You might also like
- ACS SchematicDocument2 pagesACS Schematicswish27No ratings yet
- Chest Tube Insertion and MonitoringDocument4 pagesChest Tube Insertion and MonitoringCamille Cirineo Arensol100% (2)
- Cardiac Condition NCM 112Document10 pagesCardiac Condition NCM 112Irish Eunice FelixNo ratings yet
- DRUG-STUDY Piptaz ClindamycinDocument2 pagesDRUG-STUDY Piptaz ClindamycinJAYMIE ROSE M. MANUELNo ratings yet
- Occipitoposterior PositionsDocument49 pagesOccipitoposterior PositionsBharat ThapaNo ratings yet
- ValvularDocument2 pagesValvularJulia Rae Delos SantosNo ratings yet
- E000779 FullDocument19 pagesE000779 Fullmartina silalahiNo ratings yet
- Compartment Syndrome PDFDocument187 pagesCompartment Syndrome PDFAmayaNo ratings yet
- GynexDocument73 pagesGynexDominque RabastoNo ratings yet
- Nursing Care of Clients With Immunologic Disorders: Immune SystemDocument7 pagesNursing Care of Clients With Immunologic Disorders: Immune SystemIrish Eunice FelixNo ratings yet
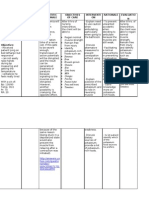
- Cues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationMiggy SikatNo ratings yet
- ORIENTATION PHASE-Undifferentiated SchizopreniaDocument7 pagesORIENTATION PHASE-Undifferentiated SchizopreniaIrish Eunice FelixNo ratings yet
- Procedure Checklist For Suctioning NCM 112 SL Done Not DoneDocument4 pagesProcedure Checklist For Suctioning NCM 112 SL Done Not DoneIrish Eunice Felix100% (1)
- MODULE Care of The Older AdultsDocument13 pagesMODULE Care of The Older AdultsIrish Eunice FelixNo ratings yet
- Post Operative MGTDocument10 pagesPost Operative MGTNatukunda DianahNo ratings yet
- Case Study Liver CirrhosisDocument64 pagesCase Study Liver CirrhosisJoseph Emmanuel Canda100% (1)
- Nurse Patient InteractionDocument14 pagesNurse Patient InteractionIrish Eunice FelixNo ratings yet
- The Dual-Zone Therapeutic Concept of Managing Immediate Implant Placement and Provisional Restoration in Anterior Extraction SocketsDocument11 pagesThe Dual-Zone Therapeutic Concept of Managing Immediate Implant Placement and Provisional Restoration in Anterior Extraction SocketsKenigal14No ratings yet
- Chlorpromazine Drug StudyDocument10 pagesChlorpromazine Drug Studyshadow gonzalezNo ratings yet
- Management of OliguriaDocument14 pagesManagement of OliguriaAhmed El-MalkyNo ratings yet
- Basilar Skull FractureDocument16 pagesBasilar Skull FractureRindahMDNo ratings yet
- DRUG STUDY (Lung Cancer)Document10 pagesDRUG STUDY (Lung Cancer)Jobelle AcenaNo ratings yet
- Nursing Care Plan On HypertensionDocument5 pagesNursing Care Plan On Hypertensionbhavana100% (1)
- annotated-COURSE TASK 2 INCREASED ICPDocument8 pagesannotated-COURSE TASK 2 INCREASED ICPJake AllegoNo ratings yet
- Patient Education: by Dr. Nadia BassuoniDocument32 pagesPatient Education: by Dr. Nadia Bassuoniاسامة محمد السيد رمضانNo ratings yet
- Bacillary DysenteryDocument32 pagesBacillary Dysenteryapi-199163990% (1)
- Concept Map 5Document2 pagesConcept Map 5api-354331689No ratings yet
- DrugStudy - CamaristaColeenMaeC (BSN III-G) (Prednisone)Document2 pagesDrugStudy - CamaristaColeenMaeC (BSN III-G) (Prednisone)Coleen Mae CamaristaNo ratings yet
- Nursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursDocument4 pagesNursing Care Plan: Subjective: During 8 Hours Nursing Management: (5) After 8 HoursRawan KhateebNo ratings yet
- Drug StudyDocument5 pagesDrug StudyDick Morgan FerrerNo ratings yet
- Pathophysiology AHS HTN EDocument1 pagePathophysiology AHS HTN Erod navalesNo ratings yet
