You might also like
- AS400 Config Audit Checklist Security BrigadeDocument4 pagesAS400 Config Audit Checklist Security BrigadeAlok DriveqNo ratings yet
- LFI CSE Fatal Incident at Qatar GasDocument1 pageLFI CSE Fatal Incident at Qatar Gasmalek sammoudiNo ratings yet
- MCBU - Lifting & Rigging Questions and AnswersDocument15 pagesMCBU - Lifting & Rigging Questions and AnswersBhaiJan59No ratings yet
- Chapter 6 Physics LabDocument3 pagesChapter 6 Physics Labraquelloveswow0% (1)
- APHIS DefensiveDriving 508 TestQuestionBankDocument6 pagesAPHIS DefensiveDriving 508 TestQuestionBankAna Célia Ferreira0% (1)
- HSE - Cirks Construction IncDocument87 pagesHSE - Cirks Construction IncCharlie OriasNo ratings yet
- Health Safety Coordinator Job DescriptionDocument1 pageHealth Safety Coordinator Job DescriptionB singhNo ratings yet
- Exposure to hand-arm and whole-body vibration from road drill useDocument3 pagesExposure to hand-arm and whole-body vibration from road drill usehogoshNo ratings yet
- Health, Safety, Security, Environment, and Quality PolicyDocument1 pageHealth, Safety, Security, Environment, and Quality PolicyVăn PhúcNo ratings yet
- Risk Assessment FundamentalsDocument13 pagesRisk Assessment FundamentalsKaito ShionNo ratings yet
- HSE Safety AuditsDocument3 pagesHSE Safety Auditsvlad100% (1)
- Risk Assessment TunnelDocument2 pagesRisk Assessment TunnelShauna LaycockNo ratings yet
- 1 45Document3 pages1 45nsadnan0% (1)
- ED2 SampleDocument53 pagesED2 SampleadelNo ratings yet
- 2 (MPH) Hazard Identification Risk Assessment and Control ProcedureDocument9 pages2 (MPH) Hazard Identification Risk Assessment and Control ProcedureLwandziso DlaminiNo ratings yet
- 2.8 HSE Training MatrixDocument2 pages2.8 HSE Training MatrixMuhammad HassaanNo ratings yet
- HSE Alert 105-21 Welder Finger InjuryDocument2 pagesHSE Alert 105-21 Welder Finger InjuryAlecs NedeaNo ratings yet
- Generic Mechanical Workshop Risk AssessmentDocument6 pagesGeneric Mechanical Workshop Risk AssessmentMohammad Abubakar SiddiqNo ratings yet
- Evaluation of Camp OHS Risks AssessmentDocument3 pagesEvaluation of Camp OHS Risks Assessmenthasanhse640No ratings yet
- Pera JackhammerDocument7 pagesPera Jackhammerjumansyahamid1988No ratings yet
- Employee Wwelfare ProjectDocument11 pagesEmployee Wwelfare ProjectVijay KishanNo ratings yet
- CHT 4331 - Chap 3 - Risk ManagementDocument12 pagesCHT 4331 - Chap 3 - Risk ManagementKatleho MohonoNo ratings yet
- Lesson Learned-HIPO Near Miss - Energy IsolationDocument1 pageLesson Learned-HIPO Near Miss - Energy IsolationMukeshNo ratings yet
- Hsps03 Working at HeightDDocument25 pagesHsps03 Working at HeightDZeinfahmi Dwireski WibawaNo ratings yet
- uJJ O: J.illDocument3 pagesuJJ O: J.illEngr.Syed AmjadNo ratings yet
- 7010 - Subcontractor Performance Assessment FormDocument4 pages7010 - Subcontractor Performance Assessment FormRifatRahmatullahNo ratings yet
- 1 Hse Management ResponsibilityDocument13 pages1 Hse Management ResponsibilityRATAN BHATIANo ratings yet
- Gotcha BrochureDocument6 pagesGotcha BrochureNurfirman HNo ratings yet
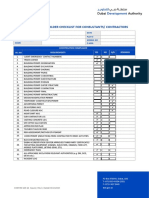
- Compliance Record Folder Checklist For Consultants/ ContractorsDocument1 pageCompliance Record Folder Checklist For Consultants/ ContractorsNijasNo ratings yet
- HSE Training ProgramDocument5 pagesHSE Training Programbotahra0% (1)
