Shoulder Special Tests and Rotator Cuff AssessmentDocument5 pagesShoulder Special Tests and Rotator Cuff AssessmentTomáš KrajíčekNo ratings yet
- Effectiveness of Myofascial Release and Muscle Energy Technique On Pectoralis Minor Length in Subjects With Shoulder Impingement Syndrome A Comparative StudyDocument10 pagesEffectiveness of Myofascial Release and Muscle Energy Technique On Pectoralis Minor Length in Subjects With Shoulder Impingement Syndrome A Comparative StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Article JCDRDocument4 pagesArticle JCDRMuhammad AbdullahNo ratings yet
- Does Experimental Low Back Pain Change PDocument8 pagesDoes Experimental Low Back Pain Change PJuancepaNo ratings yet
- 0Document11 pages0kang soon cheolNo ratings yet
- Thebiomechanics of Fixed AnklefootorthosesDocument9 pagesThebiomechanics of Fixed AnklefootorthosesUshsbsNo ratings yet
- Comparison of Shoulder Muscle Strengthening Exercises With The Conventional Treatment of Mechanical Neck PainDocument13 pagesComparison of Shoulder Muscle Strengthening Exercises With The Conventional Treatment of Mechanical Neck PainDr. Krishna N. SharmaNo ratings yet
- Development of A Protovol For The Management of Obstetric Erb's Palsy 2015Document6 pagesDevelopment of A Protovol For The Management of Obstetric Erb's Palsy 2015Michael HalimNo ratings yet
- 209 FullDocument23 pages209 FullMarta MontesinosNo ratings yet
- 0269215511423557Document10 pages0269215511423557Jose Maria DominguezNo ratings yet
- Johnston 2008Document9 pagesJohnston 2008Alexandre FerreiraNo ratings yet
- Effect of Myofascial Release on Neck and Arm Pain FunctionDocument9 pagesEffect of Myofascial Release on Neck and Arm Pain FunctionDonny HendrawanNo ratings yet
- Effects of Stabilization Exercise Using Flexi-Bar OnDocument5 pagesEffects of Stabilization Exercise Using Flexi-Bar OnYoh ChenNo ratings yet
- 72-Article Text-135-1-10-20190522 PDFDocument7 pages72-Article Text-135-1-10-20190522 PDFestherNo ratings yet
- 72-Article Text-135-1-10-20190522 PDFDocument7 pages72-Article Text-135-1-10-20190522 PDFestherNo ratings yet
- Tendon Neuroplastic Training Changing The Way We Think About Tendon RehabilitationDocument8 pagesTendon Neuroplastic Training Changing The Way We Think About Tendon RehabilitationfilipecorsairNo ratings yet
- Principles of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodFrom EverandPrinciples of Manual Medicine for Sacroiliac Joint Dysfunction: Arthrokinematic Approach-Hakata MethodShigehiko KatadaNo ratings yet
- The Neuromodulation CasebookFrom EverandThe Neuromodulation CasebookJeffrey ArleNo ratings yet
- Ensemble Marin OscillantDocument4 pagesEnsemble Marin OscillantRobson CarlosNo ratings yet
- PH103 Section U Recap NotesDocument54 pagesPH103 Section U Recap NotesLuka MegurineNo ratings yet
- Privilege Speech of Hon. Rex Sarabia, Member of The Sangguniang Panlungsod NG Iloilo Delivered On June 7, 2023 During The Regular Session of The Sangguniang Panlungsod NG IloiloDocument4 pagesPrivilege Speech of Hon. Rex Sarabia, Member of The Sangguniang Panlungsod NG Iloilo Delivered On June 7, 2023 During The Regular Session of The Sangguniang Panlungsod NG IloiloSelurongNo ratings yet
- Conclusion FdiDocument2 pagesConclusion FdiYo PaisaNo ratings yet
- BD-90 75 Dekanter DE-EN 905-738-1 02-16Document4 pagesBD-90 75 Dekanter DE-EN 905-738-1 02-16RasoolKhadibiNo ratings yet
- Crux v20n04 AprDocument35 pagesCrux v20n04 AprMauricioNo ratings yet
- U1L9 Student Guide (1) - 1Document4 pagesU1L9 Student Guide (1) - 1jonahNo ratings yet
- Reinforced Concrete Design Solution Manual 7th Edition PDFDocument5 pagesReinforced Concrete Design Solution Manual 7th Edition PDFEdmond Orena BautistaNo ratings yet
- Packing For DeploymentDocument2 pagesPacking For DeploymentMihaila CosminNo ratings yet
- Sanitas-Health Coach Quick Start GuideDocument26 pagesSanitas-Health Coach Quick Start GuideGabriel MuresanuNo ratings yet
- Solid Free Form:: Quilt Flatten Quilt QuiltDocument3 pagesSolid Free Form:: Quilt Flatten Quilt QuiltNaganthrakumar RamaswamyNo ratings yet
- ACS Sainsbury and Asda Merger Leaner 82Document26 pagesACS Sainsbury and Asda Merger Leaner 82FlareGBANo ratings yet
- GM Bluetooth Quick GuideDocument5 pagesGM Bluetooth Quick GuideTin_AmoNo ratings yet
- Sumalinog Teodoro Jr. LPDocument5 pagesSumalinog Teodoro Jr. LPDAITO CHRISTIAN DHARELNo ratings yet
- Herman Pardamean Hutabarat: Mechanical EngineerDocument3 pagesHerman Pardamean Hutabarat: Mechanical EngineerHerman HutabaratNo ratings yet
- Crimean-Congo Hemorrhagic Fever ReviewDocument31 pagesCrimean-Congo Hemorrhagic Fever ReviewfaizalNo ratings yet
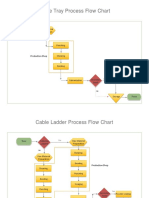
- Process Flow ChartDocument4 pagesProcess Flow Chartchacko chiramalNo ratings yet
- Internship Report FACTDocument16 pagesInternship Report FACTBennetHailinkNo ratings yet
- Edward Jumper: Willow & Lark 2017 Designed UsingDocument9 pagesEdward Jumper: Willow & Lark 2017 Designed UsingMiraNo ratings yet
- Reflective EssayDocument5 pagesReflective Essaybwood17No ratings yet
- Geometry QuotesDocument2 pagesGeometry Quotesalecksander2005No ratings yet
- Unit Ii, Lesson 4: Qualitative Research in Different Areas of KnowledgeDocument6 pagesUnit Ii, Lesson 4: Qualitative Research in Different Areas of KnowledgeJessy RoseNo ratings yet
- The Transition to Computer-Based FE Exams for Chemical EngineersDocument21 pagesThe Transition to Computer-Based FE Exams for Chemical EngineersNNo ratings yet
- Electrolytic CellDocument24 pagesElectrolytic CellIntani Mundiartasari100% (1)
- Ancient Indian WeaponsDocument25 pagesAncient Indian WeaponsjasmineNo ratings yet
- D.S.R. - 2012-2013finel PDWDocument243 pagesD.S.R. - 2012-2013finel PDWprashantlingayat25% (4)
- Pokemon Heart GoldDocument8 pagesPokemon Heart GoldPainToTheWorldNo ratings yet
- CS601 - Machine Learning - Unit 2 - Notes - 1672759753Document14 pagesCS601 - Machine Learning - Unit 2 - Notes - 1672759753mohit jaiswalNo ratings yet
- National Parks in IndiaDocument4 pagesNational Parks in IndiaVicky PandeyNo ratings yet
- STARZ Schedule 2016 12Document118 pagesSTARZ Schedule 2016 12Oscar V100% (1)