You might also like
- COVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19From EverandCOVID-19 Mortality Review in Malaysia & Updates on Clinical Management of COVID-19No ratings yet
- Anticoagulation in COVID-19: A Systematic Review and Rapid GuidanceDocument20 pagesAnticoagulation in COVID-19: A Systematic Review and Rapid GuidanceAndi Tiara S. AdamNo ratings yet
- Covid-19 and Coagulation: Bleeding and Thrombotic Manifestations of Sars-Cov-2 InfectionDocument12 pagesCovid-19 and Coagulation: Bleeding and Thrombotic Manifestations of Sars-Cov-2 InfectionDavid Mamani CardenasNo ratings yet
- Saving Critically Ill COVID-19 Patients With Mechanical Circulatory SupportDocument11 pagesSaving Critically Ill COVID-19 Patients With Mechanical Circulatory SupportSara MendesNo ratings yet
- Neutrofilos y LinfocitosDocument2 pagesNeutrofilos y LinfocitosOscarNo ratings yet
- The Hemocyte Counts As A Potential Biomarker For Predicting Disease Progression in COVID-19: A Retrospective StudyDocument10 pagesThe Hemocyte Counts As A Potential Biomarker For Predicting Disease Progression in COVID-19: A Retrospective StudygiovannaNo ratings yet
- Chakra - Factors Associated With Complications of C DiffDocument8 pagesChakra - Factors Associated With Complications of C DiffCherry SmileNo ratings yet
- Ahead of Print: Establishment of Diagnostic Protocols For COVID-19 PatientsDocument6 pagesAhead of Print: Establishment of Diagnostic Protocols For COVID-19 PatientsSana AbbasNo ratings yet
- Meta 8Document9 pagesMeta 8Jonathan AiresNo ratings yet
- Stem Cell Exosomes Show Promise for Treating Severe COVID-19Document8 pagesStem Cell Exosomes Show Promise for Treating Severe COVID-19Alejandro Andrés Salazar GuzmánNo ratings yet
- Mortality & Recurrent Seizure Risk After New-Onset Seizure in HIV-positive Zambian AdultsDocument10 pagesMortality & Recurrent Seizure Risk After New-Onset Seizure in HIV-positive Zambian AdultsAdam PrabataNo ratings yet
- Research Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology FindingsDocument9 pagesResearch Article: Neutropenic Sepsis in The ICU: Outcome Predictors in A Two-Phase Model and Microbiology Findings28121998No ratings yet
- A Study Oncytopenias and The Factors Associated With Cytopenias Among Hiv Infected Patients Admitted at A Tertiary Care HospitalDocument8 pagesA Study Oncytopenias and The Factors Associated With Cytopenias Among Hiv Infected Patients Admitted at A Tertiary Care HospitalIJAR JOURNALNo ratings yet
- RISK of Thromboembolism in Patient With Covid 19 MétaanalysisDocument14 pagesRISK of Thromboembolism in Patient With Covid 19 MétaanalysisDelgado OnthemixNo ratings yet
- A Novel Severity Score To Predict Inpatient Mortality in COVID 19 PatientsDocument8 pagesA Novel Severity Score To Predict Inpatient Mortality in COVID 19 PatientsanscstNo ratings yet
- Teori Eosinopenia DewasaDocument7 pagesTeori Eosinopenia DewasaNurlyanti RustamNo ratings yet
- 2023 - Epidemiology and Outcomes of Hospital Acquired Bloodstream Infections in Intensive Care Unit Patients The EUROBACT 2Document13 pages2023 - Epidemiology and Outcomes of Hospital Acquired Bloodstream Infections in Intensive Care Unit Patients The EUROBACT 2giseladlrNo ratings yet