- Manual Kestrel 5400Document24 pagesManual Kestrel 5400Larissa JaramilloNo ratings yet
- Heat Stress GuidelinesDocument22 pagesHeat Stress Guidelinesgajeel1991No ratings yet
- Noise and Hearing Conservation TrainingDocument1 pageNoise and Hearing Conservation TrainingRabialtu SulihahNo ratings yet
- Mayon Hazardous SubstancesDocument14 pagesMayon Hazardous Substancesjerold esponillaNo ratings yet
- Lab Design Guide ChecklistDocument9 pagesLab Design Guide ChecklistTanveer AzizNo ratings yet
- Premobilisation Wheel Loader InspectionDocument1 pagePremobilisation Wheel Loader InspectionArjun Satheesan100% (1)
- Control Subtances Hazardous HealthDocument8 pagesControl Subtances Hazardous HealthrslapenaNo ratings yet
- OTC - Letter HeadDocument3 pagesOTC - Letter HeadEngr.Syed AmjadNo ratings yet
- Safety & Health Program 1Document20 pagesSafety & Health Program 1BuicheNo ratings yet
- MUDASSIRDocument1 pageMUDASSIRSn AhsanNo ratings yet
- F03-Appointment SupervisorDocument1 pageF03-Appointment SupervisorFarhat SetharNo ratings yet
- CRCC Office-Safety-Inspection-ChecklistDocument2 pagesCRCC Office-Safety-Inspection-ChecklistSyed Amjad100% (1)
- Guide Lines For NSC HSE PlanDocument52 pagesGuide Lines For NSC HSE Planജിനാദ് അബ്ദുസ്സലാംNo ratings yet
- Young Persons Risk Assessment V2.0 October 2021Document2 pagesYoung Persons Risk Assessment V2.0 October 2021Lucas SantosNo ratings yet
- FUSHAN TECH SAFETY PROCEDUREDocument11 pagesFUSHAN TECH SAFETY PROCEDUREhoangmtbNo ratings yet
- IGC 2 Slide ReviewDocument83 pagesIGC 2 Slide ReviewaliNo ratings yet
- Confined Spaces CardsDocument1 pageConfined Spaces CardsJafar KhanNo ratings yet
- Safety Moment There Is No Shortcut To Safety 448cuoDocument6 pagesSafety Moment There Is No Shortcut To Safety 448cuoInnocent BhaikwaNo ratings yet
- Code of PracticeDocument26 pagesCode of PracticeS Khan100% (1)
- HSE Alert - LTI Fall From Heights TBTDocument12 pagesHSE Alert - LTI Fall From Heights TBTrodman823No ratings yet
- REGDOC2 1 2 Safety Culture Final EngDocument31 pagesREGDOC2 1 2 Safety Culture Final Engnagatopein6No ratings yet
- Msc-Qhsef-04 Masterlist - Documents and RecordsDocument4 pagesMsc-Qhsef-04 Masterlist - Documents and RecordsAdil Abdulkhader100% (1)
- Ventilation Plan TemplateDocument11 pagesVentilation Plan TemplatePlank89No ratings yet
- How To Conduct Workplace Inspections: A Health and Safety Guideline For Your WorkplaceDocument6 pagesHow To Conduct Workplace Inspections: A Health and Safety Guideline For Your WorkplacemashanghNo ratings yet
- Safety ProgramDocument21 pagesSafety ProgramSits RdddNo ratings yet
- Aramco Approved Gas Plant and Refinery ProjectsDocument4 pagesAramco Approved Gas Plant and Refinery ProjectsManda Khel Apna DesNo ratings yet
- Civil Engineer with 18 Years ExperienceDocument4 pagesCivil Engineer with 18 Years Experiencepasser byNo ratings yet
- Working at Height PresentationDocument11 pagesWorking at Height PresentationAbdul Hameed OmarNo ratings yet
- Mashooq CV (Updated)Document3 pagesMashooq CV (Updated)Manda Khel Apna DesNo ratings yet
- EHS Calendar September 2019 Training Fire Safety PPE AuditsDocument1 pageEHS Calendar September 2019 Training Fire Safety PPE AuditsSiddharth RanaNo ratings yet
- Assignment Safety Report WALTON Factory Mahmudul HaqueDocument28 pagesAssignment Safety Report WALTON Factory Mahmudul Haquepunter07No ratings yet
