You might also like
- Chronic Diabetic ComplicationsDocument46 pagesChronic Diabetic ComplicationsAri AsriniNo ratings yet
- Pemberian Insulin KMBDocument36 pagesPemberian Insulin KMBerdhian jatiNo ratings yet
- Komplikasi DM: Hemi SinoritaDocument26 pagesKomplikasi DM: Hemi SinoritaHuda Auto2000No ratings yet
- Medication Error Obat DM2012Document15 pagesMedication Error Obat DM2012Yusuf Ali WijayaNo ratings yet
- Lecture 5 Macrovascular ComplicationsDocument51 pagesLecture 5 Macrovascular ComplicationsCristinaGheorgheNo ratings yet
- Early Detection Kuliah DokterDocument61 pagesEarly Detection Kuliah Doktersuho exoNo ratings yet
- Insulin Dr. BowoDocument39 pagesInsulin Dr. BowoAri AsriniNo ratings yet
- Dr. R Bowo Pramono SPPD KemdDocument57 pagesDr. R Bowo Pramono SPPD Kemdanon_21114707No ratings yet
- Emergencies in Diabetes: Zulfachmi WahabDocument33 pagesEmergencies in Diabetes: Zulfachmi WahablidawatiNo ratings yet
- Management of T2DMDocument54 pagesManagement of T2DMdesyNo ratings yet
- Disglucemias Cronicas Clase 4Document101 pagesDisglucemias Cronicas Clase 4JOSÉ VIDAURE FRIAS VASQUEZNo ratings yet
- Hypoglycemia (DR Fatimah) PDFDocument23 pagesHypoglycemia (DR Fatimah) PDFriopratamasNo ratings yet
- Diabetic NephropathyDocument38 pagesDiabetic NephropathySwapnaNo ratings yet
- DM and NeurologyDocument43 pagesDM and NeurologySurat TanprawateNo ratings yet
- Diabetic Complications and Foot CareDocument54 pagesDiabetic Complications and Foot CareNaela AmranNo ratings yet
- Diabetes MelitusDocument65 pagesDiabetes MelitusDiaNo ratings yet
- Diabetes Mellitus and Hypertension Management in Clinical PracticesDocument37 pagesDiabetes Mellitus and Hypertension Management in Clinical PracticesSetyo PrabowoNo ratings yet
- Management of T Dmintheeraof Cardiovascular Outcome TrialDocument43 pagesManagement of T Dmintheeraof Cardiovascular Outcome TrialHeri Agung SetiawanNo ratings yet
- Trisula DM Titis Bang ErikDocument56 pagesTrisula DM Titis Bang ErikTitisNo ratings yet
- Askep DM Seminar KesdamDocument29 pagesAskep DM Seminar KesdamResty PermatasariNo ratings yet
- Managing Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoDocument45 pagesManaging Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoaprinaaaNo ratings yet
- Diabetes Melitus Jurnal Remed BiomedDocument6 pagesDiabetes Melitus Jurnal Remed BiomedNur Roza Aulia RNo ratings yet
- Pratley New Treatments For Type 2 DiabetesDocument85 pagesPratley New Treatments For Type 2 DiabetesMia DangaNo ratings yet
- Edit Virtual HR Managing Dyslipidemia in Special PopulationDocument38 pagesEdit Virtual HR Managing Dyslipidemia in Special PopulationIkmah FauzanNo ratings yet
- First Page PDFDocument1 pageFirst Page PDFAlejandro Guerrero LeónNo ratings yet
- Slide Curriculum Diabetes and CardiologyDocument52 pagesSlide Curriculum Diabetes and CardiologyNazmul Hasan MahmudNo ratings yet
- Deteksi Dini KomplikasiDocument70 pagesDeteksi Dini KomplikasiWiwik Puji LestariNo ratings yet
- Acute Chronic ComplicationDocument49 pagesAcute Chronic ComplicationMuhammad DaviqNo ratings yet
- Diabetes Mellitus and ComplicationsDocument25 pagesDiabetes Mellitus and ComplicationsPurnima ChoudhuryNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument6 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsRizki NovNo ratings yet
- Diabetes & Metabolic Syndrome: Clinical Research & ReviewsDocument6 pagesDiabetes & Metabolic Syndrome: Clinical Research & ReviewsRizki NovNo ratings yet
