Professional Documents
Culture Documents
Eckstein - Et - Al-2006 - The Effect of Exercise On Human Articular Cartilage
Uploaded by
Stavros LitsosOriginal Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Eckstein - Et - Al-2006 - The Effect of Exercise On Human Articular Cartilage
Uploaded by
Stavros LitsosCopyright:
Available Formats
J. Anat.
(2006) 208, pp491–512
REVIEW
Blackwell Publishing Ltd
The effects of exercise on human articular cartilage
F. Eckstein,1 M. Hudelmaier1 and R. Putz2
1
Institute of Anatomy & Musculoskeletal Research, Paracelsus Private Medical University (PMU), Salzburg, Austria
2
Musculoskeletal Research Group, Institute of Anatomy, Ludwig-Maximilians-Universität München, Germany
Abstract
The effects of exercise on articular hyaline articular cartilage have traditionally been examined in animal models,
but until recently little information has been available on human cartilage. Magnetic resonance imaging now permits
cartilage morphology and composition to be analysed quantitatively in vivo. This review briefly describes the
methodological background of quantitative cartilage imaging and summarizes work on short-term (deformational
behaviour) and long-term (functional adaptation) effects of exercise on human articular cartilage. Current findings
suggest that human cartilage deforms very little in vivo during physiological activities and recovers from deformation
within 90 min after loading. Whereas cartilage deformation appears to become less with increasing age, sex and
physical training status do not seem to affect in vivo deformational behaviour. There is now good evidence that
cartilage undergoes some type of atrophy (thinning) under reduced loading conditions, such as with postoperative
immobilization and paraplegia. However, increased loading (as encountered by elite athletes) does not appear to
be associated with increased average cartilage thickness. Findings in twins, however, suggest a strong genetic
contribution to cartilage morphology. Potential reasons for the inability of cartilage to adapt to mechanical stimuli
include a lack of evolutionary pressure and a decoupling of mechanical competence and tissue mass.
Key words adaptation; biomechanics; cartilage; morphology; magentic resonance imaging.
Hyaline articular cartilage provides the bearing
Introduction
surface of synovial joints. This review will focus on the
Diarthrodial (synovial) joints represent important organs morphology and function of this tissue, which – for the
of the musculoskeletal system. They enable individuals sake of brevity – will simply be addressed as ‘cartilage’
to maintain posture within the gravitational field, to throughout the remainder of the text. Cartilage is unique
position their body relative to their surroundings, to as it is an avascular, aneural tissue, in which cells survive
move, and to manipulate objects around them. When for a lifetime, without intercellular connections (Hunziker
performing these tasks, joints commonly encounter et al. 2002). In particular, adult articular cartilage has
forces of several times the body weight (Bergmann et al. no other known function than maintaining mechanical
1993). Diarthrodial joints are composed of various competence. Owing to its sophisticated composition, its
structures and tissues which, from a functional point of high water content and its ability to withstand hydro-
view, act in concert. Joints are made in a manner to deal static pressurization (Ateshian et al. 1994; Mow et al. 2003),
effectively with the mechanical loads encountered over cartilage is capable of transferring enormous forces
many years of life, ideally without suffering damage relatively evenly from one subchondral bone plate to
(Mow et al. 2003; Ateshian & Mow, 2005). the other (Mow et al. 1984, 1993). Under physiological
conditions, cartilage also provides an almost frictionless
gliding surface and is thus capable of transferring these
Correspondence
loads during motion (Ateshian & Mow, 2005). In order
Professor Felix Eckstein, Institute of Anatomy & Musculoskeletal
Research, PMU, Strubergasse 21, A 5020 Salzburg, Austria. T: +43 662 to be able to meet these complex mechanical demands
44 20021240; F: +43 662 44 20021249; E: felix.eckstein@pmu.ac.at without undergoing wear and tear, articular cartilage
Accepted for publication 16 January 2006 displays unique morphological and biomechanical
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
492 The effects of exercise on human articular cartilage, F. Eckstein et al.
properties (Mow et al. 1984, 1993; Buckwalter & Mankin, The biosynthetic activity of chondrocytes has also been
1998b; Hunziker et al. 2002). These properties are yet shown experimentally to be regulated by mechanical
unmatched by any artificial material, despite consider- stimuli (Kim et al. 1995; Waldman et al. 2003). Based on
able efforts by engineers and biologists (Buckwalter & these in vitro findings, mathematical models have been
Mankin, 1998a; Hunziker, 2002). developed that explain the variable thickness of carti-
Due to a lack of non-invasive methods that allow lage between joints based on differences in mechanical
human articular cartilage to be studied directly in vivo, loading magnitude (Carter & Wong, 1988a,b, 2003;
little has been known until recently about the variability Carter et al. 1991; Wong & Carter, 2003). To date, how-
of normal cartilage morphology between subjects and ever, there has been little experimental evidence to
the factors which determine this. Even less is known support this theory on a systemic level.
about the deformational behaviour of cartilage under For this reason, the primary objective of this review
load in the intact joint in vivo. However, with quantita- is to address the question of whether (and to what
tive magnetic resonance imaging (qMRI) having become extent) articular cartilage is subject to deformation
available, data on these topics have begun to emerge. under physiological loading conditions, and what
This review will primarily focus on whether articular magnitude of mechanical signals is encountered by
cartilage is mechano-adaptive. In contrast to that of many the cartilage matrix (and thus the chondrocytes) during
other tissues, the morphology of articular cartilage (i.e. activities of daily life. The second objective to be addressed
its thickness) is determined relatively late in postnatal is whether cartilage tissue can adapt to mechanical
life, during adolescence, when endochondral ossifica- stimuli by altering its morphology (specifically its thick-
tion is complete. We do not know which specific factors ness) and composition (proteoglycan, collagen and
prohibit the calcification front from advancing to interstitial water content) to the specific mechanical
the joint surface and are responsible for the fact that conditions on a systemic level. Because most of the
a layer of cartilage is maintained at the joint surface. recent experiments on these questions have been
Given the limited number of genes available to guide performed using MRI, we will also briefly review meth-
the emergence and maintenance of the morphology odological aspects of this imaging modality in the
of various tissues and functional systems in general, it context of quantitative cartilage analysis.
is tempting to hypothesize that environmental factors,
specifically mechanics, play a pivotal role in this process.
The ability of tissues to emerge and maintain their Methodological background of qMRI
structure in accordance with specific environmental of cartilage
requirements has been termed ‘functional adaptation’
MR pulse sequences for quantitative analysis
(Lamarck, 1809; Darwin, 1872; Roux, 1881; Wolff, 1892;
of cartilage morphology
Pauwels, 1980; Carter et al. 1991; Huiskes et al. 2000).
Processes of functional adaptation have been regarded An MRI pulse sequence suitable for measuring cartilage
as occurring during the development of the central morphology quantitatively must provide a high signal-to-
nervous system (e.g. the visual cortex), internal organs noise ratio (SNR) and contrast-to-noise ratio (CNR) for
(e.g. the kidney) and in tissues with primarily mechan- accurate delineation of the subchondral bone interface
ical functions, such as muscle and bone (Wolff, 1892; and articular surface, and no significant artefacts must
Pauwels, 1980; Carter et al. 1991; Keller et al. 1992; be present. Measurements should be obtained at
Booth, 1994; Huiskes et al. 2000). Physical exercise relatively short imaging times, in order to avoid motion
has been shown to increase bone and muscle mass artefacts and to be able to measure cartilage deforma-
(e.g. body building), whereas states of inactivity or tion directly after exercise (Tieschky et al. 1997). Because
microgravity have been associated with tissue atrophy cartilage layers exhibit a mean thickness of only 1.3–2.5
(Keller et al. 1992; Booth, 1994). In bone, functional mm throughout the human knee (Eckstein et al. 2001a;
adaptation to mechanics has been mathematically Hudelmaier et al. 2001) and even less so in other joints
characterized as a cell-mediated process in which (Peterfy et al. 1995; Springer et al. 1998; Graichen et al.
osteocytes act as mechanical sensors and orchestrate the 2000, 2003; Al Ali et al. 2002), a high spatial resolution
function of other (bone-forming and bone-resorbing) is required so that a sufficient number of image points
cells through biochemical signalling (Huiskes et al. 2000). (pixels) are available to characterize the thickness of
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
The effects of exercise on human articular cartilage, F. Eckstein et al. 493
the tissue throughout the joint surface, including areas
with thin cartilage coverage. Increasing the resolution
by a factor of two in three dimensions requires acqui-
sition times to be increased by a factor of 64, if the SNR
is to be kept constant. Although there is no current
consensus on the optimal resolution for imaging
cartilage morphology, a 1.5-mm section thickness and
0.3-mm in-plane resolution has been commonly used at
a field strength of 1.5 T. The specific MR pulse sequences
that has been most frequently employed for cartilage
imaging is a T1-weighted spoiled gradient echo sequence
[FLASH = fast low angle shot (Frahm et al. 1986) or
SPGR = spoiled gradient recalled acquisition at steady
state]. This sequence (Fig. 1a,b) is available on most clinical
MRI systems and has been implemented either with
frequency-selective spectral fat-suppression by a
prepulse (Recht et al. 1993; Peterfy et al. 1994; Eckstein
et al. 1996a; Cicuttini et al. 2000) or with frequency-
selective water excitation (Hardy et al. 1998; Graichen
et al. 2000; Burgkart et al. 2001; Glaser et al. 2001). Both
techniques achieve effective fat-saturation, which is
required to provide a sufficient dynamic range of the
image contrast between the cartilage and its surrounding
tissues, and to eliminate artefacts at the subchondral
bone interface. New 3.0-T whole-body MR scanners
now make it possible to perform quantitative cartilage
imaging at higher field strength (Gold et al. 2004a,b;
Eckstein et al. 2005a,b; Kornaat et al. 2005). A recent
study has shown that measurements at 3.0 T are
consistent with those at 1.5 T, and that the precision
(reproducibility) of the measurements is slightly improved
when exploiting the higher field strength to obtain a
Fig. 1 (a) Coronal MR imaging (slice thickness 1.5 mm,
higher spatial resolution (1-mm slice thickness) at 3.0 T
in-plane resolution 0.31 mm × 0.31 mm) acquired with a T1-
compared with 1.5 mm at 1.5 T (Eckstein et al. 2005a). weighted spoiled gradient echo sequence (FLASH = fast low
One of the great advantages of MRI (e.g. in comparison angle shot; or SPGR = spoiled gradient recalled acquisition
with histology) is that consecutive slices are contiguous at steady state) with frequency-selective water excitation.
(b) Segmentation showing the medial tibial cartilage in
and spatially aligned, so that three-dimensional (3D) blue, the medial femoral condyle in yellow, the lateral tibia
parameters can be obtained that characterize cartilage cartilage in green, and the lateral femoral cartilage in red.
morphology appropriately (Fig. 2). These parameters (c) Sagittal dGEMRIC image kindly provided by Dr Deborah
Burstein, Beth Israel Deaconess Medical Center, Harvard
include cartilage volume, cartilage thickness (mean,
Medical School, Boston, MA, USA.
maximum, standard deviation), cartilage surface area
(or subchondral bone interface area) as a measure of
bone size, cartilage surface curvature (joint incon-
gruity) and others (Fig. 2). When reporting cartilage over time correspond. In cross-sectional studies, it is
volume, one must keep in mind that this parameter important to report cartilage thickness directly, or to
depends on both the cartilage thickness and the normalize cartilage volume to the joint surface/bone
cartilage surface area, and that only under conditions interface area, in order to provide meaningful results.
where the cartilage surface (or chondro-osseous inter- It has been shown, for instance, that gender differences
face area) is constant, do volume or thickness changes in joint surface areas are substantially larger than those
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
494 The effects of exercise on human articular cartilage, F. Eckstein et al.
cannot be estimated from the other – both must be
measured as separate entities.
In order to derive quantitative data from a 3D,
contiguous image set, an anatomical structure (the
articular cartilage) must first be labelled, distinguishing
it from its immediate relations (segmentation – Fig. 1b).
Owing to the relatively low contrast in some areas of
the joint surface (joint contact areas, the vicinity of
synovial folds, tendons and ligaments, repair tissue, etc.),
fully automated segmentation of cartilage is impracti-
cal from MR images. Various semi-automated image
analysis techniques have been developed to date, each
requiring different degrees of user interaction. Verifica-
tion (and some degree of correction) by an experienced
user is generally necessary on a section-by-section basis.
The inability of current computer software reliably
to identify structures in images that are evident to the
experienced human eye may seem surprising. How-
ever, if one considers the great difficulties involved in
automated speech recognition by computers, despite
the tremendous efforts made by industry, one may
appreciate the complexity of automated recognition
in intricate image pattern identification. For these
reasons, and because many slices must be acquired of
one joint surface to obtain sufficient spatial resolution,
cartilage segmentation is a time-consuming process
currently requiring several hours of human interaction
per knee data set.