- Management of Therapeutic Unfractionated Heparin in COVID-19 Patients: A Retrospective Cohort StudyDocument11 pagesManagement of Therapeutic Unfractionated Heparin in COVID-19 Patients: A Retrospective Cohort StudyAriqa AzzhraNo ratings yet
- Pi Is 2352302621001058Document10 pagesPi Is 2352302621001058Вадим ЖебельNo ratings yet
- 4Document16 pages4Ihsanul Ma'arifNo ratings yet
- InternacionalDocument9 pagesInternacionalbryan ronaldNo ratings yet
- ArtículosDocument8 pagesArtículosPAOLA DICETH GARCIA OLGUINNo ratings yet
- JMV 9999 NaDocument10 pagesJMV 9999 NaNurul AzizahNo ratings yet
- 08 PJP Vol8+no1 PJP+08-01-OA-01 8ppDocument8 pages08 PJP Vol8+no1 PJP+08-01-OA-01 8pprachelNo ratings yet
- Chest CT in COVID-19 Pneumonia: What Are The Findings in Mid-Term Follow-Up?Document9 pagesChest CT in COVID-19 Pneumonia: What Are The Findings in Mid-Term Follow-Up?rishaNo ratings yet
- Artikel Covid-19Document9 pagesArtikel Covid-19nhshivani532000No ratings yet
- Manejo de CoagulopatiaDocument4 pagesManejo de CoagulopatiaSMIBA MedicinaNo ratings yet
- 10 1016@j Jaad 2019 05 096Document8 pages10 1016@j Jaad 2019 05 096JohnNo ratings yet
- Rüthrich2021 Article COVID-19InCancerPatientsClinicDocument11 pagesRüthrich2021 Article COVID-19InCancerPatientsClinicdianaNo ratings yet
- Coagulopathy and Thrombosis As A Result of Severe COVID-19 Infection: A Microvascular FocusDocument12 pagesCoagulopathy and Thrombosis As A Result of Severe COVID-19 Infection: A Microvascular FocusNathalia AzuosNo ratings yet
- Barnes2020 Article ThromboembolismAndAnticoagulanDocument10 pagesBarnes2020 Article ThromboembolismAndAnticoagulanRirin Efsa JutiaNo ratings yet
- Ipp 6 E08Document6 pagesIpp 6 E08retnoNo ratings yet
- Estudo DiabetesDocument9 pagesEstudo DiabetesFulano de TalNo ratings yet
- Procalcitonin and Secondary Bacterial InfectionsDocument6 pagesProcalcitonin and Secondary Bacterial Infectionsadrifen adriNo ratings yet
- Pi Is 1083879118313909Document2 pagesPi Is 1083879118313909Ljc JaslinNo ratings yet
- 10.5811@westjem.2020.6.47919 (2) 81105Document7 pages10.5811@westjem.2020.6.47919 (2) 81105Giovan GaulNo ratings yet
- Koni 10 1854424Document13 pagesKoni 10 1854424Simona VisanNo ratings yet
- Molecular Diversity Analysis Using SSR MarkersDocument12 pagesMolecular Diversity Analysis Using SSR Markersrushi tahakikNo ratings yet
- NAC Torres 2019Document13 pagesNAC Torres 2019Stephany MontoyaNo ratings yet
- Articulo Trombocitipenia Por Vacuna CovidDocument10 pagesArticulo Trombocitipenia Por Vacuna CovidAlex de la RNo ratings yet
- A Critical Review - Blood and Clinical Hematology Disorders in Covid-19Document6 pagesA Critical Review - Blood and Clinical Hematology Disorders in Covid-19Nurihsani 01No ratings yet
- Journal Pone 0252599Document12 pagesJournal Pone 0252599sririniaNo ratings yet
- Systemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyDocument37 pagesSystemic Immune-In Ammatory Index Predicts Prognosis of Patients With COVID-19: A Retrospective StudyJuliana SanjayaNo ratings yet
- Clinical Profile and Microbiological Aetiology Diagnosis in Adult Patients Hospitalized With Community-Acquired PneumoniaDocument10 pagesClinical Profile and Microbiological Aetiology Diagnosis in Adult Patients Hospitalized With Community-Acquired PneumoniahajajNo ratings yet
- 1 s2.0 S0012369220342872 MainDocument12 pages1 s2.0 S0012369220342872 Mainganda gandaNo ratings yet
- MainDocument14 pagesMainDoménica SánchezNo ratings yet