- Residual Risk: What Risk Remains After LDL-C Management and Intensive Therapy?Document7 pagesResidual Risk: What Risk Remains After LDL-C Management and Intensive Therapy?krispongNo ratings yet
- EMPA KIDNEY SGLT2 and Meta Analysis FINALDocument1 pageEMPA KIDNEY SGLT2 and Meta Analysis FINALThoraya AhmedNo ratings yet
- DR Supriyanto K-A New Insight Into Type 2 Diabetes Melitus Management For Reduicing Cvrdiovascular EventDocument56 pagesDR Supriyanto K-A New Insight Into Type 2 Diabetes Melitus Management For Reduicing Cvrdiovascular EventIgdrsui BoyolaliNo ratings yet
- Boala Cronica de Rinichi Adrian CovicDocument85 pagesBoala Cronica de Rinichi Adrian CovicLorenaNo ratings yet
- Diabetes Complication LectureDocument63 pagesDiabetes Complication LectureDoni MarthenNo ratings yet
- Amaryl Slide For Presentation 2015Document18 pagesAmaryl Slide For Presentation 2015suho exoNo ratings yet
- Dr. D.N. Prastowo, SP - PD: Bagian Penyakit Dalam Rs. Hana Charitas - Arga Makmur Bengkulu 2017Document45 pagesDr. D.N. Prastowo, SP - PD: Bagian Penyakit Dalam Rs. Hana Charitas - Arga Makmur Bengkulu 2017nanikNo ratings yet
- Austin AndrologyDocument4 pagesAustin AndrologyAustin Publishing GroupNo ratings yet
- Autonomic NeuropathyDocument20 pagesAutonomic NeuropathyRegina CaeciliaNo ratings yet
- Zanoglide Updated Master Slide Deck - Eva MOBILE VERSIONDocument124 pagesZanoglide Updated Master Slide Deck - Eva MOBILE VERSIONMaha BondokNo ratings yet
- Metabolic Syndrome Risk Factors and ComplicationsDocument46 pagesMetabolic Syndrome Risk Factors and ComplicationsAjeng RetnoNo ratings yet
- Penatalaksanaan Tindakan Kedokteran Gigi Pada Pasien Diabetes MellitusDocument35 pagesPenatalaksanaan Tindakan Kedokteran Gigi Pada Pasien Diabetes MellitusgeneNo ratings yet
- MEHU130 - U2 - T43 - Nefropatia DiabeticaDocument110 pagesMEHU130 - U2 - T43 - Nefropatia DiabeticaStefani AtlleNo ratings yet
- DKD and Sglt2iDocument61 pagesDKD and Sglt2iماكريلا المصريNo ratings yet
- Diabetes Autonomic NeuropathyDocument43 pagesDiabetes Autonomic NeuropathySana JamshedNo ratings yet
- Association of Blood Pressure Control and Metabolic Syndrome With Cardiovascular Risk in Elderly Japanese: JATOS StudyDocument7 pagesAssociation of Blood Pressure Control and Metabolic Syndrome With Cardiovascular Risk in Elderly Japanese: JATOS StudyRobertoNo ratings yet
- Intensive Glycemic Control in The ACCORD and ADVANCE Trials - EditorialDocument4 pagesIntensive Glycemic Control in The ACCORD and ADVANCE Trials - EditorialSheebaNo ratings yet
- Diabetes and Cardiovascular Disease: An SEO-Optimized GuideDocument36 pagesDiabetes and Cardiovascular Disease: An SEO-Optimized Guidegizi jatipadangNo ratings yet
- Diabetes Management With Basal InsulinDocument35 pagesDiabetes Management With Basal InsulinSultan MubashirNo ratings yet
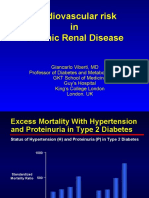
- Cardiovascular Risk in Chronic Renal DiseaseDocument36 pagesCardiovascular Risk in Chronic Renal DiseaseahkyenNo ratings yet
- Hypertension&Diabetes Mellitus: Fahmi Razi Darkuthni SMF Internal Medicine RSUD AmpanaDocument54 pagesHypertension&Diabetes Mellitus: Fahmi Razi Darkuthni SMF Internal Medicine RSUD AmpanaadminabNo ratings yet
- The Role of FDC Glimepiride-Metformin on T2DMDocument34 pagesThe Role of FDC Glimepiride-Metformin on T2DMRam PrototokonNo ratings yet
- What We Learn From The Newest Evidence ?Document70 pagesWhat We Learn From The Newest Evidence ?Intan HaddadNo ratings yet
- 2018 RTD Slide - The Place of Newer Generation SUDocument30 pages2018 RTD Slide - The Place of Newer Generation SUAlka AlkaNo ratings yet