After segmentation, computation of the cartilage
volume is straightforward, by simple numerical integra-
tion of the number of voxels attributed to the cartilage
during the segmentation process (Fig. 2). More sophis-
ticated algorithms are then used to determine the
cartilage thickness (Fig. 2) and joint surface area, which
must account for out-of-plane deviations of these
Fig. 2 (a) Three-dimensional reconstruction of femoral and
parameters. Computations should therefore be made
tibial cartilage from segmentations of contiguous MR images;
(b) distribution pattern of cartilage thickness in the femur, in three dimensions, independent of the original section
determined independent of the original section orientation. orientation. Extraction of cartilage surfaces also allows
The blue colour shows areas of thick cartilage, orange and red
for the determination of geometric topography and
show areas of thin cartilage.
curvature characteristics of diarthrodial joints (Ateshian
et al. 1991). Mathematical descriptions of joint surfaces
for cartilage thickness (Faber et al. 2001), a finding that and articular cartilage layers can also be applied to
is not evident from measuring cartilage volume derive computer models of human joints, by which the
alone. Also, it has been shown that cartilage thickness contact areas and surface stresses in joints may be
and cartilage surface areas are not closely associated estimated (Cohen et al. 1999, 2001) but these methods
in healthy individuals (Eckstein et al. 2001b); in other have not been yet applied to the study of the effects of
words, subjects in whom the articular cartilage occupies exercise on cartilage and joint morphology.
a larger surface area do not necessarily have thick Because these ‘global’ parameters (volume and mean
cartilage and vice versa. Thus, one of these parameters thickness for an entire cartilage plate) may be relatively
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
The effects of exercise on human articular cartilage, F. Eckstein et al. 495
insensitive to regional/focal changes that affect only uring cartilage volume, with random errors (absolute
small portions of the surface, several investigators have pairwise over- or underestimation) vs. the respective
presented techniques for displaying regional cartilage reference method of about 5–10%. Validation studies
thickness patterns (Eckstein et al. 1995, 1996a,b, 1998a; have also been performed in other joints with thinner
Sittek et al. 1996; Cohen et al. 1999, 2003; McGibbon & cartilage, such as the metacarpophalageal joint (Peterfy
Trahan, 2003) (Fig. 2). Changes over time (or differences et al. 1995), the hip (McGibbon et al. 1998), the elbow
between subjects) in regional cartilage thickness are, (Graichen et al. 2000) and the shoulder (Graichen et al.
however, difficult to detect from subjective comparison 2003).
of such thickness patterns, because only a limited number Precision errors are random errors that occur when
of thickness intervals can be displayed. In order to track repeated measurements of a parameter are taken under
local/regional thickness changes over time, registration constant conditions. Highly reproducible techniques
techniques have therefore been proposed (Kshirsagar are required to resolve small changes (i.e. cartilage
et al. 1998; Stammberger et al. 2000; Waterton et al. deformation) with statistical confidence. For qMRI of
2000; Lynch et al. 2001; Cohen et al. 2003; Raynauld cartilage morphology, the precision depends on factors
et al. 2003). With these methods, the bone interface or associated with image acquisition, and factors associ-
other anatomical landmarks from two data sets are ated with image analysis. Differences in joint position-
matched so that the thickness distribution can be com- ing are less critical than for projectional techniques
pared on a point-by-point basis. Stammberger et al. (such as radiography), because the technique is 3D and
(2000) reported a local mismatch of cartilage thickness the relevant quantitative measures are obtained from
for joint repositioning in the range of 0.5–1 mm. These reconstructions of serial images rather than from
local errors are relatively large in comparison with the projection onto one image plane. The lowest precision
absolute cartilage thickness in knee joint surfaces, but errors (CV% ∼1%) have been observed for axial pro-
this is not surprising given that an anatomically com- tocols of the patella (Eckstein et al. 2000b). Higher
plex structure is reconstructed and registered with data precision errors, by contrast, have been reported for
obtained from a limited number of sectional images. analyses of the femoral condyles in sagittal scans
(Eckstein et al. 2002b), whereas analysis of the total
femur has usually been comparable with other joint
Validation and reproducibility (precision) of
surfaces of the knee. Precision errors of computations of
quantitative analysis of cartilage morphology
the mean cartilage thickness throughout joint surfaces
The validity (accuracy) of qMRI of cartilage has been have been reported to be similar to those of cartilage
addressed in numerous studies over recent years and volume (Stammberger et al. 1999; Hyhlik-Dürr et al.
these have been carried out in unselected cadaver 2000; Burgkart et al. 2001; Eckstein et al. 2002b) as
joints, amputated joints (Peterfy et al. 1994; Cicuttini have those for quantification of cartilage surface areas
et al. 1999) or knee joint of patients undergoing total (Hohe et al. 2002; Eckstein et al. 2002b).
knee arthroplasty (TKA) (Peterfy et al. 1994; Cicuttini
et al. 1999; Burgkart et al. 2001; Graichen et al. 2004).
MR protocols for compositional cartilage imaging
TKA provides a unique opportunity for validating
quantitative measurements, as patients can be imaged In addition to measuring cartilage morphology, there
prior to surgery in vivo, and the tissue can be removed have been great efforts in using MRI to determine the
and analysed after the operation. Validation studies composition of cartilage, namely the glycosaminoglycan
have been carried out in comparison with various (GAG) content, collagen content and orientation, and
reference methods, namely water displacement of the interstitial water content. Attempts to determine
surgically retrieved tissue (either direct or by employing the concentration of GAG include imaging of fixed
Archimedes’ principle), anatomical sections obtained charge density by using an intravenous injection of
with high-precision band saws, computer tomography the charged clinical MRI contrast agent Gd(DTPA)2–. If
arthrography, A-mode ultrasound (not to be confused Gd(DTPA) 2– is allowed to penetrate into cartilage,
with clinical B-mode ultrasound), and stereophoto- a process that has been estimated to last for about
grammetry. Most of these comparative studies have 90 min after injection, it distributes inversely with the
reported close agreement between methods of meas- GAG concentration (Fig. 1c). Because full penetration
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
496 The effects of exercise on human articular cartilage, F. Eckstein et al.
is required, the technique has been termed delayed the magnitude of the joint loads during normal (partic-
gadolinium enhanced MRI of cartilage (dGEMRIC) ularly dynamic) exercise is unknown. Moreover, the effect
(Gray et al. 2004). When tissue is placed in a magnetic of boundary conditions (e.g. non-linear contact con-
field, magnetic moments of the protons are aligned, ditions between incongruous joint surfaces, presence
resulting in a net magnetic moment. This equilibrium is of the synovial fluid) is difficult to take into account. In
then disturbed by transmitting another magnetic field vivo data on the deformation of articular cartilage are
at the same frequency as the rotations of the protons necessary, however, in a number of areas. (1) Cartilage
for a very short time. The return to equilibrium of the deformational behaviour depends on the biochemical
magnetic moments after this pulse is strongly affected composition of the tissue and may potentially represent
by molecular interactions of the nuclei with their sur- a more sensitive surrogate marker of early osteoarthritis
roundings and can be exploited for imaging cartilage than morphological endpoints such as cartilage volume,
composition (Burstein & Gray, 2003). Two time constants thickness or joint space narrowing (Burstein et al. 2000).
are relevant in this context, the longitudinal (T1) (2) Knowing the magnitude of strain in the target tissue
and transverse relaxation time (T2). When probing T1 is important when designing cartilage transplants.
in cartilage in the presence of fully penetrated Gd(DTPA)2– Artificial cartilage can then be designed in a way to be
(dGEMRIC), one can estimate the GAG content of the able to withstand these strains ex vivo so that cartilage
tissue (Fig. 1c). dGEMRIC has been validated in basic transplants can be expected to meet mechanical require-
science and clinical studies through comparison with ments in vivo. (3) The magnitude of in vivo deforma-
biochemical and histological measures of GAG (Bashir tion of articular cartilage is related to the magnitude of
et al. 1997, 1999; Tiderius et al. 2003; Williams et al. 2004). mechanical stimulation experienced by the chondro-
Another technique that has been successfully explored cytes, which is known to affect their biosynthetic
is T2 mapping (Mosher & Dardzinski, 2004). T2 can be activity (Sah et al. 1989; Urban, 1994; Kim et al. 1995).
obtained without the presence of a contrast agent, Knowledge of cartilage deformation in vivo may thus
but cannot be attributed to a single constituent of serve as an important guideline of how to stimulate cells
cartilage composition. T2 has been shown to provide a optimally in tissue culture and cartilage transplants,
quantitative measure of cartilage interstitial fluid and and also how to use mechanical signals to stimulate
its interaction with the solid components of the extra- cartilage in situ.
cellular cartilage matrix, in particular with collagen
content and orientation, whereas there is little to no
In vitro studies of the intact femoro-patellar joint
sensitivity to changes in GAG concentration (Mosher &
Dardzinski, 2004). Spatially resolved cartilage T2 maps Cartilage deformation during loading cannot be readily
have been shown to be correlated with the regional investigated with MRI, because it is difficult to apply
water content of the deep and mid zones of cartilage relevant loads to the joint of a living person within the
(Lusse et al. 2000) but recent data suggest that collagen MRI scanner, and to keep the joint in a constant position
fibre anisotropy is the dominant factor related to relative to the coil at the same time. Note that, given
regional differences in T2. T2 of the superficial zone an in-plane resolution of 300 µm, even very tiny move-
of cartilage was shown to change with aging (Mosher ments of the limb make it impossible to obtain an
et al. 2004). accurate measure of cartilage thickness. To overcome
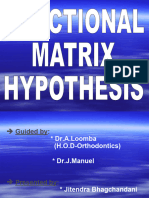
this limitation, one group (Herberhold et al. 1998) con-
structed a non-metallic compression apparatus capable
Short-term effects of exercise on articular
of generating loads of up to 1500 N (Fig. 3) for studying
cartilage (deformational behaviour)
patellofemoral compression in a clinical MRI scanner.
Although the mechanical properties of articular cartilage The time-dependent deformation of the patellofemo-
have been thoroughly studied under in vitro conditions ral cartilage was studied in situ over a 4-h period under
(Mow et al. 1993, 2003), until recently there have been continuous static loading with 150% body weight, with
little data on the magnitude of the in situ cartilage the joint capsule being kept fully intact (Herberhold
deformation in intact joints, and there have been no et al. 1999). Analysis of cartilage deformation in the
data for in vivo loading conditions. This information central 2D slice revealed a mean reduction of 44 ± 15%
cannot be extrapolated from in vitro studies, because of the initial thickness in the patella, and a cartilage
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
The effects of exercise on human articular cartilage, F. Eckstein et al. 497
Fig. 3 The non-metallic compression
apparatus that fits into the extremity coil
of a clinical MRI scanner is capable of
generating loads of up to 1500 N using
a pneumatic pressure piston, and can
accommodate a human patellofemoral
joint at a 60° flexion angle. The patella
and pressure piston are guided between
Delrin trays, so that the cartilage
deformation could be monitored using
a fast two-dimensional MR imaging
sequence with an acquisition time of
< 1 min. Images on the right show the
status of the femoropatellar cartilage
before compression (t = 0 min) and after
120 min and 240 min of compression,
respectively.
thickness change of 30 ± 10% in the femoral trochlea The patellar cartilage volume (as measured over
after 3.5 h of static loading with 150% body weight the entire patella, but not in the central 2D slice) was
(Figs 3 and 4a). The deformation of the patellar reduced by 8 ± 5% after 14 min and by 29 ± 3.2% after
cartilage exceeded that of the trochlea, this being 3.5 h of loading (Fig. 4c). After 3.5 h, deformation
consistent with the differences in cartilage mechanical had not yet ceased and equilibrium had not yet been
properties reported between the patella and femoral reached, because the load-bearing area continued to
trochlear (Froimson et al. 1997). The maximal cartilage increase proximally and distally from the site of central
deformation observed was 57 ± 15% in the patella contact, in which equilibrium had been reached (see
and 44 ± 7% in the trochlea (Herberhold et al. 1999). above). Given an interstitial water content of cartilage
Cartilage thickness decreased in an approximately of about 80%, these data suggest that more than 50%
exponential manner and cartilage deformation ceased of the interstitial fluid was displaced from the patellar
in the central slice after 3.5 h (equilibrium). Interest- cartilage matrix during 3.5 h of static compression.
ingly, however, only a small fraction of the final (3.5 h) Based on the assumptions that the solid matrix is incom-
deformation was reached during the first 1 min of pressible (Mow et al. 2003), that all volume changes are
static loading (3% cartilage thickness change in the due to fluid flow and that during compression the fluid
patella and 1.3% in the trochlea), and the deformation flow will occur throughout the articular surface into
was still of little magnitude after ∼8 min of loading the joint cavity, the rate of interstitial fluid loss from
(11% cartilage thickness change in the patella and 9% the matrix was estimated to be 1.3 (± 0.5) mm3 min−1
in the trochlea; Fig. 4b). This revealed that only about per cm2 surface area (fluid flux = 0.217 ± 0.083 µm s−1)
4–7% of the final (near equilibrium) deformation is for the first 14 min of loading, and 0.22 (± 0.04) mm3
reached with the first 1 min of loading, and that only (min cm2)−1 (0.037 ± 0.007 µm s−1) in the terminal phase
25 –30% of this final deformation is reached during the of the experiment (> 120 min). Note that these values
first 8 min of load application. provide only a mean throughout the joint surface and
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
498 The effects of exercise on human articular cartilage, F. Eckstein et al.
that the flux is assumed to be highly variable through-
out it during the compression experiment. Also, the
thickness changes were found to be highly inhomoge-
neous throughout the joint surface and load-bearing
area, with the maximal deformation (the lateral
patellar facet) being identical to the site of the maximal
cartilage thickness. An experiment using pressure-
sensitive FUJI film, conducted in the same specimens
after imaging, showed pressure maxima of 3.6 ± 1.3 MPa,
in the lateral patellar facet, the pressure distribution
being very similar to the pattern of cartilage deformation.
In one of the specimens imaging was continued after
the 3.5-h experiment and after removal of the load.
The cartilage displayed almost full recovery (98%) after
approximately 4 h. The rate of fluid re-uptake by the
cartilage matrix was 0.9 mm3 (min cm2)−1 (0.15 µm s−1)
within the first 14 min of recovery, and 0.14 mm3 (min
cm2)−1 (0.023 µm s−1) in the terminal phase of the recovery
period.
