You might also like
- 180 Degree DiabetesDocument111 pages180 Degree DiabetesJoRa71No ratings yet
- Home Power Magazine - Issue 011 - 1989-06-07 PDFDocument56 pagesHome Power Magazine - Issue 011 - 1989-06-07 PDFwienslaw5804No ratings yet
- Diabetes Conversation Maps: Journey To Better Diabetes EducationDocument1 pageDiabetes Conversation Maps: Journey To Better Diabetes EducationCenter for Managing Chronic DiseaseNo ratings yet
- Acute Chronic ComplicationDocument49 pagesAcute Chronic ComplicationMuhammad DaviqNo ratings yet
- Diabetes Complication LectureDocument63 pagesDiabetes Complication LectureDoni MarthenNo ratings yet
- Diabetes Management: OverviewDocument20 pagesDiabetes Management: Overviewlaloo01No ratings yet
- How Is Diabetes Managed?: Type 1 and Type 2 Diabetes ORDocument2 pagesHow Is Diabetes Managed?: Type 1 and Type 2 Diabetes ORdebabrata5976No ratings yet
- How Does Social Media Advertising Persuade An Investigation of The Moderation Effects of Corporate Reputation Privacy Concerns and Intrusiveness PDFDocument21 pagesHow Does Social Media Advertising Persuade An Investigation of The Moderation Effects of Corporate Reputation Privacy Concerns and Intrusiveness PDFMaryam KhaliqNo ratings yet
- Diabetes KetoacidosisDocument23 pagesDiabetes KetoacidosisSalman MajidNo ratings yet
- NSAIDs, DMARDs, Analgesics & Gout DrugsDocument114 pagesNSAIDs, DMARDs, Analgesics & Gout DrugsMani Jee100% (1)
- Last Days of Diabetes Chaper 4Document39 pagesLast Days of Diabetes Chaper 4vtrackNo ratings yet
- Find Diabitis Revrsal Prog3Document2 pagesFind Diabitis Revrsal Prog3Jani AmitkumarNo ratings yet
- The basics of how solar panels workDocument8 pagesThe basics of how solar panels workBishal LamichhaneNo ratings yet
- Diabetes Up Date 2009Document115 pagesDiabetes Up Date 2009Stefani NoviliaNo ratings yet
- Diabetes - Who - Embargoed Who Global Report On DiabetesDocument88 pagesDiabetes - Who - Embargoed Who Global Report On DiabetesFatima ShahidNo ratings yet
- Dodging Diabetes ComplicationsDocument20 pagesDodging Diabetes ComplicationsUlises MatiasNo ratings yet
- Type 2 Diabetes Mellitus (T2DM) Adult Treatment PathwayDocument2 pagesType 2 Diabetes Mellitus (T2DM) Adult Treatment PathwayFaidil Akbar100% (1)
- 3D Solar Cell Technology PresentationDocument15 pages3D Solar Cell Technology PresentationPankaj DeshmukhNo ratings yet
- Diabetes InformationDocument171 pagesDiabetes Informationtheia28No ratings yet
- Diabetes Millitus PDFDocument41 pagesDiabetes Millitus PDFAbdullah BhattiNo ratings yet
- TEACHING OF DIABETES MELLITUSDocument4 pagesTEACHING OF DIABETES MELLITUSpearl_nursingNo ratings yet
- LG LCD TV SERVICE MANUAL 15lc1rzgDocument36 pagesLG LCD TV SERVICE MANUAL 15lc1rzgStefanoViganóNo ratings yet
- How EXERCISE Helps Control DiabetesDocument23 pagesHow EXERCISE Helps Control DiabetesApurba MukherjeeNo ratings yet
- LG 37lb1da LCD TV Service ManualDocument83 pagesLG 37lb1da LCD TV Service ManualEdwin BenitezNo ratings yet
- 7-dayGDM Mealplan Oct292021 FNL1115Document5 pages7-dayGDM Mealplan Oct292021 FNL1115Vera HoNo ratings yet
- Molecular Basis of Type 2 DiabetesDocument22 pagesMolecular Basis of Type 2 DiabetespimpellerNo ratings yet
- Diabetes Type 2 Treatment AlgorithmDocument25 pagesDiabetes Type 2 Treatment AlgorithmJ Wong100% (1)
- IoT Based Elderly Healthcare Monitoring SystemDocument11 pagesIoT Based Elderly Healthcare Monitoring SystemIJRASETPublicationsNo ratings yet
- Diabetes PPT FianlDocument31 pagesDiabetes PPT FianlUqba MishalNo ratings yet
- Diabetes Management.Document24 pagesDiabetes Management.Hasrul Muslih0% (1)
- Problem Solving NewDocument25 pagesProblem Solving NewAswathy AswathyNo ratings yet
- Understanding DiabetesDocument13 pagesUnderstanding DiabetesBratatiNo ratings yet