- Cardiovascular Complication in HD 2019 DR RubinDocument49 pagesCardiovascular Complication in HD 2019 DR RubinASIS ADRINo ratings yet
- Management of Hyperglycemia and Diabetes in The HospitalDocument46 pagesManagement of Hyperglycemia and Diabetes in The HospitalvinoadhiyogaNo ratings yet
- DiabetesDocument39 pagesDiabetesRutuja VedpathakNo ratings yet
- VidagliptineDocument36 pagesVidagliptineAriyanaNo ratings yet
- The Metabolic SyndromeDocument37 pagesThe Metabolic SyndromeRoby Kieran100% (1)
- Screening For Micro and Macrovascular ComplicationDocument38 pagesScreening For Micro and Macrovascular ComplicationRoby KieranNo ratings yet
- Thyroid It IsDocument16 pagesThyroid It IsRoby KieranNo ratings yet
- Thyroid Gland and Disordwr KuliahDocument67 pagesThyroid Gland and Disordwr KuliahRoby KieranNo ratings yet
- Insulin Aspart Dan ProteminatedDocument4 pagesInsulin Aspart Dan ProteminatedSastra WijayaNo ratings yet
- Hyperthyroidsm and The HeartDocument23 pagesHyperthyroidsm and The HeartRoby KieranNo ratings yet
- DM Keto Dan HiperosmolarDocument33 pagesDM Keto Dan HiperosmolarRoby KieranNo ratings yet
- DM & KomplikasiDocument98 pagesDM & KomplikasiRoby KieranNo ratings yet
- Management of Perioperative On Diabetic Patients: DR Budi Enoch SPPDDocument18 pagesManagement of Perioperative On Diabetic Patients: DR Budi Enoch SPPDRoby KieranNo ratings yet
- DR Budi Enoch SPPDDocument31 pagesDR Budi Enoch SPPDRoby KieranNo ratings yet
- Levemir InternetDocument15 pagesLevemir InternetRoby KieranNo ratings yet
- Insulin: The Structure of Insulin. The Left Side Is A Space-Filling Model of The InsulinDocument21 pagesInsulin: The Structure of Insulin. The Left Side Is A Space-Filling Model of The Insulinsuho exoNo ratings yet
- Lipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeDocument65 pagesLipid Treatments in Cardiologic, Metabolic and Diabetics: From Guideline To Clinical PracticeRoby KieranNo ratings yet
- Myeloid Leukemia: DR Budi Enoch SPPDDocument36 pagesMyeloid Leukemia: DR Budi Enoch SPPDRoby KieranNo ratings yet
- Apa Yang Baru Dari DM Type 2Document31 pagesApa Yang Baru Dari DM Type 2Roby KieranNo ratings yet
- Anemi Aplastik Dan MielodisplasiaDocument34 pagesAnemi Aplastik Dan MielodisplasiaRoby KieranNo ratings yet
- Lymphoid Lekemia: DR Budi Enoch SPPDDocument32 pagesLymphoid Lekemia: DR Budi Enoch SPPDLia pramitaNo ratings yet
- Disorder of PlateletsDocument27 pagesDisorder of PlateletsRoby KieranNo ratings yet
- Kuliah DnaDocument47 pagesKuliah DnaRoby KieranNo ratings yet
- Microcytic Anemia, Iron Deff Dan ThalasemiaDocument34 pagesMicrocytic Anemia, Iron Deff Dan ThalasemiaRoby KieranNo ratings yet
- Kuliah Kelainan PeriartikulerDocument20 pagesKuliah Kelainan PeriartikulerRoby KieranNo ratings yet
- Kristal Artropati KuliahDocument36 pagesKristal Artropati KuliahRoby KieranNo ratings yet
- Pain KuliahDocument25 pagesPain KuliahRoby KieranNo ratings yet
- Shock Shock: DR Budi Enoch SPPDDocument31 pagesShock Shock: DR Budi Enoch SPPDRoby KieranNo ratings yet
- Evidence-Based Medicine,: Iwan Darmansjah Pusat Uji Klinik Obat, FkuiDocument40 pagesEvidence-Based Medicine,: Iwan Darmansjah Pusat Uji Klinik Obat, FkuiKastrat Lgm Fk UnismaNo ratings yet
- Coagulation DisordersDocument26 pagesCoagulation DisordersLia pramita0% (1)
- Cardinal Manifestations HeadacheDocument51 pagesCardinal Manifestations HeadacheRoby KieranNo ratings yet