It may appear surprising that cartilage deforms so
little for the first few minutes under high loads. How-
ever, the primary function of cartilage is not to absorb
energy through deformation (a function that is performed
by the muscles, the tendons and the joint as an organ),
but to distribute the load equally to the subchondral
bone plate and to provide minimal friction during
motion. This function can be compared with the inflated
tyre of a bike, which should not deform, in order to
avoid damage to the wheel (the subchondral bone)
and to provide minimum resistance during rolling. The
energy absorption, by contrast, is provided by a spring
(the joint, with its tendons and muscles), and energy
absorption is warranted by controlled joint movement
and negative acceleration in it. It may be argued that
deformation is higher when high-impact loading occurs,
but it should be remembered that cartilage consists of
80–90% interstitial fluid, which is incompressible, and
which has little time to escape from the load-bearing
area in high-impact loading. This can be appreciated
Fig. 4 In situ compression of patellofemoral cartilage using
the compression device shown in Fig. 3. (a) Graph showing the when landing on one’s front or back on water after a
mean reduction of thickness in a central axial 2D slice through jump from a 10-m tower. Given that the water has little
the patellofemoral contact zone over 3.5 h of static loading
time to escape under these high-impact conditions, little
with 150% body weight; (b) only a small fraction of the final
thickness is reached during the first few minutes of static energy absorption is provided, and this even more so in
loading; (c) patellar cartilage volume (measured over the the cartilage, in which the fluid is bound to the matrix.
entire patella) was reduced by approximately 30% after 3.5 h
of loading.
In vivo deformation of the patellar cartilage
In order to determine in vivo cartilage deformation
shortly after exercise, we have quantified the cartilage
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
The effects of exercise on human articular cartilage, F. Eckstein et al. 499
volume of healthy volunteers after 1 h of physical rest
(no weight-bearing in the scanner) and then 3–7 min
after 50 knee bends (Eckstein et al. 1998b). Note that so
far it has been impossible to determine cartilage defor-
mation reliably during loading in vivo for the reasons
mentioned in the first paragraph, and that it also can-
not be determined immediately after the exercise, as
some time is required to reposition the patient in the
magnet, to obtain a preliminary view for slice position
and alignment, and actually to acquire the 3D image
data. After the knee bends we observed a reduction
in cartilage volume (compression) in the patella of
2.4–8.6% (mean = 6.0%) (Fig. 5) (Eckstein et al. 1998b).
Note that this is the mean deformation across the
entire patellar cartilage and that a certain amount of
inhomogeneity may be present, with some areas encoun-
tering higher and some lower deformation (see below).
When asking the same subjects to perform 100 knee
bends (Eckstein et al. 1999), the level of deformation
was of 2.4 – 8.5% (mean = 5.0%) and was not signific-
antly different from that after 50 knee bends (Fig. 5).
We then examined the time required for recovery of
the cartilage under non-weight-bearing conditions
(Eckstein et al. 1999). A period of 45 min was required
to compensate approximately 50% of the deformation
observed after knee bends and a period of 90 min to
attain the pre-exercise volume before the knee bends
(Eckstein et al. 1999) (Fig. 5). The fluid re-uptake appeared
to be almost linear throughout the observation period, Fig. 5 Patellar cartilage deformation after six sets of 50 knee
bends at 15-min intervals (top), and during recovery after
and the average fluid flux during the recovery period
100 knee bends (bottom).
was estimated to be approximately 0.027 µm s−1. This
compares well with the values observed during terminal macromolecular composition of the cartilage occurred
recovery after long-term static loading (Eckstein et al. following exercise.
1999) (see above). We demonstrated further that When comparing static (90° squatting for 20 s) with
multiple sets of 50 knee bends, with intervals of 15 min of dynamic loading (30 deep knee bends to 120°), dif-
rest in between, maintained the level of deformation ferences were found both in the magnitude and in the
measured after the first set of knee bends (around pattern of cartilage deformation throughout the joint
5–6%), but did not lead to further cartilage deforma- surface (Eckstein et al. 2000a). The reduction in cartilage
tion beyond this value (Eckstein et al. 1999) (Fig. 5). thickness after 30 knee bends (5.9 ± 2.1%) was not less
Liess et al. (2002) studied 20 healthy volunteers after than after 50 or 100 knee bends, with the range being
performing 60 knee bends. MR images of the patellar 2.9–9.6%. After static loading, we also observed a
cartilage were acquired immediately following exercise significant reduction of the patellar cartilage volume
and then after 45 min of rest. Within 45 min of loading, of 4.7 ± 1.6% (range 2.4–6.5%). The maximal deforma-
patellar cartilage volume increased by 5.4 ± 1.5%. At tion was observed in the central aspect of the lateral facet,
the same time, T2 maps of the patellar cartilage were which is also the site of maximal cartilage thickness
acquired. During the 45-min recovery period, T2 increased (Fig. 6). The cartilage volume changes recorded after
by 2.6 ± 1.0% (P < 0.05). The authors concluded that dynamic loading were significantly higher than those
small physiological changes in the water content of after static loading (P < 0.05), probably because the
patellar cartilage and concomitant changes of the patellar joint surface area involved in load-bearing is
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
500 The effects of exercise on human articular cartilage, F. Eckstein et al.
Fig. 6 In vivo deformation patterns of
patellar cartilage after different
physiological activities (see text). A
posterior view onto the right patellar
cartilage surface (proximal pole of the
patella on top, medial side on the left):
average of differences in cartilage
thickness before and after various
activities averaged over 12 volunteers.
Red and orange colours show areas of
high deformation, blue colour areas of
little deformation.
much higher for dynamic exercise with a wide range of (5) cycling for 10 min on a training bike at a frequency
knee angles being taken, and the correlation coefficient of 80 Hz (Fig. 6). The cartilage deformation of the patella
for deformation after the two activities was r = 0.69 (P < was 5.9 ± 2.1% after the 30 knee bends, 2.8 ± 0.8% after
0.05). In a recent paper we compared several activities walking, 5.0 ± 1.3% after running and 4.5 ± 1.6% after
(Eckstein et al. 2005c), including (1) 30 deep knee bends, cycling (Fig. 6), with all changes being significant at P <
(2) static loading (see above), (3) normal walking at 0.01. In order to investigate the pattern of cartilage defor-
ground level for 5 min, (4) running 200 m and walking mation throughout the patella as well, we employed
up and down 54 steps over a total time of 4 min, and the matching algorithm described by Stammberger et al.
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
The effects of exercise on human articular cartilage, F. Eckstein et al. 501
the cartilages are thinner and the precision errors (CV
2–3%) are higher than for patellar cartilage. Waterton
et al. (2000) studied volunteers in the morning and then
after a day of mainly standing activity. They reported
no change in overall femoral cartilage volume and
thickness but cartilage thinning in the femorotibial
contact zones. They observed an increase in thickness
in areas of the femoral condyles and trochlea that were
supposedly not involved in loading during standing,
and they hypothesized that this resulted from negative
Fig. 7 Scheme showing the state of patellar cartilage intra-articular pressure during joint extension by the
deformation (cartilage thickness change) during normal daily quadriceps muscles. It was alternatively suggested that
activity and the physiological window of cartilage interstitial fluid was displaced from load-bearing to
deformation between non-weight-bearing conditions and
heavy exercise, such as deep knee bends.
non-load-bearing areas within the cartilage. To inves-
tigate femorotibial cartilage deformation after more
intense activities, we acquired two coronal scans after
(2000). Cartilage thickness difference maps for the 12 a period of 60 min of physical rest in a first session (in
volunteers were displayed using grey value coding. order to reduce the precision error involved), and then
Averages of the deformation patterns of the 12 volunteers one coronal scan after 30 knee bends in 12 healthy
(for each activity) were then derived, in order to reduce subjects (Eckstein et al. 2005c). Other activities investig-
the noise. They were then recoded in colour intervals, ated in the same volunteers included 12 knee bends
in order to visualize better the effects of short-term performed on one leg only, 2 min of static loading of
exercise throughout the patellar surface (Fig. 6). During the femorotibial joint of one leg at 15° flexion, and ten
squatting and walking, changes were confined to limited jumps from a chair (40 cm height) onto one leg (Fig. 8).
regions of the patellar surface, consistent with the con- No significant change in cartilage volume was observed
tact areas involved for these activities (Hehne, 1990). in femorotibial cartilage after two-legged knee
Activities where there was a larger range of knee bends (except for the lateral tibia) or one-legged knee
motion (running including stairs, cycling, knee bends) bends (Eckstein et al. 2005c). Significant changes were
involved a more widespread area of deformation. observed in the medial and lateral tibial cartilage after
When measuring patellar cartilage of volunteers in the impact loading (jumps from 40 cm height), but not in
evening after a day of normal activity (no period of rest the medial or lateral femoral condyle (Fig. 8). Changes
prior to imaging) and then after spending the night with borderline significance were found in the medial
sleeping (and without weight-bearing) in the MRI unit, tibial and lateral femoral condyles after the static
Sitoci et al. (2003) found that cartilage volume increased loading exercise (Eckstein et al. 2005c).
significantly, but only by 2.2% overnight. This finding When investigating seven female runners after
is consistent with that of a 3% deformation observed performing a full distance marathon under competi-
when walking after a period of non-load-bearing. In tive conditions (Boston marathon 2005), no significant
summary, these data demonstrate that during normal deformation of tibiofemoral or patellofemoral carti-
daily activity (walking etc.), the patellar cartilage is at lage was observed 90 min after the race (Kunz et al.
a state of approximately 2–3% average compression 2005). These findings do not exclude the possibility
vs. non-weight-bearing conditions, and that intense that some deformation may have been present imme-
exercise may add another 2–3% of average compres- diately after the race, but these data show that no pro-
sion on top of those encountered during normal daily longed deformation occurs after a very intense activity
activity vs. non-weight-bearing conditions (Fig. 7). involving several thousand load cycles. In the same
sample, Williams et al. (2005) found a decrease of the
dGEMRIC index in the medial and lateral femoral con-
In vivo deformation of femorotibial cartilage
dyles 1 day after the race (up to 18%), followed by a
Femorotibial cartilage deformation is more challeng- return towards pre-race values at 1 week and recovery
ing to investigate compared with the patella, because to near pre-race values by 6 weeks post-race. The
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
502 The effects of exercise on human articular cartilage, F. Eckstein et al.
tibial cartilage, by contrast, displayed no change in the
dGEMRIC index at day 1; but a significant increase at
week 1. Six weeks after the race, values had returned
to pre-race levels. Because no change in cartilage
thickness was observed immediately after the race
(Kunz et al. 2005) and therefore also is unlikely to have
occurred 1 day, 1 week or 6 weeks after the race, these
data indicate that there may be a loss of GAG after
intense physical activity, and that this may evoke a
biological response that increases cell metabolism and
production of GAG.
Mosher et al. (2005) obtained T2 maps of weight-
bearing femoral and tibial articular cartilage in young
healthy men before and immediately after 30 min of
running. They found no statistically significant change
in T2 profiles of tibial cartilage, but a significant decrease
in T2 of the superficial 40% of weight-bearing femoral
cartilage after exercise. The authors concluded that
these results support the hypothesis that cartilage
compression results in greater anisotropy of superficial
collagen fibres.
In vivo deformation of cartilage as related to cartilage
mechanical properties
As in vivo cartilage deformation is a complex event that
is determined by (1) the load applied to the joint, (2)
the load distribution within the joint during the specific
activity and (3) cartilage mechanical properties, and
because measurements of it are additionally confounded
by precision errors, one cannot equate the deforma-
tional behaviour of cartilage directly with its material
properties. However, in a study of cartilage recovery
after 100 knee bends (Eckstein et al. 1999) we found
that the fluid flux during recovery (no weight bearing)
was highly correlated (r = 0.87) with the magnitude of
deformation observed after the knee bends. Because
the recovery was found to be approximately linear
throughout the 90-min observation period, and because
no external forces acted on the joint during the recovery
period, it is reasonable to assume that the individual
fluid flux throughout the surface observed during
cartilage recovery after knee bends reflects the specific
mechanical properties of the cartilage in this individual.
Fig. 8 Graphs showing the magnitude of tibiofemoral The high correlation of the flux during recovery with
cartilage deformation (change in mean thickness) and level of the magnitude of deformation after knee bends
significance after various types of activities: MT = medial tibia;
suggests therefore that MRI-based measurement of
cMF = central medial femur (condyle); LT = lateral tibia;
cLF = central lateral femur (condyle). in vivo deformation gives at least some insight into the
individual mechanical properties of the cartilage in vivo.
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
The effects of exercise on human articular cartilage, F. Eckstein et al. 503
When investigating non-osteoarthritic subjects aged three world champions and one Olympic medallist. The
50 –75 years, Hudelmaier et al. (2001) found a smaller reduction in patellar cartilage volume after 30 knee
degree of patellar cartilage deformation than in younger bends was 4.1 ± 2.6% in the non-athletic participants,
subjects aged 20–30 years. A potential explanation 2.9% ± 1.9% in the weightlifters and 3.9 ± 1.8% in the
for the reduced deformation is that older individuals bobsleigh sprinters. Although there was a trend for the
exhibit different motor strategies (Papa & Cappozzo, weightlifters to display a lower magnitude of deforma-
2000) and subject their knee joints to smaller loads tion, the difference between the groups was not statis-
during knee bending. It has, however, been demonstrated tically significant.
that due to non-enzymatic glycolisation, collagen cross- To date, there are no data on in vivo cartilage deforma-
links increase with aging (pentosidine), both in animals tion in osteoarthritic patients, and obviously there are
and in humans (Takahashi et al. 1995; Brama et al. 1999), ethical problems in subjecting patients with knee
a process that has been found to render the cartilage pain to intense exercise protocols. However, cartilage is
matrix stiffer than in the young (Chen et al. 2002; known to become more compliant (less stiff) with osteo-
Verzijl et al. 2002; Saudek & Kay, 2003). The finding of arthritis, and standardized in vivo loading protocols
reduced cartilage deformation after exercise in the may eventually be used clinically to evaluate functional
50 –75-year-old subjects therefore lends support to the properties over the course of joint disease, or even to
concept that changes in cartilage mechanical properties study the effects of different types of therapy on carti-
can be detected in vivo, by examining deformational lage quality (Burstein & Gray, 2003).
behaviour of cartilage after exercise. No difference in
cartilage deformational behaviour between women
and men was observed in this study (Hudelmaier et al. Long-term effects of exercise on articular
2001), either in the 20 –30-year-olds or in the 50–75- cartilage (functional adaptation)
year-olds.