- A Drug Study On: EpinephrineDocument16 pagesA Drug Study On: EpinephrineJay Jay JayyiNo ratings yet
- Drug AnalysisDocument10 pagesDrug AnalysisChanel BalinbinNo ratings yet
- Anxiety R:T Death ThreatDocument8 pagesAnxiety R:T Death ThreatAlfredo BaulaNo ratings yet
- NCP of Difficulty of BreathingDocument2 pagesNCP of Difficulty of BreathingMan GatuankoNo ratings yet
- Atropine Sulfate Indications: Adverse Effects: CNS: Headache, Ataxia, Contraindication: Assessment & Drug EffectsDocument4 pagesAtropine Sulfate Indications: Adverse Effects: CNS: Headache, Ataxia, Contraindication: Assessment & Drug EffectsMarie Kris Chua AbelleraNo ratings yet
- Case 1 - Pneumonia (Final)Document4 pagesCase 1 - Pneumonia (Final)Joegie ArioNo ratings yet
- I.intrODUCTION Hypertension (High Blood Pressure) Is ADocument19 pagesI.intrODUCTION Hypertension (High Blood Pressure) Is Aoril04No ratings yet
- PathophysiologyDocument2 pagesPathophysiologyKarla Karina Dela CruzNo ratings yet
- Rhabdomyolysis Case Study WeeblyDocument18 pagesRhabdomyolysis Case Study Weeblyapi-241865788No ratings yet
- IschemicheartdiseaseDocument11 pagesIschemicheartdiseaseZaimon MaulionNo ratings yet
- Rifaximin Nihms443516Document10 pagesRifaximin Nihms443516MIHAELANo ratings yet
- Case Study On Gastrointestinal Disorders PDFDocument5 pagesCase Study On Gastrointestinal Disorders PDFJude Micko Bunyi AlipitNo ratings yet
- Chronic Kidney DiseaseDocument2 pagesChronic Kidney DiseaseNi Putu Sri AndiniNo ratings yet
- RLEFand ECSDocument3 pagesRLEFand ECSPaul JacksonNo ratings yet
- NAHCO3Document2 pagesNAHCO3Krizha Angela NicolasNo ratings yet
- Cerebrovascular DiseaseDocument4 pagesCerebrovascular DiseasekathyfacaNo ratings yet
- Osteosarcoma-Ana and PhysiologyDocument4 pagesOsteosarcoma-Ana and PhysiologyNeirfla WassabiNo ratings yet
- Case Study UrtiDocument9 pagesCase Study UrtiRonica GonzagaNo ratings yet
- GENITO URINARY SYSTEM 2nd Year BSC NursingDocument8 pagesGENITO URINARY SYSTEM 2nd Year BSC NursingShreyas WalvekarNo ratings yet
- IVABRADINEDocument9 pagesIVABRADINEIvan Darío Castillo OrozcoNo ratings yet
- Introduction - MIDocument10 pagesIntroduction - MIkhimiiiNo ratings yet
- Operating RoomDocument13 pagesOperating RoomrichardNo ratings yet
- Bisgop EnxymeDocument28 pagesBisgop EnxymefjkgldjfNo ratings yet
- NCP Risk InfectionDocument1 pageNCP Risk InfectionEni RahmawatiNo ratings yet
- ZyvoxDocument1 pageZyvoxSheri490No ratings yet
- Case CHFDocument10 pagesCase CHFAgnes Erlita Distriani Patade50% (2)
- Cardiovascular Agents: Florianne E. Adlawan, R.NDocument31 pagesCardiovascular Agents: Florianne E. Adlawan, R.NadlawanflorianneNo ratings yet
- Vincristine MonographDocument9 pagesVincristine MonographcmeytasNo ratings yet
- Nursing Care Plan 1Document3 pagesNursing Care Plan 1gagandipkS100% (1)
- Retractors 2. Grasping / HoldingDocument5 pagesRetractors 2. Grasping / HoldingJanelle Dela CruzNo ratings yet
- Drug Study of Ron Steven AlvarezDocument2 pagesDrug Study of Ron Steven AlvarezAlvarez StevenNo ratings yet
- Suctioning The Nasopharygeal and Oropharyngeal AirwaysDocument8 pagesSuctioning The Nasopharygeal and Oropharyngeal AirwaysChamelli RobinNo ratings yet
- Tabalba 1-Y1-2 Lab Exercise 3Document4 pagesTabalba 1-Y1-2 Lab Exercise 3Shane V. TabalbaNo ratings yet