- Cardinal Manifestations Back and Neck PainDocument33 pagesCardinal Manifestations Back and Neck PainRoby KieranNo ratings yet
- Social Responsibility and Managerial Ethics (Principles of Management)Document35 pagesSocial Responsibility and Managerial Ethics (Principles of Management)Reader94% (16)
- L&T Type 2 Co-Ordination Selection ChartsDocument48 pagesL&T Type 2 Co-Ordination Selection Chartsrdeepak99100% (7)
- Hotel Training ReportDocument14 pagesHotel Training ReportButchick Concepcion Malasa100% (1)
- Mechanical installation and maintenance guidelines for length counterDocument2 pagesMechanical installation and maintenance guidelines for length countervinod kumarNo ratings yet
- Lesson 1 G8Document11 pagesLesson 1 G8Malorie Dela CruzNo ratings yet
- Knowledge, Attitudes and Practices of Nursing Students on Dengue FeverDocument9 pagesKnowledge, Attitudes and Practices of Nursing Students on Dengue FeverElinNo ratings yet
- X1jet MX Manual PDFDocument97 pagesX1jet MX Manual PDFrithik srivastavaNo ratings yet
- Mechanics of Solids by Sadhu Singhpdf Ebook and Ma PDFDocument1 pageMechanics of Solids by Sadhu Singhpdf Ebook and Ma PDFNeeraj Janghu0% (2)
- CCNA Security Instructor Lab Manual v1 - p8Document1 pageCCNA Security Instructor Lab Manual v1 - p8MeMe AmroNo ratings yet
- Cbs BookDocument294 pagesCbs Bookadmiralninja100% (1)
- Procedure For Design and DevelopmentDocument8 pagesProcedure For Design and DevelopmentISO SRCASNo ratings yet
- NHW Upper Intermediate 4e Wordlist HungarianDocument34 pagesNHW Upper Intermediate 4e Wordlist HungarianpcdmisNo ratings yet
- Vehicle Speed Control Using RF CommunicationDocument20 pagesVehicle Speed Control Using RF CommunicationRaina John100% (2)
- NEM Report - IntroDocument11 pagesNEM Report - IntroRoshni PatelNo ratings yet
- Ritual and Religion Course at University of EdinburghDocument10 pagesRitual and Religion Course at University of EdinburghRenata DC MenezesNo ratings yet
- Estudio ArminioDocument13 pagesEstudio ArminioJavier LópezNo ratings yet
- Slings CatalogDocument152 pagesSlings CatalogtaNNertaroNo ratings yet
- CẤU TẠO TỪ VÀ TỪ LOẠIDocument15 pagesCẤU TẠO TỪ VÀ TỪ LOẠIccnsdNo ratings yet
- Salon Lesson Plan 233-1Document7 pagesSalon Lesson Plan 233-1api-264569989No ratings yet
- Chapter 12 1Document15 pagesChapter 12 1Brigitte ReyesNo ratings yet
- Teaching English Poetry at Secondary LevelDocument15 pagesTeaching English Poetry at Secondary LevelEngr Saud shahNo ratings yet
- Zero-Force Members: Hapter Tructural NalysisDocument3 pagesZero-Force Members: Hapter Tructural NalysistifaNo ratings yet
- 14-01 Lista de Laptops - DistribuidoresDocument29 pages14-01 Lista de Laptops - DistribuidoresInkil Orellana TorresNo ratings yet
- Argacel TCW_enDocument2 pagesArgacel TCW_enUtpalNo ratings yet
- EnrollNOLA Daily Seat Availability ReportDocument2 pagesEnrollNOLA Daily Seat Availability ReportAdvocateOnlineNo ratings yet
- Negros IslandDocument18 pagesNegros IslandGrace AmaganNo ratings yet
- Loveology: God. Love. Marriage. Sex. and The Never-Ending Story of Male and Female. by John Mark Comer, SamplerDocument32 pagesLoveology: God. Love. Marriage. Sex. and The Never-Ending Story of Male and Female. by John Mark Comer, SamplerZondervan40% (5)
- The Biology of Vascular Epiphytes Zotz 2016 PDFDocument292 pagesThe Biology of Vascular Epiphytes Zotz 2016 PDFEvaldo Pape100% (1)
- Lucky TextileDocument5 pagesLucky TextileSaim Bin RashidNo ratings yet
- Visual Communication, Summary WritingDocument8 pagesVisual Communication, Summary WritingAsumpta MainaNo ratings yet