Intersubject variability, side differences and
In one of the studies previously mentioned (Eckstein
correlation with anthropometric measures
et al. 2005c) we tested the hypothesis that the in vivo
deformation of patellar cartilage is smaller in pro- Numerous studies have reported a high degree of
fessional athletes than in non-athletic volunteers. This intersubject variability in cartilage volume, thickness
hypothesis was based on the observation that cartilage and surface areas of the human knee (Jones et al. 2000;
composition and mechanical properties functionally Eckstein et al. 2001a,b; Hudelmaier et al. 2001, 2003;
adapt to mechanical stimulation in some animal experi- Cicuttini et al. 2002, 2003; Burgkart et al. 2003), and
ments (reviewed by Vanwanseele et al. 2002b), whereas also in other joints of the body (Springer et al. 1998;
another study showed that continuous training of Graichen et al. 2000, 2003; Al Ali et al. 2002). Hudel-
dogs did not alter the compositional or mechanical maier et al. (2003) showed that muscle cross-sectional
properties of articular cartilage, even though the areas (MCSAs) of the thigh and calves can be reproduc-
animal had been training throughout life (Newton ibly measured using a spin echo magnetic resonance
et al. 1997). These different outcomes of animal models sequence and are more highly correlated with cartilage
may be potentially explained by differences in suscept- morphology than body height or body weight. Also,
ibility to mechanical stimuli at different levels of skeletal MCSAs contributed significant, independent informa-
maturity. However, there is as yet no convincing evidence tion in multiple regression models, with cartilage
that human cartilage composition can be changed by morphology as the dependent varaible and body weight
mechanical stimulation, and in particular changed and height as independent variables. These models
to a degree that it affects its in vivo deformational predicted approximately 75% of the variability in
behaviour. We therefore compared patellar cartilage cartilage volume (Hudelmaier et al. 2003). No signifi-
deformational behaviour in 14 men who had never cant differences were found in knee cartilage mor-
performed regular training of muscle strength with phology of the left and right limbs of volunteers, and
seven professional weightlifters, and seven professional the left–right differences were substantially lower
bobsleigh sprinters. The weightlifters were regional than the intersubject variability. This applied to carti-
champions and included one world champion. The lage volume, thickness and surface area (Eckstein et al.
bobsleigh sprinters were national finalists and included 2002c). The side differences were not associated with
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
504 The effects of exercise on human articular cartilage, F. Eckstein et al.
lower limb dominance, i.e. subjects with dominance for a significant linear decrease in knee cartilage thick-
of the right lower limb did not display systematically ness both in the presence and in the absence of osteo-
higher cartilage volume, thickness or surface areas arthritis. These findings were, however, confined to
on that side. However, side differences in MCSAs were the site of most frequent femorotibial contact of the
moderately correlated with side differences in cartilage lateral and medial femoral condyle but did not apply to
volume, thickness and surface areas, i.e. subjects with the patella, the tibia or the posterior aspects of the
higher thigh MCSAs on the right tended to have higher femoral condyles. Hudelmaier et al. (2001) examined
cartilage volume, thickness and joint surface areas in men and women aged 50–75 years with no history of
the right knee (Eckstein et al. 2002c). knee pain, trauma or surgery. In the patella, they found
Cicuttini et al. (1999) reported sex differences of no significant difference in cartilage thickness com-
cartilage volume in adults, and Jones et al. (2000) in pared with men aged 18–40 years (−6%), but a signific-
children and adolescents. The sex differences remained antly lower thickness (−12%; P < 0.05) compared with
significant after adjusting for age, body weight, height women aged 18–40 years. Interestingly, women also
and femoral (condylar) bone volume. Faber et al. (2001) displayed a larger decrease of the quadriceps cross-
also observed significant sex differences of cartilage sectional area with age than men. For other joint surfaces
volume in the medial tibia (+43% in men) and lateral of the knee they estimated the amount of cartilage
tibia (+47%), and smaller (albeit significant) differences thinning with age to be approximately 4% per decade
in the patella (+20%) and femur (+27%). It was shown, and rates were similar for both sexes (Hudelmaier et al.
however, that gender differences in cartilage volume 2003).
originated mainly from differences in the joint surface
area size (total knee = +23% in men; P < 0.01), but to a
Reduced loading conditions
lesser extent from differences in cartilage thickness
(total knee = +8% in men; difference not statistically As stated above, mechanical stimuli are known to
significant) (Faber et al. 2001). Eckstein et al. (2001a) represent potent regulators of muscle and bone tissue
reported that after matching men and women with mass. Animal studies have suggested that cartilage
identical body weight and height, men did not display thickness decreases during immobilization but investiga-
significantly higher cartilage thickness than women, tions in animals with increased levels of exercise have
but still had significantly larger joint surface areas. produced inconclusive and partly contradictory
This suggests that even when being matched for body results (Helminen et al. 1992; Newton et al. 1997; for
height and weight, women have smaller knee joint sur- a recent review see Vanwanseele et al. 2002b). In a
faces than men. Eckstein et al. (2004) further examined cross-sectional study, Vanwanseele et al. (2002a) exam-
whether gender differences in joint surface areas of ined the knee joints of paraplegic patients at 6, 12 and
the ankle joint were smaller than in the knee (based 24 months after injury and found the cartilage thick-
on the notion that women suffer more often from knee ness to be significantly reduced in relation to healthy
osteoarthritis than men, but men more often from subjects of the same sex. The authors confirmed a
osteoarthritic changes in the ankle). However, the authors reduction in cartilage thickness in paraplegic patients
found the sex differences to be similar for both joints. in a 12-month longitudinal study (Vanwanseele et al.
A source of controversy has been whether cartilage 2003), in which they reported an annual reduction in
thinning occurs during the normal aging process cartilage thickness of > 10% in all compartments of the
(possibly as a result of reduction in mechanical loading) knee, whereas no significant changes of cartilage
or whether the decrease only affects people with thickness were found in the shoulder (Vanwanseele
arthritis. In human specimens, Meachim (1971) found et al. 2004). Hinterwimmer et al. (2004) recently showed
no significant decrease of cartilage thickness in the that even during short-term reduced loading condi-
human shoulder with age, whereas in the patella tions (7 weeks of partial weight bearing at the knee,
Meachim et al. (1977) observed cartilage thinning, in after a surgical intervention at the ankle) there was a
particular in women over the age of 50 years. These significant degree of cartilage thinning (Fig. 9). Partial
changes were attributed to osteoarthritis rather than unloading was associated with an average reduction of
to aging as such. Karvonen et al. (1994) concluded from the quadriceps muscle cross-sectional area (as measured
local measurements in MR images that age accounted with MRI) of 11% (Fig. 9), but no significant increase
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
The effects of exercise on human articular cartilage, F. Eckstein et al. 505
alterations of the cartilage, specifically the proteo-
glycans, that may jeopardize its morphological integrity
and mechanical competence (Haapala et al. 1999).
Hudelmaier et al. (2001) examined a single volunteer
after 6 weeks of complete non-load-bearing and restric-
tion of knee joint motion to 0–30° of flexion. They
found a 14% lower patellar cartilage thickness on the
immobilized side, but no side differences in tibial carti-
lage morphology. At the same time, side differences in
quadriceps cross-sectional area amounted to 36%
after immobilization. During a 24-month remobilization
period with intensive physiotherapy and weight train-
ing over the first 7 months, side differences in patellar
cartilage thickness and quadriceps cross-sectional
area reduced to 2 and 9%, respectively, within the
first 9 months, and to 8 and 4%, respectively, over the
Fig. 9 Graph showing the average change in quadriceps cross- entire observation period (24 months) (Fig. 10). Patellar
sectional area and in cartilage thickness during 7 weeks of
cartilage deformation was 9% 4 weeks after immobiliza-
partial weight bearing of the knee (sole contact) in a group of
20 volunteers following a fracture of the ankle joint. tion (the first time point at which the participant was
able to perform deep knee bends) and was lower at later
time points (1–6% at 6–18 months). These findings
or decrease in cartilage volume or thickness was indicate that the stiffness of the patellar cartilage may
observed in the contra-lateral limb that was subject to be reduced after immobilization, probably as a conse-
increased loading during the 7-week period. These quence of biochemical alterations of the cartilage.
data indicate that cartilage undergoes some process of
atrophy in the absence of mechanical stimulation. The
Increased loading conditions
findings may have important implications for the clini-
cal management of the postoperative period in bone In a cross-sectional study of 92 children (age 9–18 years),
and joint surgery, and also for long-term space travel in Jones et al. (2000) reported a significant association
the context of the international space station or a jour- between cartilage volume and self-reported level of
ney to Mars. These observations in particular raise the exercise in children. The authors observed that physical
question as to what extent morphological changes
(cartilage thinning) during reduced weight-bearing
conditions are reversible.
In immature beagle dogs, Kiviranta et al. (1994)
reported that after 11 weeks of immobilization and
15 weeks of remobilization, the GAG content was fully
restored in most joint compartments, but not in the
peripheral regions of the femoral condyles. They also
found an incomplete restoration of femoral cartilage
thickness after remobilization and reasoned that there
was an inability of previously unloaded cartilage to with-
stand physiological loads during the remobilization
process (Kiviranta et al. 1994). The same group reported
a decrease in indentation stiffness after 11 weeks of Fig. 10 Graph showing the side differences of quadriceps
immobilization, which was not fully restored during a cross-sectional area (CSA) and mean patellar cartilage
thickness (in percentage left vs. right) during a 24-month
50-week remobilization period (Haapala et al. 1999). The
remobilization period in one subject, after 6 weeks of
authors claimed that extended immobilization of a joint immobilization of the left limb, with no weight bearing and
may cause long-lasting biochemical and biomechanical restriction of knee movement from 0° to 30° of flexion.
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
506 The effects of exercise on human articular cartilage, F. Eckstein et al.
activity was a significant explanatory factor for cartilage exercising twice per week and (3) elite runners. The
volume at all sites in the knee (r2 = 7–14%, P < 0.05) index was found to be significantly higher in individuals
and that the most consistent association was with who exercised regularly, and still higher in the elite
vigorous activity in the 2 weeks prior to imaging. In a runners. The authors concluded that human knee
longitudinal study of 74 children of the same cohort cartilage may adapt to exercise by increasing the GAG
(observation period 1.3 –1.9 years) the authors (Jones content, but that a higher proportion of extracellular
et al. 2003) found an association of average intensity of body water (a larger distribution volume for the contrast
sport (again evaluated by responses to a questionnaire). agent applied) may also to some extent explain the
Subjects above the median were found to gain approx- higher dGEMRIC index values in elite runners. Recently,
imately twice as much cartilage as those below the the same group (Roos & Dahlberg, 2005) reported that
median at tibial (but not patellar) cartilage. From these the dGEMRIC index increased over 4 months in 30
studies, the authors concluded that cartilage develop- subjects (who had undergone partial medial meniscectomy
ment is amenable to modification. Note, however, that 3–5 years previously) during a supervised, three-times
analysis of cartilage volume does not permit one to weekly exercise protocol. There also was a relatively
separate the effect on cartilage development (thick- high correlation (r = 0.74) between change in T1 (Gd)
ness) and bone growth (epiphyseal joint surface area). and the self-reported change in physical activity level,
When investigating mature adults, however, Eckstein over the 4-month period. These results indicate that
et al. (2002a) found no difference in cartilage thickness compositional adaptation (increase in GAG content) of
in triathletes, who had been training for at least 10 h cartilage may occur over relatively short time intervals
per week over the last 3 years and had also been physi- in response to exercise and mechanical loading.
cally active throughout childhood and adolescence in Gratzke et al. (2002) compared knee cartilage
comparison with individuals who had never been physi- morphology in 14 elite athletes (seven weightlifters
cally active (< 1 h sport per week throughout life), had and seven bobsleigh sprinters) with 14 men who had
no job that involved physical activity, and had a normal never performed strength training (for a more detailed
body mass index (Eckstein et al. 2002a). The latter find- description of the participants see above). All athletes
ings suggest that the relatively great variability in had been actively training throughout adolescence, well
cartilage thickness observed between subjects is not before reaching skeletal maturity. The weightlifters
readily explained by variability in mechanical loading his- displayed 26% higher (P < 0.01) extensor forces, as
tory (Carter et al. 1991). Interestingly, however, triath- measured with a Cybex dynamometer, and 30% higher
letes displayed somewhat larger knee joint surface (P < 0.001) extensor MCSAs than the non-athletic
areas (+9%, P < 0.01 in men; +7%, P = 0.08 in women). volunteers. The same applied to the bobsleigh sprinters
These observations indicate that the biological mecha- (+ 43%/+23%, P < 0.001, respectively). The cartilage
nism to reduce high stress at the articular surface may thickness, articular joint surface area and chondro-
be by an increase in the area of the load-bearing osseous interface area were not significantly greater in
surface rather than an increase in cartilage thickness the group of athletes compared with the group of non-
(Eckstein et al. 2002a). A potential reason for this is that athletic volunteers, except for the cartilage thickness of
beyond a certain thickness the nutritive situation of the patella. This was 14% greater (P < 0.01) in the weight-
the cartilage becomes critical, and/or that the stress lifters and 17% greater (P < 0.01) in the sprinters.