- Usefulness of Presepsin As A Diagnostic and Prognostic Marker of Sepsis in Daily Clinical PracticeDocument7 pagesUsefulness of Presepsin As A Diagnostic and Prognostic Marker of Sepsis in Daily Clinical Practicefaraz.mirza1No ratings yet
- Covid 10Document14 pagesCovid 10jenifer paathNo ratings yet
- Diagnose of BSIDocument12 pagesDiagnose of BSIWong Chun ShengNo ratings yet
- Determining Which Hospitalized Coronavirus Disease 2019 Patients Require Urgent EchocardiographyDocument8 pagesDetermining Which Hospitalized Coronavirus Disease 2019 Patients Require Urgent EchocardiographyMarco Antonio Viera ArevaloNo ratings yet
- 394 Full PDFDocument20 pages394 Full PDFHaltiNo ratings yet
- Antibiotic Prescribing Patterns at COVID-19 Dedicated Wards in Bangladesh: Findings From A Single Center StudyDocument5 pagesAntibiotic Prescribing Patterns at COVID-19 Dedicated Wards in Bangladesh: Findings From A Single Center Studyاحمد عرفاتNo ratings yet
- Potential Pathogenic Mechanisms Involved in The As PDFDocument8 pagesPotential Pathogenic Mechanisms Involved in The As PDFEndah KusumaNo ratings yet
- Covid Asociado A CoagulopatiaDocument2 pagesCovid Asociado A CoagulopatiaNahui IcatlNo ratings yet
- Does Baseline Diuretics Use Affect Prognosis in Patients With COVID-19?Document6 pagesDoes Baseline Diuretics Use Affect Prognosis in Patients With COVID-19?Muhammad Halil GibranNo ratings yet
- Jurnal 7Document4 pagesJurnal 7Ariqa AzzhraNo ratings yet
- Hospital-Acquired Pneumonia in Critically Ill Children: Incidence, Risk Factors, Outcome and Diagnosis With Insight On The Novel Diagnostic Technique of Multiplex Polymerase Chain ReactionDocument7 pagesHospital-Acquired Pneumonia in Critically Ill Children: Incidence, Risk Factors, Outcome and Diagnosis With Insight On The Novel Diagnostic Technique of Multiplex Polymerase Chain ReactionadhitiaNo ratings yet
- Ciz 1049Document9 pagesCiz 1049Justin WilliemNo ratings yet
- Lopes 2020Document11 pagesLopes 2020some buddyyNo ratings yet
- Effectiveness of Quinolone ProphylaxisDocument15 pagesEffectiveness of Quinolone ProphylaxisDeski MadeNo ratings yet
- Emergencies in Diabetes: Zulfachmi WahabDocument33 pagesEmergencies in Diabetes: Zulfachmi WahablidawatiNo ratings yet
- Tafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahDocument22 pagesTafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahlidawatiNo ratings yet
- Tafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahDocument22 pagesTafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahlidawatiNo ratings yet
- Hubungan Antara Gaya Belajar, Kemandirian Belajar, Dan Minat Belajar Dengan Hasil Belajar Biologi SiswaDocument8 pagesHubungan Antara Gaya Belajar, Kemandirian Belajar, Dan Minat Belajar Dengan Hasil Belajar Biologi SiswalidawatiNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument13 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistslidawatiNo ratings yet
- 2019 (Covid-19) Dengan HipertensiDocument6 pages2019 (Covid-19) Dengan HipertensilidawatiNo ratings yet
- Tafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahDocument22 pagesTafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahlidawatiNo ratings yet
- Hypertension Linked to Stroke RiskDocument4 pagesHypertension Linked to Stroke RisklidawatiNo ratings yet
- 1 SM PDFDocument4 pages1 SM PDFDaris UntoroNo ratings yet