- Diabetes Mellitus CuredDocument12 pagesDiabetes Mellitus CuredsherryNo ratings yet
- Solar Energy: ContentDocument15 pagesSolar Energy: ContentAnonymous Apt8lLHmYNo ratings yet
- Juegos para La ClaseDocument359 pagesJuegos para La Clasedpapalia3744No ratings yet
- QR Management of Type 2 Diabetes Mellitus (5th Edition) PDFDocument8 pagesQR Management of Type 2 Diabetes Mellitus (5th Edition) PDFKai Xin100% (1)
- Smart Blood SugarDocument3 pagesSmart Blood SugarSimon Josh0% (1)
- Questions: Will Solar Work in My Location?Document4 pagesQuestions: Will Solar Work in My Location?Mario AlbertoNo ratings yet
- Diabetes CareDocument156 pagesDiabetes CaresahebjuNo ratings yet
- Led TV: Service ManualDocument75 pagesLed TV: Service ManualIulius-virgil DogaruNo ratings yet
- 7 Deadly Horrors DiabetesDocument20 pages7 Deadly Horrors Diabetestafer692002No ratings yet
- Diabetic Neuropathy PPT FinalDocument54 pagesDiabetic Neuropathy PPT FinalJenny Juniora AjocNo ratings yet
- A. Biology of Aging PDFDocument9 pagesA. Biology of Aging PDFlolipopckpNo ratings yet
- Fellowship in DiabetesDocument2 pagesFellowship in DiabetesBenjamin NelsonNo ratings yet
- Solar Power World January 2023 v2Document116 pagesSolar Power World January 2023 v2ELECTROSTATIC SPRAYERS GREECENo ratings yet
- Photo-Voltaic Solar Panel Monitoring With Safety Control Using NodeRED and ArduinoDocument10 pagesPhoto-Voltaic Solar Panel Monitoring With Safety Control Using NodeRED and ArduinoIJRASETPublicationsNo ratings yet
- READ THIS FIRST Diabetes Destroyer System 2Document111 pagesREAD THIS FIRST Diabetes Destroyer System 2Gabriel CaraveteanuNo ratings yet
- Case StudyDocument9 pagesCase StudyJulianne P. VillanuevaNo ratings yet
- Human Mineral 2Document24 pagesHuman Mineral 2Nitay SorkarNo ratings yet
- 3 - 2 Guidelines For Selction of Generator For SHPDocument48 pages3 - 2 Guidelines For Selction of Generator For SHPbacuoc.nguyen356No ratings yet
- ADA GUIDELINES FOR DIABETES DIAGNOSIS AND CARE-2015Document182 pagesADA GUIDELINES FOR DIABETES DIAGNOSIS AND CARE-2015MiaMDNo ratings yet
- Diabetes PPT FinalDocument86 pagesDiabetes PPT FinalMohammed IbraheemNo ratings yet
- KPI vs CSF - What managers need to knowDocument6 pagesKPI vs CSF - What managers need to knowuueNo ratings yet
- Medication Error Obat DM2012Document15 pagesMedication Error Obat DM2012Yusuf Ali WijayaNo ratings yet
- Komplikasi DM: Hemi SinoritaDocument26 pagesKomplikasi DM: Hemi SinoritaHuda Auto2000No ratings yet
- Hypoglycemia Protocol for Diabetics and Non-DiabeticsDocument43 pagesHypoglycemia Protocol for Diabetics and Non-DiabeticsHEBA NAJJAR100% (1)
- Treatment Based On: Pathophysiology of HyperglycemiaDocument38 pagesTreatment Based On: Pathophysiology of HyperglycemiaRoby KieranNo ratings yet
- Diabetes Acute Complications - Hypoglycemia and DKADocument37 pagesDiabetes Acute Complications - Hypoglycemia and DKAsilver mistNo ratings yet
- Hypoglycemia: DR Putra Hendra SPPD UnibaDocument17 pagesHypoglycemia: DR Putra Hendra SPPD UnibaThariq MuslimNo ratings yet
- Diabetes Autonomic NeuropathyDocument43 pagesDiabetes Autonomic NeuropathySana JamshedNo ratings yet
- Tafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahDocument22 pagesTafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahlidawatiNo ratings yet
- Tafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahDocument22 pagesTafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahlidawatiNo ratings yet
- Hypertension Linked to Stroke RiskDocument4 pagesHypertension Linked to Stroke RisklidawatiNo ratings yet
- Tafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahDocument22 pagesTafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahlidawatiNo ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument13 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistslidawatiNo ratings yet