distribution (load partitioning) within the cartilage Nevertheless, there was still a wide overlap in patellar
becomes unfavourable with thicker cartilage. With cartilage thickness values between the athletes and
thicker cartilage, there is more space for the interstitial non-athletic participants. The findings of this (and
fluid to escape laterally from the site of contact and previously cited) studies indicate that differences in
hydrostatic pressurization is reduced. With larger con- mechanical environment may not readily explain
tact areas, by contrast, the force is distributed onto a the relatively large variability of cartilage morphology
wider area, keeping the stress at the joint surface within observed between human subjects, despite enormous
reasonable limits, and the mechanism of hydrostatic interindividual differences in mechanical loading
pressurization of the interstitial fluid is enhanced. history throughout the relevant developmental period
Tiderius et al. (2003) compared the dGEMRIC index in (adolescence) in which endochondral ossification is
(1) non-exercising individuals, (2) individuals physically completed and cartilage form is determined. These
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
The effects of exercise on human articular cartilage, F. Eckstein et al. 507
findings, however, refer to the average cartilage separate entities. They observed a remarkable similarity
thickness throughout joint surfaces, and adaptation at in cartilage morphology between twins (coefficient
a regional level cannot be discounted. Why there was of variation 3.2% for cartilage thickness and 2.2% for
a trend towards increased patellar cartilage thickness joint surface area), in comparison with the substantially
in athletes with high muscle strength, and a trend larger variability between subjects for a young reference
towards larger joint surface areas in athletes with high population of 117 subjects (CV 12 and 11% for cartilage
endurance is currently unclear, but these findings will thickness in women and men, respectively, and 10 and
have to be confirmed in larger samples and in athletes 9% for joint surface areas). These findings suggest that
with different types of specializations. Future studies not only bone size (or joint surface areas), but also
should also include regional analyses of cartilage thick- cartilage thickness appears to be strongly determined
ness, which have so far not been presented in the con- by genetics. The lack of correlation in cartilage thick-
text of the response of cartilage to exercise. ness between the knee and ankle (Eckstein et al. 2004),
however, indicates that different genes may be respon-
sible for cartilage thickness in different joints of the
Genetic influence
human body.
In the interpretation of the cumulative data reviewed
in this article, environmental (mechanical) factors appear
Conclusion
to play only a small (if any) role in determining cartilage
morphology in adults, although a wide variability of Taken together, these findings indicate that differences
cartilage thickness is observed in the population, in cartilage form between individuals cannot be readily
even in the absence of arthritic changes (Eckstein et al. explained by functional adaptation to mechanics, and
2001a; Burgkart et al. 2003; Hudelmaier et al. 2003). that the emergence and maintenance of cartilage form
One potential explanation for the intersubject differ- appears to depend on information from the genome.
ences observed in cartilage morphology is genetic dif- Although hyaline articular cartilage appears to display
ferences between individuals. atrophic changes (thinning) during unloading and may
Antoniades et al. (2001) examined the minimal joint exhibit compositional changes (increase in GAG) after
space width of hip radiographs of 222 monozygotic (MZ) exercise, it seems to differ from other musculoskeletal
and 240 dizygotic (DZ) twins. They found that genetic tissues with load-bearing function as it cannot increase
factors accounted for most of the variation in joint space tissue mass postnatally as a result of mechanical stimu-
width, but were not able to make direct measurements lation (Lamarck, 1809; Darwin, 1872; Roux, 1881; Wolff,
of cartilage thickness. Hunter et al. (2003) examined 31 1892; Pauwels, 1980; Carter et al. 1991; Huiskes et al.
MZ and 37 DZ twin pairs to assess the relative contribu- 2000). The specific signals that stop the ossification
tion of genetic and environmental factors to knee cartilage front from progressing to the joint surface (and that
volume. The heritability was estimated to range from preserve a cartilage layer of given thickness) remain
61 to 76% for different compartments of the knee. How- enigmatic. However, our results clearly suggest that,
ever, the authors used an MR sequence (T2-weighted, contrary to general expectation, mechanical feedback
fat-saturated sagittal gradient echo) that has not been does not play a relevant role in this process and, in con-
validated for the purpose of cartilage volume measure- trast to bone, does not serve to regulate the complex
ments, and cartilage volume is strongly dependent on biochemical metabolic machinery towards lasting
bone size, so that the genetic contribution to cartilage optimality of cartilage form (Huiskes et al. 2000). In
(thickness) formation is difficult to estimate. attempting to address the question of why (in contrast
Zhai et al. (2004) investigated the heritability of cartilage to muscle and bone) cartilage does not appear to
volume and bone size by examining sibling pairs. They adapt its mass to mechanical stimulation, the following
estimated the heritability of cartilage volume to be aspects need to be considered. (1) Loss of cartilage and
65 – 84% for various knee compartments, and that of joint function is a problem generally encountered by
bone size to be 57–85%. Again, however, cartilage individuals after their reproductive period and – in con-
thickness was not determined directly. trast to bone fracture and muscle weakness – this may
Siedek et al. (2002) examined 12 MZ twin pairs to deter- have not created evolutionary pressures for the tissue
mine knee cartilage thickness and joint surface areas as to be able to adapt to mechanical usage. (2) Whereas
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
508 The effects of exercise on human articular cartilage, F. Eckstein et al.
too much bone or too much muscle are metabolically Huskes R), pp. 447– 494. Philadelphia: Lippincott, Williams &
expensive and provide a clear disadvantage for fast Wilkins.
Bashir A, Gray ML, Boutin RD, Burstein D (1997) Glyco-
locomotion, a slight increase in cartilage thickness has
saminoglycan in articular cartilage: in vivo assessment with
no known negative consequences on metabolism and delayed Gd (DTPA) (2-)-enhanced MR imaging. Radiology
speed of locomotion. Therefore, there may have been 205, 551–558.
less of an evolutionary pressure to adapt cartilage Bashir A, Gray ML, Hartke J, Burstein D (1999) Nondestructive
imaging of human cartilage glycosaminoglycan concentra-
morphology to the immediate mechanical demands
tion by MRI. Magn Reson Med 41, 857– 865.
encountered by the individual. (3) Lastly, whereas ‘more’ Bergmann G, Graichen F, Rohlmann A (1993) Hip joint loading
muscle provides more tensile strength, and ‘more’ bone during walking and running, measured in two patients. J
provides higher structural compressive and bending Biomech 26, 969 – 990.
strength and hence better protection against fractures, Booth FW (1994) Terrestrial applications of bone and muscle
research in microgravity. Adv Space Res 14, 373 –376.
‘more’ cartilage is not known to be associated with
Brama PA, Tekoppele JM, Bank RA, Van Weeren PR, Barneveld A
improved mechanical competence of joints. There may (1999) Influence of site and age on biochemical characteristics
thus exist a decoupling between functional competence of the collagen network of equine articular cartilage. Am J
and tissue mass. Hydrostatic pressurization provides a Vet Res 60, 341–345.
Buckwalter JA, Mankin HJ (1998a) Articular cartilage: degen-
mechanism by which cartilage is able to distribute joint
eration and osteoarthritis, repair, regeneration, and trans-
forces evenly onto the subchondral bone (Ateshian et al. plantation. Instr Course Lect 47, 487–504.
1994; Mow et al. 2003), protect itself from mechanical Buckwalter JA, Mankin HJ (1998b) Articular cartilage: tissue
damage, and probably also provides almost frictionless design and chondrocyte–matrix interactions. Instr Course
Lect 47, 477–486.
surfaces during dynamic motion (Krishnan et al. 2003).
Burgkart R, Glaser C, Hyhlik-Durr A, et al. (2001) Magnetic
This mechanism is probably more difficult to accom- resonance imaging-based assessment of cartilage loss in severe
plish in a thick cartilage layer, in which the interstitial osteoarthritis: accuracy, precision, and diagnostic value.
fluid can escape laterally from the site of contact. These Arthritis Rheum 44, 2072–2077.
aspects may provide some explanation as to why carti- Burgkart R, Glaser C, Hinterwimmer S, et al. (2003) Feasibility
of T and Z scores from magnetic resonance imaging data for
lage is less (if at all) responsive to increased mechanical
quantification of cartilage loss in osteoarthritis. Arthritis
loading. However, the inability of cartilage to adapt to Rheum 48, 2829 –2835.
its mechanical environment may be coupled with its Burstein D, Bashir A, Gray ML (2000) MRI techniques in early
inability to repair following mechanical and other insults stages of cartilage disease. Invest Radiol 35, 622– 638.
Burstein D, Gray M (2003) New MRI techniques for imag-
(Hunziker et al. 2002). This inability may be essential
ing cartilage. J Bone Joint Surg Am 85, Supplement 2, 70–
in understanding the deleterious consequences of 77.
cartilage loss in degenerative joint disease and the Carter DR, Wong M (1988a) Mechanical stresses and endo-
large burden of osteoarthritis on the aging population chondral ossification in the chondroepiphysis. J Orthop Res
(Yelin & Callahan, 1995). 6, 148 –154.
Carter DR, Wong M (1988b) The role of mechanical loading
histories in the development of diarthrodial joints. J Orthop
Res 6, 804 – 816.
References
Carter DR, Wong M, Orr TE (1991) Musculoskeletal ontogeny,
Al Ali D, Graichen H, Faber S, et al. (2002) Quantitative carti- phylogeny, and functional adaptation. J Biomech 24 (Suppl. 1),
lage imaging of the human hind foot: precision and inter- 3 –16.
subject variability. J Orthop Res 20, 249 –256. Carter DR, Wong M (2003) Modelling cartilage mechanobiology.
Antoniades L, Spector TD, MacGregor AJ (2001) The genetic Philos Trans R Soc Lond B Biol Sci 358, 1461–1471.
contribution to hip joint morphometry and relationship to Chen AC, Temple MM, Ng DM, et al. (2002) Induction of
hip cartilage thickness. Osteoarthritis Cartilage 9, 593–595. advanced glycation end products and alterations of the
Ateshian GA, Soslowsky LJ, Mow VC (1991) Quantitation of tensile properties of articular cartilage. Arthritis Rheum 46,
articular surface topography and cartilage thickness in 3212–3217.
knee joints using stereophotogrammetry. J Biomech 24, Cicuttini F, Forbes A, Morris K, et al. (1999) Gender differences
761–776. in knee cartilage volume as measured by magnetic resonance
Ateshian GA, Lai WM, Zhu WB, Mow VC (1994) An asymptotic imaging. Osteoarthritis Cartilage 7, 265 –271.
solution for the contact of two biphasic cartilage layers. J Cicuttini F, Forbes A, Asbeutah A, Morris K, Stuckey S (2000)
Biomech 27, 1347–1360. Comparison and reproducibility of fast and conventional
Ateshian G, Mow VC (2005) Friction, lubrication, and wear of spoiled gradient-echo magnetic resonance sequences in the
articular cartilage and diathrodial joints. In Basic Orthopaedic determination of knee cartilage volume. J Orthop Res 18,
Biomechanics and Mechanobiology, 3rd edn (eds Mow VC, 580 –584.
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
The effects of exercise on human articular cartilage, F. Eckstein et al. 509
Cicuttini FM, Wluka AE, Wang Y, et al. (2002) Compartment Eckstein F, Heudorfer L, Faber SC, et al. (2002b) Long-term and
differences in knee cartilage volume in healthy adults. J resegmentation precision of quantitative cartilage MR
Rheumatol 29, 554–556. imaging (qMRI). Osteoarthritis Cartilage 10, 922–928.
Cicuttini FM, Wluka AE, Forbes A, Wolfe R (2003) Comparison Eckstein F, Muller S, Faber SC, et al. (2002c) Side differences of
of tibial cartilage volume and radiologic grade of the tibio- knee joint cartilage volume, thickness, and surface area,
femoral joint. Arthritis Rheum 48, 682– 688. and correlation with lower limb dominance – an MRI-based
Cohen ZA, McCarthy DM, Kwak SD, et al. (1999) Knee cartilage study. Osteoarthritis Cartilage 10, 914 –921.
topography, thickness, and contact areas from MRI: in-vitro Eckstein F, Siedek V, Glaser C, et al. (2004) Correlation and sex
calibration and in-vivo measurements. Osteoarthritis Cartilage differences between ankle and knee cartilage morphology
7, 95–109. determined by quantitative magnetic resonance imaging.
Cohen ZA, Roglic H, Grelsamer RP, et al. (2001) Patellofemoral Ann Rheum Dis 63, 1490 –1495.
stresses during open and closed kinetic chain exercises. An Eckstein F, Charles HC, Buck RJ, et al. (2005a) Accuracy and
analysis using computer simulation. Am J Sports Med 29, precision of quantitative assessment of cartilage morpho-
480–487. logy by magnetic resonance imaging at 3.0T. Arthritis Rheum
Cohen ZA, Mow VC, Henry JH, Levine WN, Ateshian GA (2003) 52, 3132–3136.
Templates of the cartilage layers of the patellofemoral joint Eckstein F, Hudelmaier M, Wirth W, et al. (2005b) Double echo
and their use in the assessment of osteoarthritic cartilage steady state (DESS) Magnetic resonance imaging of knee
damage. Osteoarthritis Cartilage 11, 569 –579. articular cartilage at 3 Tesla – a pilot study for the osteoarthritis
Darwin C (1872) The Origin of Species, 6th edn. New York: initiative. Ann Rheum Dis, doi: 10.113b/ard.2005.039370.