- Bayyinat ArticleDocument4 pagesBayyinat ArticleHamzaNoumanNo ratings yet
- Best Practices in Machinery InstallationDocument2 pagesBest Practices in Machinery InstallationHamzaNoumanNo ratings yet
- 2005 Nondestructive Testing Guide Equipment Condition AssessmentDocument8 pages2005 Nondestructive Testing Guide Equipment Condition AssessmentHamzaNoumanNo ratings yet
- Balance Plot FormDocument1 pageBalance Plot FormHamzaNoumanNo ratings yet
- Helium Leak Detector vs Pressure Decay Leak Testing MethodsDocument2 pagesHelium Leak Detector vs Pressure Decay Leak Testing MethodsHamzaNoumanNo ratings yet
- Shift 2 Schedule (Sept 12 - Sept 20 '22)Document1 pageShift 2 Schedule (Sept 12 - Sept 20 '22)HamzaNoumanNo ratings yet
- The ABC of NDTDocument5 pagesThe ABC of NDTHamzaNoumanNo ratings yet
- Acceptance Criteria of Weld Defects As Per Different CodesDocument17 pagesAcceptance Criteria of Weld Defects As Per Different CodesShubham ShuklaNo ratings yet
- H Hole MesaurmentDocument2 pagesH Hole MesaurmentHamzaNoumanNo ratings yet
- Congratulations On Your Completion: Hamza NomanDocument1 pageCongratulations On Your Completion: Hamza NomanHamzaNoumanNo ratings yet
- Fluid Handling System PriceDocument2 pagesFluid Handling System PriceHamzaNoumanNo ratings yet
- Nbo-Tc NewDocument24 pagesNbo-Tc NewHamzaNoumanNo ratings yet
- Certificate of Completion: Hafiz NomanDocument1 pageCertificate of Completion: Hafiz NomanHamzaNoumanNo ratings yet
- Confirmation - Check-InDocument1 pageConfirmation - Check-InHamzaNoumanNo ratings yet
- MC LiftRigBestPractices Poster 11X17Document1 pageMC LiftRigBestPractices Poster 11X17HamzaNoumanNo ratings yet
- 7 22 2022 Mech - 19596Document1 page7 22 2022 Mech - 19596HamzaNoumanNo ratings yet
- Onboarding Checklist: Best Practices for a Smooth StartDocument1 pageOnboarding Checklist: Best Practices for a Smooth StartHamzaNoumanNo ratings yet
- Scaffolding: Submitted By, Akhilesh.A Production Operator (TR), Forbes Bumiarmada LimitedDocument42 pagesScaffolding: Submitted By, Akhilesh.A Production Operator (TR), Forbes Bumiarmada LimitedHamzaNoumanNo ratings yet
- Cylinder Test-Certification-ProceduresDocument3 pagesCylinder Test-Certification-ProceduresHamzaNoumanNo ratings yet
- Calculate your daily water intake based on weightDocument7 pagesCalculate your daily water intake based on weightSuyenthan SathishNo ratings yet
- Manpower Workshop Garage CraftDocument7 pagesManpower Workshop Garage CraftHamzaNoumanNo ratings yet
- Sr. No. Description Unit: Workshop / Garage Craft IssuesDocument14 pagesSr. No. Description Unit: Workshop / Garage Craft IssuesHamzaNoumanNo ratings yet
- Contract Extension of Hafiz Hussain 2021Document2 pagesContract Extension of Hafiz Hussain 2021HamzaNoumanNo ratings yet
- Advance Cash For Cricket PitchDocument1 pageAdvance Cash For Cricket PitchHamzaNoumanNo ratings yet
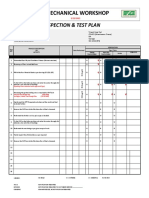
- Mechanical Workshop: Inspection & Test PlanDocument4 pagesMechanical Workshop: Inspection & Test PlanHamzaNoumanNo ratings yet
- JSA For Woma Jet TestingDocument2 pagesJSA For Woma Jet TestingHamzaNoumanNo ratings yet
- D Level Safety Meeting Quality Checklist - RevisedDocument1 pageD Level Safety Meeting Quality Checklist - RevisedHamzaNoumanNo ratings yet