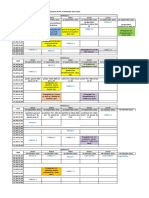
- Jadwal Blok 19 Edited 1Document2 pagesJadwal Blok 19 Edited 1lidawatiNo ratings yet
- C-Reactive Protein Levels of Sepsis Patients: A Comparison of Three Immunoassay MethodsDocument5 pagesC-Reactive Protein Levels of Sepsis Patients: A Comparison of Three Immunoassay MethodslidawatiNo ratings yet
- Tafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahDocument22 pagesTafsir Virus (Fauqa Ba'Ūdhah: Korelasi Covid-19 Dengan Ayat-Ayat AllahlidawatiNo ratings yet
- Hubungan Antara Gaya Belajar, Kemandirian Belajar, Dan Minat Belajar Dengan Hasil Belajar Biologi SiswaDocument8 pagesHubungan Antara Gaya Belajar, Kemandirian Belajar, Dan Minat Belajar Dengan Hasil Belajar Biologi SiswalidawatiNo ratings yet
- Trombositopenia Dan Trombosis Pada Pasien Rawat Inap Dengan COVID-19Document3 pagesTrombositopenia Dan Trombosis Pada Pasien Rawat Inap Dengan COVID-19lidawatiNo ratings yet
- 2019 (Covid-19) Dengan HipertensiDocument6 pages2019 (Covid-19) Dengan HipertensilidawatiNo ratings yet
- 1 SM PDFDocument4 pages1 SM PDFDaris UntoroNo ratings yet
- Hubungan Antara Lama Penggunaan Aspirin Dengan Nilai Agregasi Trombosit Pada Pasien Hipertensi Di Rsup Prof. Dr. R. D. Kandou ManadoDocument6 pagesHubungan Antara Lama Penggunaan Aspirin Dengan Nilai Agregasi Trombosit Pada Pasien Hipertensi Di Rsup Prof. Dr. R. D. Kandou ManadoDewina Dyani RosariNo ratings yet
- MEDIKA TADULAKO, Jurnal Ilmiah Kedokteran, Vol. 4 No. 1: Januari 2017Document10 pagesMEDIKA TADULAKO, Jurnal Ilmiah Kedokteran, Vol. 4 No. 1: Januari 2017lidawatiNo ratings yet
- Hypertension Linked to Stroke RiskDocument4 pagesHypertension Linked to Stroke RisklidawatiNo ratings yet
- Clinical Pathology and Medical Laboratory: Indonesian Journal ofDocument8 pagesClinical Pathology and Medical Laboratory: Indonesian Journal oflidawatiNo ratings yet
- Trombositopenia Dan Trombosis Pada Pasien Rawat Inap Dengan COVID-19Document3 pagesTrombositopenia Dan Trombosis Pada Pasien Rawat Inap Dengan COVID-19lidawatiNo ratings yet
- (Inggris) D-Dimer ElevationDocument19 pages(Inggris) D-Dimer ElevationlidawatiNo ratings yet
- Xu2020 Article MechanismOfThrombocytopeniaInCDocument4 pagesXu2020 Article MechanismOfThrombocytopeniaInClidawatiNo ratings yet
- (Inggris) D-Dimer DiomarkerDocument11 pages(Inggris) D-Dimer DiomarkerlidawatiNo ratings yet
- 1 s2.0 S0924857920301059 MainDocument13 pages1 s2.0 S0924857920301059 MainNini RinNo ratings yet
- D-dimer and platelet aggregation predict thrombotic risk in PADDocument8 pagesD-dimer and platelet aggregation predict thrombotic risk in PADlidawatiNo ratings yet
- E 6Document4 pagesE 6Gus RintoNo ratings yet
- Andreas C. Widjaja-01Document9 pagesAndreas C. Widjaja-01Legina AdityaNo ratings yet
- (Inggris) D-Dimer Antigen Konsep Dan Prospek Ke DepanDocument10 pages(Inggris) D-Dimer Antigen Konsep Dan Prospek Ke DepanlidawatiNo ratings yet
- IFCC Interim Guidelines On Biochemical/ Hematological Monitoring of COVID-19 PatientsDocument8 pagesIFCC Interim Guidelines On Biochemical/ Hematological Monitoring of COVID-19 PatientslidawatiNo ratings yet
- Sridhar 2016Document6 pagesSridhar 2016Desmiyati AdoeNo ratings yet
- (Inggris) Hubungan D-Dimer Dan Tekanan DarahDocument6 pages(Inggris) Hubungan D-Dimer Dan Tekanan DarahlidawatiNo ratings yet
- The D-Dimer Assay: Eric D. Johnson - John C. Schell - George M. RodgersDocument7 pagesThe D-Dimer Assay: Eric D. Johnson - John C. Schell - George M. RodgerslidawatiNo ratings yet
- Anti - HyperlipidemiaDocument18 pagesAnti - HyperlipidemiaZakarie Abdullahi Hussein100% (1)
- Report Public Dialogue Nanotech HealthcareDocument90 pagesReport Public Dialogue Nanotech HealthcareGemerlyn VallesNo ratings yet