New America Library. Eckstein F, Lemberger B, Gratzke C, et al. (2005c) In vivo cartilage
Eckstein F, Sittek H, Milz S, et al. (1995) The potential of deformation after different types of activity and its dependence
magnetic resonance imaging (MRI) for quantifying articular on physical training status. Ann Rheum Dis 64, 291–295.
cartilage thickness – a methodological study. Clin Biomech Faber SC, Eckstein F, Lukasz S, et al. (2001) Gender differences
(Bristol, Avon) 10, 434 – 440. in knee joint cartilage thickness, volume and articular sur-
Eckstein F, Gavazzeni A, Sittek H, et al. (1996a) Determination face areas: assessment with quantitative three-dimensional
of knee joint cartilage thickness using three-dimensional MR imaging. Skeletal Radiol 30, 144–150.
magnetic resonance chondro-crassometry (3D MR-CCM). Frahm J, Haase A, Matthaei D (1986) Rapid three-dimensional
Magn Reson Med 36, 256 –265. MR imaging using the FLASH technique. J Comput Assist
Eckstein F, Sittek H, Gavazzeni A, et al. (1996b) Magnetic Tomogr 10, 363 –368.
resonance chondro-crassometry (MR CCM): a method for Froimson MI, Ratcliffe A, Gardner TR, Mow VC (1997) Differ-
accurate determination of articular cartilage thickness? Magn ences in patellofemoral joint cartilage material properties
Reson Med 35, 89 –96. and their significance to the etiology of cartilage surface
Eckstein F, Schnier M, Haubner M, et al. (1998a) Accuracy of fibrillation. Osteoarthritis Cartilage 5, 377–386.
cartilage volume and thickness measurements with mag- Glaser C, Faber S, Eckstein F, et al. (2001) Optimization and
netic resonance imaging. Clin Orthop 352, 137–148. validation of a rapid high-resolution T1-w 3D FLASH water
Eckstein F, Tieschky M, Faber SC, et al. (1998b) Effect of phys- excitation MRI sequence for the quantitative assessment
ical exercise on cartilage volume and thickness in vivo: MR of articular cartilage volume and thickness. Magn Reson
imaging study. Radiology 207, 243 –248. Imaging 19, 177–185.
Eckstein F, Tieschky M, Faber S, Englmeier KH, Reiser M (1999) Gold GE, Han E, Stainsby J, et al. (2004a) Musculoskeletal MRI
Functional analysis of articular cartilage deformation, at 3.0 T: relaxation times and image contrast. AJR Am J
recovery, and fluid flow following dynamic exercise in vivo. Roentgenol 183, 343 –351.
Anat Embryol (Berl) 200, 419 – 424. Gold GE, Suh B, Sawyer-Glover A, Beaulieu C (2004b) Muscu-
Eckstein F, Lemberger B, Stammberger T, Englmeier KH, loskeletal MRI at 3.0 T: initial clinical experience. AJR Am J
Reiser M (2000a) Patellar cartilage deformation in vivo after Roentgenol 183, 1479 –1486.
static versus dynamic loading. J Biomech 33, 819 – 825. Graichen H, Eisenhart-Rothe R, Vogl T, Englmeier KH, Eckstein F
Eckstein F, Lemberger B, Stammberger T, Englmeier KH, (2004) Quantitative assessment of cartilage status in osteo-
Reiser M (2000b) Patellar cartilage deformation in vivo after arthritis by quantitative magnetic resonance imaging:
static versus dynamic loading. J Biomech 33, 819 – 825. technical validation for use in analysis of cartilage volume
Eckstein F, Reiser M, Englmeier KH, Putz R (2001a) In vivo mor- and further morphologic parameters. Arthritis Rheum 50,
phometry and functional analysis of human articular cartilage 811– 816.
with quantitative magnetic resonance imaging – from image Graichen H, Jakob J, Eisenhart-Rothe R, et al. (2003) Validation
to data, from data to theory. Anat Embryol (Berl) 203, 147–173. of cartilage volume and thickness measurements in the human
Eckstein F, Winzheimer M, Hohe J, Englmeier KH, Reiser M shoulder with quantitative magnetic resonance imaging.
(2001b) Interindividual variability and correlation among Osteoarthritis Cartilage 11, 475– 482.
morphological parameters of knee joint cartilage plates: Graichen H, Springer V, Flaman T, et al. (2000) Validation
analysis with three-dimensional MR imaging. Osteoarthritis of high-resolution water-excitation magnetic resonance
Cartilage 9, 101–111. imaging for quantitative assessment of thin cartilage layers.
Eckstein F, Faber S, Muhlbauer R, et al. (2002a) Functional Osteoarthritis Cartilage 8, 106 –114.
adaptation of human joints to mechanical stimuli. Osteoar- Gratzke C, Glaser C, Englmeier KH, Reiser M, Eckstein F (2002)
thritis Cartilage 10, 44 – 50. Comparison of cartilage morphology in professional weight-
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
510 The effects of exercise on human articular cartilage, F. Eckstein et al.
lifters and sprinters with normal volunteers suggests that human effect of sex, growth, body composition, and physical activ-
articular cartilage cannot adapt to functional stimulation. ity. Pediatr Res 54, 230–236.
Osteoarthritis Cartilage 10 [(Suppl. A)], S11 [abstract]. Karvonen RL, Negendank WG, Teitge RA, et al. (1994) Factors
Gray ML, Eckstein F, Peterfy C, et al. (2004) Toward imaging affecting articular cartilage thickness in osteoarthritis and
biomarkers for osteoarthritis. Clin Orthop 427, S175–S181. aging. J Rheumatol 21, 1310 –1318.
Haapala J, Arokoski JP, Hyttinen MM, et al. (1999) Remobili- Keller TS, Strauss AM, Szpalski M (1992) Prevention of bone
zation does not fully restore immobilization induced articu- loss and muscle atrophy during manned space flight. Micro-
lar cartilage atrophy. Clin Orthop 00, 218–229. gravity Q 2, 89 –102.
Hardy PA, Recht MP, Piraino DW (1998) Fat suppressed MRI of Kim YJ, Bonassar LJ, Grodzinsky AJ (1995) The role of cartilage
articular cartilage with a spatial-spectral excitation pulse. J streaming potential, fluid flow and pressure in the stimula-
Magn Reson Imaging 8, 1279–1287. tion of chondrocyte biosynthesis during dynamic compres-
Hehne HJ (1990) Biomechanics of the patellofemoral joint and sion. J Biomech 28, 1055 –1066.
its clinical relevance. Clin Orthop 00, 73–85. Kiviranta I, Tammi M, Jurvelin J, et al. (1994) Articular carti-
Helminen HJ, Kiviranta I, Saamanen AM, et al. (1992) Effect of lage thickness and glycosaminoglycan distribution in the
motion and load on articular cartilage in animal models. In young canine knee joint after remobilization of the immo-
Articular Cartilage and Osteoarthritis (eds Kuettner KE, bilized limb. J Orthop Res 12, 161–167.
Roth A), pp. 501–510. New York: Raven. Kornaat PR, Reeder SB, Koo S, et al. (2005) MR imaging of
Herberhold C, Stammberger T, Faber S, et al. (1998) An MR- articular cartilage at 1.5T and 3.0T: comparison of SPGR and
based technique for quantifying the deformation of articu- SSFP sequences. Osteoarthritis Cartilage 13, 338–344.
lar cartilage during mechanical loading in an intact cadaver Krishnan R, Park S, Eckstein F, Ateshian GA (2003) Inhomoge-
joint. Magn Reson Med 39, 843–850. neous cartilage properties enhance superficial interstitial
Herberhold C, Faber S, Stammberger T, et al. (1999) In situ fluid support and frictional properties, but do not provide a
measurement of articular cartilage deformation in intact homogeneous state of stress. J Biomech Eng 125, 569–577.
femoropatellar joints under static loading. J Biomech 32, Kshirsagar AA, Watson PJ, Tyler JA, Hall LD (1998) Measure-
1287–1295. ment of localized cartilage volume and thickness of human
Hinterwimmer S, Krammer M, Krotz M, et al. (2004) Cartilage knee joints by computer analysis of three-dimensional
atrophy in the knees of patients after seven weeks of partial magnetic resonance images. Invest Radiol 33, 289 –299.
load bearing. Arthritis Rheum 50, 2516–2520. Kunz M, Williams A, McKenzie C, Burstein D, Eckstein F (2005)
Hohe J, Ateshian G, Reiser M, Englmeier KH, Eckstein F (2002) No prolonged deformation of knee joint cartilage after the
Surface size, curvature analysis, and assessment of knee Boston marathon. Osteoarthritis Cart 13 (Suppl. A), 124
joint incongruity with MRI in vivo. Magn Reson Med 47, [abstract].
554–561. Lamarck JB (1809) Philosophie Zoologique. Paris: Bailleres.
Hudelmaier M, Glaser C, Hohe J, et al. (2001) Age-related Liess C, Lüsse S, Karger N, Heller M, Glüer CC (2002) Detection
changes in the morphology and deformational behavior of of changes in cartilage water content using MRI T2-mapping
knee joint cartilage. Arthritis Rheum 44, 2556–2561. in vivo. Osteoarthritis Cartilage 10, 907–913.
Hudelmaier M, Glaser C, Englmeier KH, et al. (2003) Correla- Lusse S, Claassen H, Gehrke T, et al. (2000) Evaluation of water
tion of knee-joint cartilage morphology with muscle cross- content by spatially resolved transverse relaxation times of
sectional areas vs. anthropometric variables. Anat Rec 270A, human articular cartilage. Magn Reson Imaging 18, 423 –430.
175–184. Lynch JA, Zaim S, Zhao J, Peterfy CG, Genant HK (2001) Auto-
Huiskes R, Ruimerman R, Van Lenthe GH, Janssen JD (2000) matic measurement of subtle changes in articular cartilage
Effects of mechanical forces on maintenance and adapta- from MRI of teh knee by combining 3D image registration
tion of form in trabecular bone. Nature 405, 704–706. and segmentation. Proc SPIE (Int Soc for Opt Engineering)
Hunter DJ, Snieder H, March L, Sambrook PN (2003) Genetic 4322, 431– 439.
contribution to cartilage volume in women: a classical twin McGibbon CA, Dupuy DE, Palmer WE, Krebs DE (1998) Carti-
study. Rheumatology (Oxford) 42, 1495–1500. lage and subchondral bone thickness distribution with MR
Hunziker EB (2002) Articular cartilage repair: basic science and imaging. Acad Radiol 5, 20 –25.
clinical progress. A review of the current status and pros- McGibbon CA, Trahan CA (2003) Measurement accuracy of
pects. Osteoarthritis Cartilage 10, 432–463. focal cartilage defects from MRI and correlation of MRI
Hunziker EB, Quinn TM, Hauselmann HJ (2002) Quantitative graded lesions with histology: a preliminary study. Osteo-
structural organization of normal adult human articular car- arthritis Cartilage 11, 483– 493.
tilage. Osteoarthritis Cartilage 10, 564–572. Meachim G (1971) Effect of age on the thickness of adult articular
Hyhlik-Dürr A, Faber S, Burgkart R, et al. (2000) Precision of cartilage at he shoulder joint. Ann Rheum Dis 30, 43 –46.
tibial cartilage morphometry with a coronal water-excitation Meachim G, Bentley G, Baker R (1977) Effect of age on thickness
MR sequence. Eur Radiol 10, 297–303. of adult patellar articular cartilage. Ann Rheum Dis 36, 563–568.
Jones G, Glisson M, Hynes K, Cicuttini F (2000) Sex and site dif- Mosher TJ, Dardzinski BJ (2004) Cartilage MRI T2 relaxation
ferences in cartilage development: a possible explanation time mapping: overview and applications. Semin Muscu-
for variations in knee osteoarthritis in later life. Arthritis loskelet Radiol 8, 355–368.
Rheum 43, 2543–2549. Mosher TJ, Liu Y, Yang QX, et al. (2004) Age dependency of
Jones G, Ding C, Glisson M, et al. (2003) Knee articular carti- cartilage magnetic resonance imaging T2 relaxation times
lage development in children: a longitudinal study of the in asymptomatic women. Arthritis Rheum 50, 2820 –2828.
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
The effects of exercise on human articular cartilage, F. Eckstein et al. 511
Mosher TJ, Smith HE, Collins C, et al. (2005) Change in knee Sittek H, Eckstein F, Gavazzeni A, et al. (1996) Assessment of
cartilage T2 at MR imaging after running: a feasibility study. normal patellar cartilage volume and thickness using MRI:
Radiology 234, 245–249. an analysis of currently available pulse sequences. Skeletal
Mow VC, Holmes MH, Lai WM (1984) Fluid transport and Radiol 25, 55–62.
mechanical properties of articular cartilage: a review. J Bio- Springer V, Graichen H, Stammberger T, et al. (1998) [Non-
mech 17, 377–394. invasive analysis of cartilage volume and cartilage thickness
Mow VC, Ateshian GA, Spilker RL (1993) Biomechanics of in the human elbow joint using MRI]. Anat Anz 180, 331–
diarthrodial joints: a review of twenty years of progress. 338.
J Biomech Eng 115, 460 – 467. Stammberger T, Eckstein F, Englmeier KH, Reiser M (1999)
Mow VC, Gu WY, Chen FH (2003) Structure and function of Determination of 3D cartilage thickness data from MR
articular cartilage and meniscus. In Basic Orthopaedic imaging: computational method and reproducibility in the
Biomechanics and Mechanobiology, 3rd edn (eds Mow VC, living. Magn Reson Med 41, 529 –536.