- C-Reactive Protein Levels of Sepsis Patients: A Comparison of Three Immunoassay MethodsDocument5 pagesC-Reactive Protein Levels of Sepsis Patients: A Comparison of Three Immunoassay MethodslidawatiNo ratings yet
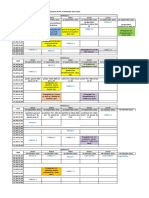
- Jadwal Blok 19 Edited 1Document2 pagesJadwal Blok 19 Edited 1lidawatiNo ratings yet
- (Inggris) D-Dimer DiomarkerDocument11 pages(Inggris) D-Dimer DiomarkerlidawatiNo ratings yet
- Hubungan Antara Lama Penggunaan Aspirin Dengan Nilai Agregasi Trombosit Pada Pasien Hipertensi Di Rsup Prof. Dr. R. D. Kandou ManadoDocument6 pagesHubungan Antara Lama Penggunaan Aspirin Dengan Nilai Agregasi Trombosit Pada Pasien Hipertensi Di Rsup Prof. Dr. R. D. Kandou ManadoDewina Dyani RosariNo ratings yet
- Tafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahDocument22 pagesTafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahlidawatiNo ratings yet
- Clinical Pathology and Medical Laboratory: Indonesian Journal ofDocument8 pagesClinical Pathology and Medical Laboratory: Indonesian Journal oflidawatiNo ratings yet
- Hypertension Linked to Stroke RiskDocument4 pagesHypertension Linked to Stroke RisklidawatiNo ratings yet
- MEDIKA TADULAKO, Jurnal Ilmiah Kedokteran, Vol. 4 No. 1: Januari 2017Document10 pagesMEDIKA TADULAKO, Jurnal Ilmiah Kedokteran, Vol. 4 No. 1: Januari 2017lidawatiNo ratings yet
- 1 s2.0 S0924857920301059 MainDocument13 pages1 s2.0 S0924857920301059 MainNini RinNo ratings yet
- Xu2020 Article MechanismOfThrombocytopeniaInCDocument4 pagesXu2020 Article MechanismOfThrombocytopeniaInClidawatiNo ratings yet
- Trombositopenia Dan Trombosis Pada Pasien Rawat Inap Dengan COVID-19Document3 pagesTrombositopenia Dan Trombosis Pada Pasien Rawat Inap Dengan COVID-19lidawatiNo ratings yet
- (Inggris) D-Dimer Antigen Konsep Dan Prospek Ke DepanDocument10 pages(Inggris) D-Dimer Antigen Konsep Dan Prospek Ke DepanlidawatiNo ratings yet
- IFCC Interim Guidelines On Biochemical/ Hematological Monitoring of COVID-19 PatientsDocument8 pagesIFCC Interim Guidelines On Biochemical/ Hematological Monitoring of COVID-19 PatientslidawatiNo ratings yet
- D-dimer and platelet aggregation predict thrombotic risk in PADDocument8 pagesD-dimer and platelet aggregation predict thrombotic risk in PADlidawatiNo ratings yet
- Trombositopenia Dan Trombosis Pada Pasien Rawat Inap Dengan COVID-19Document3 pagesTrombositopenia Dan Trombosis Pada Pasien Rawat Inap Dengan COVID-19lidawatiNo ratings yet
- Andreas C. Widjaja-01Document9 pagesAndreas C. Widjaja-01Legina AdityaNo ratings yet
- (Inggris) D-Dimer ElevationDocument19 pages(Inggris) D-Dimer ElevationlidawatiNo ratings yet
- (Inggris) Hubungan D-Dimer Dan Tekanan DarahDocument6 pages(Inggris) Hubungan D-Dimer Dan Tekanan DarahlidawatiNo ratings yet
- The D-Dimer Assay: Eric D. Johnson - John C. Schell - George M. RodgersDocument7 pagesThe D-Dimer Assay: Eric D. Johnson - John C. Schell - George M. RodgerslidawatiNo ratings yet
- E 6Document4 pagesE 6Gus RintoNo ratings yet
- Sridhar 2016Document6 pagesSridhar 2016Desmiyati AdoeNo ratings yet
- FacebookH Cking 1 3 (SFILEDocument10 pagesFacebookH Cking 1 3 (SFILEFitra AkbarNo ratings yet
- Shooting ScriptDocument12 pagesShooting Scriptapi-544851273No ratings yet
- M.Com Second Semester – Advanced Cost Accounting MCQDocument11 pagesM.Com Second Semester – Advanced Cost Accounting MCQSagar BangreNo ratings yet