- Pathophysiology: HIV Infection and AIDSDocument7 pagesPathophysiology: HIV Infection and AIDSmeylin SNo ratings yet
- ConjunctivitisDocument15 pagesConjunctivitisPuviyarasiNo ratings yet
- Jurnal Skripsi Anestesi 4Document8 pagesJurnal Skripsi Anestesi 4Tiara Anggun NurartoNo ratings yet
- Risk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriDocument14 pagesRisk factors of diabetic retinopathy and vision threatening diabetic retinopathy and vision threatening diabetic retinopaty based on diabetic retinopathy screening program in greater bandung, west java.astriSi PuputNo ratings yet
- A Century of Biological-Weapons Programs (1915-2015) : Reviewing The EvidenceDocument26 pagesA Century of Biological-Weapons Programs (1915-2015) : Reviewing The EvidenceCaio CesarNo ratings yet
- Clinical Course Discussion: Oregon Health & Science University, Portland, OregonDocument1 pageClinical Course Discussion: Oregon Health & Science University, Portland, OregonperjadanutNo ratings yet
- English: Quarter 4 - Module 1: Using Appropriate Grammatical Signals or Expressions To Each Pattern of Idea DevelopmentDocument33 pagesEnglish: Quarter 4 - Module 1: Using Appropriate Grammatical Signals or Expressions To Each Pattern of Idea DevelopmentShiela Tecson Gamayon40% (5)
- 1 PBDocument11 pages1 PBNaswa Alifia PutriNo ratings yet
- Tensiometro Jumper Jpd-Ha101Document48 pagesTensiometro Jumper Jpd-Ha101Ozkar EduardoNo ratings yet
- OMES-protocol OMDDocument9 pagesOMES-protocol OMDMaritzashuNo ratings yet
- 2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Document11 pages2017 (Laporan Pelayanan Rawat Jalan Dr. Ida Ayu Anom Margareni)Anggi RiyaniNo ratings yet
- Surgical SeiveDocument28 pagesSurgical SeiveSumeet PratapNo ratings yet
- Cardiac Marker Sem 5Document42 pagesCardiac Marker Sem 5novi pujiNo ratings yet
- Catálogo de Dispositivos PQS 2014 PDFDocument318 pagesCatálogo de Dispositivos PQS 2014 PDFGestion Biomedica Prosalco IPSNo ratings yet
- M.Sc Psychology Syllabus Provides Comprehensive CoverageDocument55 pagesM.Sc Psychology Syllabus Provides Comprehensive CoverageRashmi NNo ratings yet
- Pharma Laboratory ExperimentsDocument34 pagesPharma Laboratory Experimentsapi-3748748100% (4)
- Interpersonal Relationships Professional Communication Skills For Nurses 6Th Edition Arnold Test Bank Full Chapter PDFDocument29 pagesInterpersonal Relationships Professional Communication Skills For Nurses 6Th Edition Arnold Test Bank Full Chapter PDFhungden8pne100% (11)
- 2019b TK ManualDocument210 pages2019b TK ManualZvonko ŠuljakNo ratings yet
- OVPR FY20Q1 Proposal List PDFDocument45 pagesOVPR FY20Q1 Proposal List PDFtsuregiNo ratings yet
- Specialized Group Homes For Persons With Severe or Profound Mental Retardation and Serious Problem Behaviour in EnglandDocument18 pagesSpecialized Group Homes For Persons With Severe or Profound Mental Retardation and Serious Problem Behaviour in EnglandDeborah RiskinNo ratings yet
- Dentoalveolar Injuries and Wiring TechniquesDocument60 pagesDentoalveolar Injuries and Wiring Techniquessamys2ndemailNo ratings yet
- Special Edition E-80 4Document2 pagesSpecial Edition E-80 4Ankit AgarwalNo ratings yet
- Introduction to Radiotherapy: Blackboard AssignmentDocument2 pagesIntroduction to Radiotherapy: Blackboard AssignmentRafaNo ratings yet
- BOSH For SO1 Student Manual SampleDocument65 pagesBOSH For SO1 Student Manual SampleFroilan olazo100% (1)
- Physical Fitness Physical FitnessDocument18 pagesPhysical Fitness Physical FitnessCharmaine JanorasNo ratings yet
- Uts Advocacy PaperDocument11 pagesUts Advocacy PaperPlu AldiniNo ratings yet
- Garner 1511222Document17 pagesGarner 1511222Bj LongNo ratings yet
- Nejmoa1901814 AppendixDocument29 pagesNejmoa1901814 AppendixMuhammad AbdurrosyidNo ratings yet