- Nursing Care Plan Human Response Pattern AMB/Manifestation Nursing Diagnosis Goal/ Outcome Nursing Intervention Rationale EvaluationDocument2 pagesNursing Care Plan Human Response Pattern AMB/Manifestation Nursing Diagnosis Goal/ Outcome Nursing Intervention Rationale EvaluationMarielle Chua100% (1)
- Drug StudyDocument1 pageDrug StudyMaui LopezNo ratings yet
- NCP Ineffective BreathingDocument6 pagesNCP Ineffective BreathingCuttie Anne GalangNo ratings yet
- Levemir Product Insert PDFDocument11 pagesLevemir Product Insert PDFDegee O. GonzalesNo ratings yet
- CELLULITIS NCPDocument7 pagesCELLULITIS NCPGwayne Gumangi UnsingNo ratings yet
- A. Cases of Patients Admitted in An ICU Generally, This Are The Few Common Condition of The Patients in ICUDocument5 pagesA. Cases of Patients Admitted in An ICU Generally, This Are The Few Common Condition of The Patients in ICUAngeline KimaykimayNo ratings yet
- Health Care Provider Involved in ICUDocument1 pageHealth Care Provider Involved in ICUKathleen BautistaNo ratings yet
- Resignation LetterDocument1 pageResignation LetterIrish Eunice FelixNo ratings yet
- Standard VS. Universal Precautions.Document1 pageStandard VS. Universal Precautions.Irish Eunice FelixNo ratings yet
- Felix, Irish Eunice A. BSN - 3ADocument1 pageFelix, Irish Eunice A. BSN - 3AIrish Eunice FelixNo ratings yet
- Rates of Acute Illnes in Adults by Age (/100 Population) Health StatusDocument6 pagesRates of Acute Illnes in Adults by Age (/100 Population) Health StatusIrish Eunice FelixNo ratings yet
- Cardiac Conditions Cardiac Dysrhythmias: B. Sinus BradycardiaDocument5 pagesCardiac Conditions Cardiac Dysrhythmias: B. Sinus BradycardiaIrish Eunice FelixNo ratings yet
- Disorders of The Thyroid GlandsDocument10 pagesDisorders of The Thyroid GlandsIrish Eunice FelixNo ratings yet
- Care-of-the-client-with-problems-related-to-Endocrine-system WEEK 4-6Document7 pagesCare-of-the-client-with-problems-related-to-Endocrine-system WEEK 4-6Irish Eunice FelixNo ratings yet
- Disorders of Pituitary Gland: Week 10Document13 pagesDisorders of Pituitary Gland: Week 10Irish Eunice FelixNo ratings yet
- Summary of Digestion: C. Gastrointestinal Hormones 1. GastrinDocument5 pagesSummary of Digestion: C. Gastrointestinal Hormones 1. GastrinIrish Eunice FelixNo ratings yet
- Assessment 1.3Document2 pagesAssessment 1.3Irish Eunice FelixNo ratings yet
- CUP Financial Assistance FormDocument1 pageCUP Financial Assistance FormIrish Eunice FelixNo ratings yet
- Disorders of Pituitary Gland: Week 10Document15 pagesDisorders of Pituitary Gland: Week 10Irish Eunice FelixNo ratings yet
- Assignment #6 - RizalDocument2 pagesAssignment #6 - RizalIrish Eunice FelixNo ratings yet
- Assessment 1.4Document3 pagesAssessment 1.4Irish Eunice FelixNo ratings yet
- Assessment 1.2 SalvadorDocument2 pagesAssessment 1.2 SalvadorIrish Eunice FelixNo ratings yet
- Assessment 1.3Document3 pagesAssessment 1.3Irish Eunice FelixNo ratings yet
- Letters in ResearchDocument6 pagesLetters in ResearchIrish Eunice FelixNo ratings yet
- Clinical Rotation Ii NCM 116 BSN 3 A 1Document1 pageClinical Rotation Ii NCM 116 BSN 3 A 1Irish Eunice FelixNo ratings yet
- Self AwarenessDocument1 pageSelf AwarenessIrish Eunice FelixNo ratings yet
- Cita Astals Recounts Struggles With Mental DisordersDocument2 pagesCita Astals Recounts Struggles With Mental DisordersIrish Eunice FelixNo ratings yet
- Schizoprenia: A Beautiful MindDocument4 pagesSchizoprenia: A Beautiful MindIrish Eunice FelixNo ratings yet