- Cebuano LanguageDocument15 pagesCebuano LanguageIsla PageNo ratings yet
- Sato Printer Api Reference DocumentDocument34 pagesSato Printer Api Reference Documentsupersteel.krwNo ratings yet
- Construction Materials and Testing: "WOOD"Document31 pagesConstruction Materials and Testing: "WOOD"Aira Joy AnyayahanNo ratings yet
- Olt CliDocument2 pagesOlt CliMohammad SaeedNo ratings yet
- Physical Science 1Document25 pagesPhysical Science 1EJ RamosNo ratings yet
- CHM131 Presentation - Oxidation of MetalsDocument11 pagesCHM131 Presentation - Oxidation of MetalsNazrul ShahNo ratings yet
- Technology Class ResumeDocument4 pagesTechnology Class Resumeapi-259588430No ratings yet
- Effect of Upstream Dam Geometry On Peak Discharge During Overtopping Breach in Noncohesive Homogeneous Embankment Dams Implications For Tailings DamsDocument22 pagesEffect of Upstream Dam Geometry On Peak Discharge During Overtopping Breach in Noncohesive Homogeneous Embankment Dams Implications For Tailings DamsHelvecioNo ratings yet
- CBK Test QuestionsDocument2 pagesCBK Test QuestionsMehul GuptaNo ratings yet
- 7 - NIBL - G.R. No. L-15380 Wan V Kim - DigestDocument1 page7 - NIBL - G.R. No. L-15380 Wan V Kim - DigestOjie SantillanNo ratings yet
- A Review of The Management of Cerebral Vasospasm After Aneurysmal Subarachnoid HemorrhageDocument15 pagesA Review of The Management of Cerebral Vasospasm After Aneurysmal Subarachnoid HemorrhageAlanNo ratings yet
- St. Anthony College Calapan City Syllabus: Course DescriptionDocument6 pagesSt. Anthony College Calapan City Syllabus: Course DescriptionAce HorladorNo ratings yet
- Optical Fiber Communication Case Study on Material DispersionDocument5 pagesOptical Fiber Communication Case Study on Material DispersionAyush SharmaNo ratings yet
- Divisional Chart-IDocument1 pageDivisional Chart-Iabhisek1987No ratings yet
- Assessmentof Safety Cultureand Maturityin Mining Environments Caseof Njuli QuarryDocument12 pagesAssessmentof Safety Cultureand Maturityin Mining Environments Caseof Njuli QuarryAbdurrohman AabNo ratings yet
- Format of Synopsis - Project - 1Document5 pagesFormat of Synopsis - Project - 1euforia hubNo ratings yet
- READMEDocument3 pagesREADMERadu TimisNo ratings yet
- AlternatorDocument3 pagesAlternatorVatsal PatelNo ratings yet
- Determination of Atenolol in Pharmaceutical Dosages by Fourier Transform Infrared Spectrometry (FTIR)Document11 pagesDetermination of Atenolol in Pharmaceutical Dosages by Fourier Transform Infrared Spectrometry (FTIR)Geovas GomezNo ratings yet
- Password ManagementDocument7 pagesPassword ManagementNeerav KrishnaNo ratings yet
- An Introduction To Log ShootingDocument10 pagesAn Introduction To Log ShootingSorin GociuNo ratings yet
- What Is Your Road, Man?Document232 pagesWhat Is Your Road, Man?Oana AndreeaNo ratings yet
- Design and Analysis of Buck ConverterDocument18 pagesDesign and Analysis of Buck Converterk rajendraNo ratings yet
- Retrenchment StrategiesDocument3 pagesRetrenchment StrategiesSABRI AKBAL MOHAMED HASSAN100% (3)
- Desk PiDocument21 pagesDesk PiThan LwinNo ratings yet
- Red Lion Edict-97 - Manual PDFDocument282 pagesRed Lion Edict-97 - Manual PDFnaminalatrukNo ratings yet
- Climate Change Survivor GameDocument22 pagesClimate Change Survivor Game许凉发No ratings yet