- Pakarab Fertilizers IT Help Desk FormDocument1 pagePakarab Fertilizers IT Help Desk FormHamzaNoumanNo ratings yet
- Incident / Injury Occurrence Report Part A:: Form No: SAF/2/001 Date Prepared: 29 / 09 / 08 Revision: 00Document2 pagesIncident / Injury Occurrence Report Part A:: Form No: SAF/2/001 Date Prepared: 29 / 09 / 08 Revision: 00HamzaNoumanNo ratings yet
- Regional Campus The English and Foreign Languages UniversityDocument2 pagesRegional Campus The English and Foreign Languages UniversitySidra KhanNo ratings yet
- HTML MCQDocument22 pagesHTML MCQBuxar Students LifeNo ratings yet
- CPA Review Module on Accounting Standards and RegulationDocument13 pagesCPA Review Module on Accounting Standards and RegulationLuiNo ratings yet
- Roof Beam Layout - r1Document1 pageRoof Beam Layout - r1Niraj ShindeNo ratings yet
- Saura, Jasmin E. - DVM - 2B Biochemistry (Activity 2)Document2 pagesSaura, Jasmin E. - DVM - 2B Biochemistry (Activity 2)Jasmin SauraNo ratings yet
- Inv 069 1701757527Document1 pageInv 069 1701757527neetu9414576916No ratings yet
- DGN ExamDocument5 pagesDGN ExamMaiga Ayub HusseinNo ratings yet
- Chapter 3 Week 1 Inductive and Deductive ReasoningDocument57 pagesChapter 3 Week 1 Inductive and Deductive ReasoningDiane Agcaoili Edra50% (6)
- Customer Satisfaction in Maruti SuzukiDocument31 pagesCustomer Satisfaction in Maruti Suzukirajesh laddha100% (1)
- Sample Resume For HRDocument2 pagesSample Resume For HRnapinnvoNo ratings yet
- Age Hardening Gold Alloys For JewelryDocument4 pagesAge Hardening Gold Alloys For JewelryReinol Eko SianturiNo ratings yet
- GogikavofobifigukidonDocument2 pagesGogikavofobifigukidonMd. Bepul HossainNo ratings yet
- Axial Centrifugal FansDocument15 pagesAxial Centrifugal FansAhsan JavedNo ratings yet
- MdmedichaoiceDocument324 pagesMdmedichaoicelancastd54No ratings yet
- Diosdado MacapagalDocument13 pagesDiosdado MacapagalMermie ArmentaNo ratings yet
- Metal Expansion Joint 2020 v2 20MBDocument116 pagesMetal Expansion Joint 2020 v2 20MBanni trejoNo ratings yet
- Dear Boy (Acordes para Cancion)Document4 pagesDear Boy (Acordes para Cancion)Rodolfo GuglielmoNo ratings yet
- Aling Presing ChichacornDocument2 pagesAling Presing ChichacornMhel Joshua Bautista HermitanioNo ratings yet
- LC1D150M7: Product Data SheetDocument3 pagesLC1D150M7: Product Data SheetTrong Hung NguyenNo ratings yet
- San Lam Stratus FundsDocument2 pagesSan Lam Stratus FundsTiso Blackstar GroupNo ratings yet
- Frogkisser! by Garth Nix (Excerpt)Document17 pagesFrogkisser! by Garth Nix (Excerpt)I Read YA0% (1)
- Telangana Energy Dept Contact NumbersDocument27 pagesTelangana Energy Dept Contact Numbersstarpowerzloans rjyNo ratings yet
- React Rich Text EditorDocument3 pagesReact Rich Text Editordhirendrapratapsingh398No ratings yet
- Lifeboat Equipment ListDocument1 pageLifeboat Equipment Listjosua albertNo ratings yet
- B1 UDO Trace LogDocument14 pagesB1 UDO Trace LogCh M KashifNo ratings yet
- Hajipur Resume GVVDocument2 pagesHajipur Resume GVVRajnish JhaNo ratings yet
- Data Sheet Ads1292rDocument69 pagesData Sheet Ads1292rKaha SyawalNo ratings yet
- Sunday School Lesson Activity 219 Moses Builds A Tablernacle in The Wilderness - Printable 3D Model KitDocument17 pagesSunday School Lesson Activity 219 Moses Builds A Tablernacle in The Wilderness - Printable 3D Model Kitmcontrerasseitz3193No ratings yet