- Ebola Virus Disease Mers Cov Middle East Respiratory Syndrome-Related CoronavirusDocument5 pagesEbola Virus Disease Mers Cov Middle East Respiratory Syndrome-Related CoronavirusIrish Eunice FelixNo ratings yet
- Ineffective Airway Clearance Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term: IndependentDocument4 pagesIneffective Airway Clearance Assessment Diagnosis Planning Intervention Rationale Evaluation Subjective: Short Term: IndependentIrish Eunice FelixNo ratings yet
- Nurses NotesDocument1 pageNurses NotesIrish Eunice FelixNo ratings yet
- Liu 2019Document5 pagesLiu 2019Amelia Kristin SimanjuntakNo ratings yet
- Procedure Guide For Bag Technique Part 3Document2 pagesProcedure Guide For Bag Technique Part 3CrishaGarraNo ratings yet
- Common Lesser Toe Problems - Surgical Options: Claw, Hammer and Mallet ToesDocument2 pagesCommon Lesser Toe Problems - Surgical Options: Claw, Hammer and Mallet ToesJoshua RobertsNo ratings yet
- Breast LumpsDocument77 pagesBreast LumpsAliyah Tofani PawelloiNo ratings yet
- The Challenge of Kidney Damage During Interventional Cardiology ProceduresDocument6 pagesThe Challenge of Kidney Damage During Interventional Cardiology ProceduresIJAR JOURNALNo ratings yet
- Bilateral Cleft Lip ReconstructionDocument14 pagesBilateral Cleft Lip ReconstructionHusni mubarakNo ratings yet
- Capnography Selection Guide: FOR 92516, 92517, 92518 Capnography & Multigas ModulesDocument1 pageCapnography Selection Guide: FOR 92516, 92517, 92518 Capnography & Multigas ModulesfugarisaNo ratings yet
- Kasus 3Document18 pagesKasus 3Angga RistaNo ratings yet
- Concept Map Cabg PTDocument8 pagesConcept Map Cabg PTapi-607926939No ratings yet
- LASER THERAPY PresentationDocument31 pagesLASER THERAPY Presentationapi-3741769100% (5)
- QS EndotrachealIntubationDocument4 pagesQS EndotrachealIntubationChandra HalimNo ratings yet
- Aortic Arch: Left Common Carotid ArteryDocument3 pagesAortic Arch: Left Common Carotid ArteryANGELYSSA KRYSTILEE AQUINONo ratings yet
- Complications in Children With Percutaneous Endoscopic Gastrostomy (PEG) PlacementDocument5 pagesComplications in Children With Percutaneous Endoscopic Gastrostomy (PEG) PlacementHenry BarberenaNo ratings yet
- LD Implant FailuresDocument152 pagesLD Implant Failureswasim hussainNo ratings yet
- Root Canal Treatment Consent FormDocument2 pagesRoot Canal Treatment Consent FormMartina HodgsonNo ratings yet
- Cardiovascular SystemDocument18 pagesCardiovascular SystemDeep RoyNo ratings yet
- GB Cancer - Radiologic-Pathologic CorrelationDocument20 pagesGB Cancer - Radiologic-Pathologic CorrelationSamuel WidjajaNo ratings yet
- Instruments & OSCE StationsDocument3 pagesInstruments & OSCE StationsFarazNo ratings yet
- DIAGNOSTIC AND LABORATORY TESTS (Lecture) 1Document4 pagesDIAGNOSTIC AND LABORATORY TESTS (Lecture) 1sheynmalubayNo ratings yet
- Echocardiogram (Echo) : What Is An Echocardiogram?Document3 pagesEchocardiogram (Echo) : What Is An Echocardiogram?Samantha CheskaNo ratings yet
- A Project Report On: Fortis Hospital AnandapurDocument36 pagesA Project Report On: Fortis Hospital AnandapurKaran KaranNo ratings yet
- OSCE Checklist Cervical Screening SmearDocument2 pagesOSCE Checklist Cervical Screening SmearDemuel Dee L. BertoNo ratings yet
- Instructions For UseDocument20 pagesInstructions For UseMinnossNo ratings yet
- Consent For AnaesthesiaDocument34 pagesConsent For AnaesthesiaSherifMohamedNo ratings yet
- Overview of Central Venous Access - UpToDateDocument27 pagesOverview of Central Venous Access - UpToDateJAvier GarciaNo ratings yet