Huskes R), pp. 181–258. Philadelphia: Lippincott, Williams & Stammberger T, Hohe J, Englmeier KH, Reiser M, Eckstein F
Wilkins. (2000) Elastic registration of 3D cartilage surfaces from MR
Newton PM, Mow VC, Gardner TR, Buckwalter JA, Albright JP image data for detecting local changes in cartilage thick-
(1997) Winner of the 1996 Cabaud Award. The effect of life- ness. Magn Reson Med 44, 592– 601.
long exercise on canine articular cartilage. Am J Sports Med Takahashi M, Hoshino H, Kushida K, Inoue T (1995) Direct
25, 282–287. measurement of crosslinks, pyridinoline, deoxypyridinoline,
Papa E, Cappozzo A (2000) Sit-to-stand motor strategies inves- and pentosidine, in the hydrolysate of tissues using high-
tigated in able-bodied young and elderly subjects. J Bio- performance liquid chromatography. Anal Biochem 232,
mech 33, 1113–1122. 158–162.
Pauwels F (1980) Biomechanics of the Locomotion Apparatus. Tiderius CJ, Olsson LE, Leander P, Ekberg O, Dahlberg L (2003)
Berlin: Springer. Delayed gadolinium-enhanced MRI of cartilage (dGEMRIC)
Peterfy CG, Van Dijke CF, Janzen DL, et al. (1994) Quanti- in early knee osteoarthritis. Magn Reson Med 49, 488–
fication of articular cartilage in the knee with pulsed 492.
saturation transfer subtraction and fat-suppressed MR Tieschky M, Faber S, Haubner M, et al. (1997) Repeatability of
imaging: optimization and validation. Radiology 192, 485 – patellar cartilage thickness patterns in the living, using a
491. fat-suppressed magnetic resonance imaging sequence with
Peterfy CG, Van Dijke CF, LUY, et al. (1995) Quantification short acquisition time and three-dimensional data process-
of the volume of articular cartilage in the metacarpopha- ing. J Orthop Res 15, 808– 813.
langeal joints of the hand: accuracy and precision of Urban JP (1994) The chondrocyte: a cell under pressure. Br J
three-dimensional MR imaging. AJR Am J Roentgenol 165, Rheumatol 33, 901–908.
371–375. Vanwanseele B, Eckstein F, Knecht H, Stussi E, Spaepen A
Raynauld JP, Kauffmann C, Beaudoin G, et al. (2003) Reliabil- (2002a) Knee cartilage of spinal cord-injured patients dis-
ity of a quantification imaging system using magnetic reso- plays progressive thinning in the absence of normal joint
nance images to measure cartilage thickness and volume in loading and movement. Arthritis Rheum 46, 2073–2078.
human normal and osteoarthritic knees. Osteoarthritis Car- Vanwanseele B, Lucchinietti E, Stussi E (2002b) The effects of
tilage 11, 351–360. immobilization on the characteristics of articular cartilage:
Recht MP, Kramer J, Marcelis S, et al. (1993) Abnormalities of current concepts and future directions. Osteoarthritis Carti-
articular cartilage in the knee: analysis of available MR tech- lage 10, 408 – 419.
niques. Radiology 187, 473– 478. Vanwanseele B, Eckstein F, Knecht H, Spaepen A, Stussi E
Roos EM, Dahlberg L (2005) Positive effects of moderate exer- (2003) Longitudinal analysis of cartilage atrophy in the
cise on glycosaminoglycan content in knee cartilage: a four- knees of patients with spinal cord injury. Arthritis Rheum
month, randomized, controlled trial in patients at risk of 48, 3377–3381.
osteoarthritis. Arthritis Rheum 52, 3507–3514. Vanwanseele B, Eckstein F, Hadwighorst H, et al. (2004) In
Roux W (1881) Der Kampf der Teile Im Organismus. Leipzig: vivo precision of quantitative shoulder cartilage measure-
Engelmann. ments, and changes after spinal cord injury. Magn Reson
Sah RL, Kim YJ, Doong JY, et al. (1989) Biosynthetic response Med 51, 1026–1030.
of cartilage explants to dynamic compression. J Orthop Res Verzijl N, Degroot J, Ben ZC, et al. (2002) Crosslinking by
7, 619–636. advanced glycation end products increases the stiffness
Saudek DM, Kay J (2003) Advanced glycation endproducts and of the collagen network in human articular cartilage: a pos-
osteoarthritis. Curr Rheumatol Rep 5, 33 – 40. sible mechanism through which age is a risk factor for osteo-
Siedek V, Glaser C, Englmeier KH, Reiser M, Eckstein F (2002) arthritis. Arthritis Rheum 46, 114–123.
MRI-based analysis of knee and ankle cartilage in mono- Waldman SD, Spiteri CG, Grynpas MD, Pilliar RM, Kandel RA
cygotic twins suggests that its morphology is strongly deter- (2003) Long-term intermittent shear deformation improves
mined by genetics. Osteoarthritis Cartilage 10 (Suppl. A), the quality of cartilaginous tissue formed in vitro. J Orthop
S56 (PS 110) [abstract]. Res 21, 590 –596.
Sitoci KH, Hudelmaier M, Glaser C, et al. (2003) Nocturnal Waterton JC, Solloway S, Foster JE, et al. (2000) Diurnal vari-
changes of cartilage morphology in healthy subjects. Osteo- ation in the femoral articular cartilage of the knee in young
arthritis Cartilage 11 (Suppl. A), S95 [abstract]. adult humans. Magn Reson Med 43, 126 –132.
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
512 The effects of exercise on human articular cartilage, F. Eckstein et al.
Williams A, Gillis A, McKenzie C, et al. (2004) Glycosamino- Wong M, Carter DR (2003) Articular cartilage functional histo-
glycan distribution in cartilage as determined by delayed morphology and mechanobiology: a research perspective.
gadolinium-enhanced MRI of cartilage (dGEMRIC): Bone 33, 1–13.
potential clinical applications. AJR Am J Roentgenol 182, Yelin E, Callahan LF (1995) The economic cost and social and
167–172. psychological impact of musculoskeletal conditions. National
Williams A, Krishnan N, McKenzie C, Burstein D (2005) Mole- Arthritis Data Work Groups. Arthritis Rheum 38, 1351–1362.
cular imaging of cartilage effects of running a marathon on Zhai G, Stankovich J, Ding C, et al. (2004) The genetic contri-
dGEMRIC of the knee. Osteoarthritis Cartilage in press. bution to muscle strength, knee pain, cartilage volume,
Wolff J (1892) Das Gesetz der Transformation der Knochen. bone size, and radiographic osteoarthritis: a sibpair study.
Berlin: Hirschwald (reprinted Schattauer, Stuttgart 1991). Arthritis Rheum 50, 805 – 810.
© 2006 The Authors
Journal compilation © 2006 Anatomical Society of Great Britain and Ireland
You might also like
- Dynamics of The Human Masticatory SystemDocument12 pagesDynamics of The Human Masticatory SystemLinda Garcia PNo ratings yet
- Art:10 1007/s004290000154Document27 pagesArt:10 1007/s004290000154beacr22_22No ratings yet
- 810mecanobiologia en Suturas CranealesDocument9 pages810mecanobiologia en Suturas CranealesLalo MojicaNo ratings yet
- Tendon Tissue-Engineering ScaffoldsDocument21 pagesTendon Tissue-Engineering ScaffoldsVanessa GrüberNo ratings yet
- D H M S: Ynamics of The Uman Asticatory YstemDocument11 pagesD H M S: Ynamics of The Uman Asticatory YstemHugo A. Cárdenas IglesiasNo ratings yet
- Frog 2005Document11 pagesFrog 2005Alfi OktafaniNo ratings yet
- Bone Mechanical Properties in Healthy and Diseased StatesDocument31 pagesBone Mechanical Properties in Healthy and Diseased StatesThauane MaiaNo ratings yet
- 1 s2.0 S0021929012002801 MainDocument6 pages1 s2.0 S0021929012002801 MainCarlos De la cruzNo ratings yet
- Gardner A 2000Document11 pagesGardner A 2000Bastion ReinhartNo ratings yet
- Gardnera 2000Document11 pagesGardnera 2000Bastion ReinhartNo ratings yet
- Bone Remodelling: Scientific SectionDocument7 pagesBone Remodelling: Scientific SectionRohini TondaNo ratings yet
- Nihms 743965Document25 pagesNihms 743965registrepremsaNo ratings yet
- Temporomandibular: Dynamic Properties of The Joint DiscDocument5 pagesTemporomandibular: Dynamic Properties of The Joint DiscKevinNo ratings yet
- Mechanical Loads - Bone ResponseDocument19 pagesMechanical Loads - Bone ResponselllllAdelalllllNo ratings yet
- Hammer 2018Document14 pagesHammer 2018jklNo ratings yet
- ChaitowBook ExcerptDocument9 pagesChaitowBook ExcerptQuiroprácticaParaTodosNo ratings yet
- Craniofacial Biomechanics An Overview of Recent Multibody Modeling StudiesDocument10 pagesCraniofacial Biomechanics An Overview of Recent Multibody Modeling StudiesDenise MathreNo ratings yet
- The Human Meniscus: A Review of Anatomy, Function, Injury, and Advances in TreatmentDocument19 pagesThe Human Meniscus: A Review of Anatomy, Function, Injury, and Advances in TreatmentRazlivenaTintaNo ratings yet
- MB41Document6 pagesMB41GERARDO TORRES RUIZNo ratings yet
- Primary Role of Functional Matrices in Facial GrowthDocument12 pagesPrimary Role of Functional Matrices in Facial GrowthPranshu MathurNo ratings yet
- Load-Displacement Properties of The Human Triceps Surae Aponeurosis and Tendon in Runners and Non-RunnersDocument9 pagesLoad-Displacement Properties of The Human Triceps Surae Aponeurosis and Tendon in Runners and Non-RunnersbanditoszNo ratings yet
- 05 - Journal of Anatomy - 2013 - GerlingDocument11 pages05 - Journal of Anatomy - 2013 - Gerlingalan.consultoriafitnessNo ratings yet
- Tsubota 2009Document7 pagesTsubota 2009Catherine NocuaNo ratings yet
- 1 s2.0 S0021929023001525 MainDocument12 pages1 s2.0 S0021929023001525 MainJose PerezNo ratings yet
- Dynamics of The Human Masticatory System. ReviewDocument12 pagesDynamics of The Human Masticatory System. Reviewjrr158No ratings yet
- Multiscale Modeling of Bone Tissue MechanobiologyDocument12 pagesMultiscale Modeling of Bone Tissue MechanobiologyLina AvilaNo ratings yet
- Paper58 Mechanical Properties Hierarchical Structure Bone Med Eng Phys 20 (2) Rho Et Al 1998Document11 pagesPaper58 Mechanical Properties Hierarchical Structure Bone Med Eng Phys 20 (2) Rho Et Al 1998leksremeshNo ratings yet
- The Biomechanics of Stretching: Duane KnudsonDocument10 pagesThe Biomechanics of Stretching: Duane KnudsonAnuragNo ratings yet
- The Biomechanics of Stretching: Duane KnudsonDocument10 pagesThe Biomechanics of Stretching: Duane KnudsonSanjanaNo ratings yet
- (1987) Mecanostato de FrostDocument9 pages(1987) Mecanostato de FrostDaniel EchegarayNo ratings yet
- Nihms 796031Document21 pagesNihms 796031registrepremsaNo ratings yet
- Finite Element Investigation of The Loadin Grate Effect On The Spinal Load-Sharing Changes Under Impact ConditionsDocument11 pagesFinite Element Investigation of The Loadin Grate Effect On The Spinal Load-Sharing Changes Under Impact ConditionsNico FranckNo ratings yet
- Biomechanics of Craniofacial Sutures Orthopedic ImplicationsDocument8 pagesBiomechanics of Craniofacial Sutures Orthopedic ImplicationsMuhammad FahmyNo ratings yet
- Mechanical Loading of The Intervertebral Disc: From The Macroscopic To The Cellular LevelDocument12 pagesMechanical Loading of The Intervertebral Disc: From The Macroscopic To The Cellular LevelDaniel FreireNo ratings yet
- Journal of Biomechanics: Junyan Li, Todd D. Stewart, Zhongmin Jin, Ruth K. Wilcox, John FisherDocument7 pagesJournal of Biomechanics: Junyan Li, Todd D. Stewart, Zhongmin Jin, Ruth K. Wilcox, John FisherRenka BlodersNo ratings yet
- MRM 20104Document6 pagesMRM 20104GerardoNo ratings yet
- Claes 1999Document12 pagesClaes 1999Bastion ReinhartNo ratings yet
- Vera Garcia 2006 Effects of Different Levels of Torso Coactivation On Trunk Muscular and Kinematic Responses To PoDocument13 pagesVera Garcia 2006 Effects of Different Levels of Torso Coactivation On Trunk Muscular and Kinematic Responses To PoMichael JunNo ratings yet
- Eight Weeks of Proprioceptive Neuromuscular FaciliDocument9 pagesEight Weeks of Proprioceptive Neuromuscular FaciliMauricio MoncadaNo ratings yet
- Biomechanism of StretchingDocument11 pagesBiomechanism of Stretchingsara mohamedNo ratings yet
- The Differential Roles of Periosteal and Capsular Functional Matrices in Orofacial GrowthDocument6 pagesThe Differential Roles of Periosteal and Capsular Functional Matrices in Orofacial GrowthCony Del CidNo ratings yet
- Whalen 1988Document13 pagesWhalen 1988ManuelMartinezMartínezNo ratings yet
- Paper CartilagoDocument7 pagesPaper CartilagoJaviera ZúñigaNo ratings yet
- Stretch-Shortening Cycle: A Powerful Model To Study Normal and Fatigued MuscleDocument10 pagesStretch-Shortening Cycle: A Powerful Model To Study Normal and Fatigued MuscleNuta Marius AlexandruNo ratings yet
- Bone Remodeling Wolff's LawDocument4 pagesBone Remodeling Wolff's LawThe Penitent OneNo ratings yet
- NIH Public Access: The Effects of Ligamentous Injury in The Human Lower Cervical SpineDocument13 pagesNIH Public Access: The Effects of Ligamentous Injury in The Human Lower Cervical SpineIsrael BlancoNo ratings yet
- Alierta 2014Document11 pagesAlierta 2014Bastion ReinhartNo ratings yet
- 2011 A Review of The Anatomy of The Hip Abductor Muscles, GluteusDocument12 pages2011 A Review of The Anatomy of The Hip Abductor Muscles, Gluteusmari netaNo ratings yet
- Fibrous Systems As Potential Solutions For Tendon and Ligament Repair, Healing, and RegenerationDocument26 pagesFibrous Systems As Potential Solutions For Tendon and Ligament Repair, Healing, and RegenerationDamaris SoileNo ratings yet
- Elastic Properties of Woven Bone: Effect of Mineral Content and Collagen Fibrils OrientationDocument14 pagesElastic Properties of Woven Bone: Effect of Mineral Content and Collagen Fibrils OrientationAlvaraso MarmolNo ratings yet
- Biomedicines 10 00342 v2Document25 pagesBiomedicines 10 00342 v2Affan Nadeem QaziNo ratings yet
- The Differential Roles of Periosteal and Capsular Functional Matrices in Orofacial GrowthDocument6 pagesThe Differential Roles of Periosteal and Capsular Functional Matrices in Orofacial GrowthAaron Neal DmdNo ratings yet
- Biomechanics of The Menisci of The KneeDocument9 pagesBiomechanics of The Menisci of The KneePaulo Emílio Alves AlvesNo ratings yet
- Functional Matrix HypothesisDocument160 pagesFunctional Matrix HypothesisRicha AhlawatNo ratings yet
- Biophysical stimuli influence cell differentiation during tissue formationDocument10 pagesBiophysical stimuli influence cell differentiation during tissue formationBastion ReinhartNo ratings yet
- Chains, Trains and Contractile Fields: Matt Wallden, MSC Ost Med, Do, ND, Associate EditorDocument8 pagesChains, Trains and Contractile Fields: Matt Wallden, MSC Ost Med, Do, ND, Associate EditorMohamed ElMeligieNo ratings yet
- Isometric Contraction Reduce Plantar Flexor Moment PDFDocument12 pagesIsometric Contraction Reduce Plantar Flexor Moment PDFWilda NingsihNo ratings yet
- Journal Of: Architectural Properties of The First Dorsal Interosseous MuscleDocument7 pagesJournal Of: Architectural Properties of The First Dorsal Interosseous MuscleHeculesNo ratings yet
- SMR X Cadena PosteriorDocument11 pagesSMR X Cadena PosteriorAlvaro RodriguezNo ratings yet
- Bone Remodeling Process: Mechanics, Biology, and Numerical ModelingFrom EverandBone Remodeling Process: Mechanics, Biology, and Numerical ModelingNo ratings yet
- Shrek 2014 - Bone Loss Over One Year of Training and Competition in Female CyclistsDocument14 pagesShrek 2014 - Bone Loss Over One Year of Training and Competition in Female CyclistsStavros LitsosNo ratings yet
- Specker 2015 - Does Exercise Influence Pediatric Bone - A Systematic ReviewDocument15 pagesSpecker 2015 - Does Exercise Influence Pediatric Bone - A Systematic ReviewStavros LitsosNo ratings yet
- Pelland 2004 - Efficacy of Strength Exercises For OA - Part I - A Meta-AnalysisDocument32 pagesPelland 2004 - Efficacy of Strength Exercises For OA - Part I - A Meta-AnalysisStavros LitsosNo ratings yet
- Tanaka 2013 - Efficacy of Strengthening or Aerobic Exercise On Pain Relief in People With Knee OA - A Sys Review and Meta Analysis of RCTsDocument13 pagesTanaka 2013 - Efficacy of Strengthening or Aerobic Exercise On Pain Relief in People With Knee OA - A Sys Review and Meta Analysis of RCTsStavros LitsosNo ratings yet
- Shrek 2010 - Bone and ClaimbingDocument1 pageShrek 2010 - Bone and ClaimbingStavros LitsosNo ratings yet
- Michalopoulou 2013 - Physical Activity Is Associated With Bone Geometry of Premenarcheal Girls in A Dose-Depentant MannerDocument8 pagesMichalopoulou 2013 - Physical Activity Is Associated With Bone Geometry of Premenarcheal Girls in A Dose-Depentant MannerStavros LitsosNo ratings yet
- Delarue 2007 - Physical Exercise Supervised or Not by A PT in The Treatment of Lower-Limb OA - Elaboration of French Clinical Practice GuidelinesDocument10 pagesDelarue 2007 - Physical Exercise Supervised or Not by A PT in The Treatment of Lower-Limb OA - Elaboration of French Clinical Practice GuidelinesStavros LitsosNo ratings yet
- Hudelmaier 2001 - Age-Related Changes in The Morphology and Deformational Behavior of Knee Joint CartilageDocument6 pagesHudelmaier 2001 - Age-Related Changes in The Morphology and Deformational Behavior of Knee Joint CartilageStavros LitsosNo ratings yet
- Michalopoulou 2013 - Physical Activity Is Associated With Bone Geometry of Premenarcheal Girls in A Dose-Depentant MannerDocument8 pagesMichalopoulou 2013 - Physical Activity Is Associated With Bone Geometry of Premenarcheal Girls in A Dose-Depentant MannerStavros LitsosNo ratings yet
- Artrite e Exercício, Revisão PDFDocument11 pagesArtrite e Exercício, Revisão PDFRosaneLacerdaNo ratings yet
- Abbott 2015 - The Incremental Effects of Manual Therapy or Booster Sessions in Addition To Exercise Therapy For KneeOA - A RCTDocument9 pagesAbbott 2015 - The Incremental Effects of Manual Therapy or Booster Sessions in Addition To Exercise Therapy For KneeOA - A RCTStavros LitsosNo ratings yet
- Bricca 2019 - Impact of Exercise On Articular Cartilage in People at Risk of or With Established Knee OA - A Sys-Rev of RCTsDocument9 pagesBricca 2019 - Impact of Exercise On Articular Cartilage in People at Risk of or With Established Knee OA - A Sys-Rev of RCTsStavros LitsosNo ratings yet
- S.Litsos, E.Verzili Final Report - Muscle Activation During Cycling - Excercise PhysiologyDocument3 pagesS.Litsos, E.Verzili Final Report - Muscle Activation During Cycling - Excercise PhysiologyStavros LitsosNo ratings yet
- Delarue 2007 - Physical Exercise Supervised or Not by A PT in The Treatment of Lower-Limb OA - Elaboration of French Clinical Practice GuidelinesDocument10 pagesDelarue 2007 - Physical Exercise Supervised or Not by A PT in The Treatment of Lower-Limb OA - Elaboration of French Clinical Practice GuidelinesStavros LitsosNo ratings yet
- Balance Ability - Neuromuscular BiologyDocument7 pagesBalance Ability - Neuromuscular BiologyStavros LitsosNo ratings yet
- Patella Reflex - Neuromuscular BiologyDocument6 pagesPatella Reflex - Neuromuscular BiologyStavros LitsosNo ratings yet
- Bricca 2019 - Impact of Exercise On Articular Cartilage in People at Risk of or With Established Knee OA - A Sys-Rev of RCTsDocument9 pagesBricca 2019 - Impact of Exercise On Articular Cartilage in People at Risk of or With Established Knee OA - A Sys-Rev of RCTsStavros LitsosNo ratings yet
- Biomechanical Analysis - Kinisiology (Stavros Litsos)Document47 pagesBiomechanical Analysis - Kinisiology (Stavros Litsos)Stavros LitsosNo ratings yet
- Strength, Speed and Power - Exercise PhysiologyDocument47 pagesStrength, Speed and Power - Exercise PhysiologyStavros LitsosNo ratings yet
- S.Litsos, E.Verzili Laboratorium 1 - Frorce Platform - BiomechanicsDocument5 pagesS.Litsos, E.Verzili Laboratorium 1 - Frorce Platform - BiomechanicsStavros LitsosNo ratings yet
- Hearing and Visual Reaction - Neuromuscular BiologyDocument6 pagesHearing and Visual Reaction - Neuromuscular BiologyStavros LitsosNo ratings yet
- Muscle Fatigue - Exercise PhysiologyDocument18 pagesMuscle Fatigue - Exercise PhysiologyStavros LitsosNo ratings yet
- Metabolism - Exercise PhysiologyDocument49 pagesMetabolism - Exercise PhysiologyStavros Litsos100% (1)
- Vitamin and Mineral Contents of Gongronema Latifolium LeavesDocument3 pagesVitamin and Mineral Contents of Gongronema Latifolium LeavesFrida Febriani IsnanisafitriNo ratings yet
- Mvf404 Mhn-Seh2000w 956 b4 SiDocument2 pagesMvf404 Mhn-Seh2000w 956 b4 SiluisneiralopezNo ratings yet
- Definisi, Karakteristik dan Contoh Aplikasi SIGDocument28 pagesDefinisi, Karakteristik dan Contoh Aplikasi SIGtoyota taaNo ratings yet
- Anatomy of A Plated HoleDocument5 pagesAnatomy of A Plated Holepbs0707No ratings yet
- Material Safety Data Sheet: Chemtherm 550Document6 pagesMaterial Safety Data Sheet: Chemtherm 550Javier vaca villalbaNo ratings yet
- SampleDocument8 pagesSampleAntônioNo ratings yet
- 21st Century Science - Summer 2011 - The Universe Is CreativeDocument84 pages21st Century Science - Summer 2011 - The Universe Is CreativeMatthew EhretNo ratings yet
- Regulation 1 Regulation 2 Regulation 3 Regulation 4 Regulation 5 Regulation 6 Regulation 7 Regulation 8 Regulation 9 AppendixDocument10 pagesRegulation 1 Regulation 2 Regulation 3 Regulation 4 Regulation 5 Regulation 6 Regulation 7 Regulation 8 Regulation 9 AppendixAnonymous 7gJ9alpNo ratings yet
- Guía de Instalación y Programación: Sistema de Seguridad de 32 ZonasDocument68 pagesGuía de Instalación y Programación: Sistema de Seguridad de 32 ZonasfernanfivNo ratings yet
- Part 1Document52 pagesPart 1Jeffry Daud BarrungNo ratings yet
- Catalogo Tecnico Gb-S v07Document29 pagesCatalogo Tecnico Gb-S v07farou9 bmzNo ratings yet
- Types of swords from around the worldDocument4 pagesTypes of swords from around the worldДмитрий МихальчукNo ratings yet
- Final Nasir GlassDocument57 pagesFinal Nasir GlassShuvo Taufiq Ahmed100% (2)
- Nursing TheoriesDocument9 pagesNursing TheoriesMichelleneChenTadleNo ratings yet
- SE 276B Syllabus Winter 2018Document2 pagesSE 276B Syllabus Winter 2018Manu VegaNo ratings yet
- Dog Cake Recipe For Dozer's Birthday! - RecipeTin EatsDocument36 pagesDog Cake Recipe For Dozer's Birthday! - RecipeTin EatsZyreen Kate CataquisNo ratings yet
- Water Quality Notes: Alkalinity and Hardness: P. Chris WilsonDocument6 pagesWater Quality Notes: Alkalinity and Hardness: P. Chris WilsonrishabhNo ratings yet
- Quest The Last RemnantDocument67 pagesQuest The Last Remnantding suheNo ratings yet
- Preventive Maintenance Service Concept For SPACOM Product FamilyDocument27 pagesPreventive Maintenance Service Concept For SPACOM Product FamilyMiguel MarquesNo ratings yet
- 4.2 - Traditional Double-Walled HapaDocument25 pages4.2 - Traditional Double-Walled HapaThakur VeeruNo ratings yet
- CHAPTER-9, Respiration in Organisms.Document3 pagesCHAPTER-9, Respiration in Organisms.HarshitAhelani2379ScribdNo ratings yet
- What Is A Supply ChainDocument20 pagesWhat Is A Supply ChainThanh Binh Tran NguyenNo ratings yet
- Ac+lic Lab Manual 2018-19Document76 pagesAc+lic Lab Manual 2018-19Samanvi SaatviNo ratings yet
- Akbh PSK (V), TRBH As Y: AdhimokṣADocument8 pagesAkbh PSK (V), TRBH As Y: AdhimokṣA张晓亮No ratings yet
- A Feminist Analysis of Habba Khatoon'S Poetry: Dr. Mir Rifat NabiDocument7 pagesA Feminist Analysis of Habba Khatoon'S Poetry: Dr. Mir Rifat NabiShabir AhmadNo ratings yet
- PTC Document Status: (Updated 11 November 2015)Document5 pagesPTC Document Status: (Updated 11 November 2015)AndersonGabriel23No ratings yet
- ON Code (Aci 318-77) : Commentary Building Requirements For Reinforced ConcreteDocument132 pagesON Code (Aci 318-77) : Commentary Building Requirements For Reinforced ConcreteAzmi BazazouNo ratings yet
- Golden Dawn 2 9 The Moon BreathDocument4 pagesGolden Dawn 2 9 The Moon BreathF_RCNo ratings yet
- Fitness RX For Women - December 2013Document124 pagesFitness RX For Women - December 2013renrmrm100% (2)
- The Cactus and the SnowsDocument22 pagesThe Cactus and the SnowsCrisNo ratings yet