You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- JUNE-29-2021-Reflection Paper - PGI MANIMTIMDocument2 pagesJUNE-29-2021-Reflection Paper - PGI MANIMTIMKim Adarem Joy ManimtimNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- PGI MANIMTIM - CPG - BF Screening Guidelines For PediatricsDocument42 pagesPGI MANIMTIM - CPG - BF Screening Guidelines For PediatricsKim Adarem Joy ManimtimNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- JULY-8-2021 - Reflection Paper - PGI MANIMTIMDocument2 pagesJULY-8-2021 - Reflection Paper - PGI MANIMTIMKim Adarem Joy ManimtimNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Significance of The StudyDocument25 pagesSignificance of The StudyKim Adarem Joy ManimtimNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- 6.01 - Diabetes Mellitus EDITED 4.22.2018Document30 pages6.01 - Diabetes Mellitus EDITED 4.22.2018Kim Adarem Joy ManimtimNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- CA - HarmDocument29 pagesCA - HarmKim Adarem Joy ManimtimNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- JUNE-23-2021 - PGI MANIMTIM-Reaction Paper On PFC MatrixDocument1 pageJUNE-23-2021 - PGI MANIMTIM-Reaction Paper On PFC MatrixKim Adarem Joy ManimtimNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Reflective Writing - Pgi ManimtimDocument22 pagesReflective Writing - Pgi ManimtimKim Adarem Joy ManimtimNo ratings yet
- Harm: Critical Appraisal: Perpetual Help Medical Center-Biñan Uph-Dr. Jose G. Tamayo Medical University Foundation, IncDocument34 pagesHarm: Critical Appraisal: Perpetual Help Medical Center-Biñan Uph-Dr. Jose G. Tamayo Medical University Foundation, IncKim Adarem Joy ManimtimNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- June 22 2021 Pgi Manimtim - Reaction PaperDocument3 pagesJune 22 2021 Pgi Manimtim - Reaction PaperKim Adarem Joy ManimtimNo ratings yet
- July-2-2021 Reflection Paper PGI MANIMTIMDocument2 pagesJuly-2-2021 Reflection Paper PGI MANIMTIMKim Adarem Joy ManimtimNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- PGI - MANIMTIM - Reaction Paper 10 - OHEPDocument1 pagePGI - MANIMTIM - Reaction Paper 10 - OHEPKim Adarem Joy ManimtimNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Pediatrics - Case Protocol - PGI MANIMTIM - DR TOMINEZDocument6 pagesPediatrics - Case Protocol - PGI MANIMTIM - DR TOMINEZKim Adarem Joy ManimtimNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- JULY-5-2021-PGI Manimtim-Reflection PaperDocument1 pageJULY-5-2021-PGI Manimtim-Reflection PaperKim Adarem Joy ManimtimNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- June-23-2021 - Pgi Manimtim - Reaction PaperDocument3 pagesJune-23-2021 - Pgi Manimtim - Reaction PaperKim Adarem Joy ManimtimNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Department of Pediatrics: Case ProtocolDocument11 pagesDepartment of Pediatrics: Case ProtocolKim Adarem Joy ManimtimNo ratings yet
- PGI - MANIMTIM - Reaction Paper 11 - RRL Dr. LapitanDocument1 pagePGI - MANIMTIM - Reaction Paper 11 - RRL Dr. LapitanKim Adarem Joy ManimtimNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- PGI - MANIMTIM - Reaction Paper 14 - Clerk's Action Plan and OHEPDocument1 pagePGI - MANIMTIM - Reaction Paper 14 - Clerk's Action Plan and OHEPKim Adarem Joy ManimtimNo ratings yet
- Soal Pat Inggris Kelas 7 - 2021Document9 pagesSoal Pat Inggris Kelas 7 - 2021Bella Septiani FaryanNo ratings yet
- Dasar-Dasar Radiologi MuskuloskeletalDocument26 pagesDasar-Dasar Radiologi MuskuloskeletalandreNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Study Literature Review: Hubungan Tingkat Depresi: Dengan Kualitas Tidur Pada Lanjut UsiaDocument10 pagesStudy Literature Review: Hubungan Tingkat Depresi: Dengan Kualitas Tidur Pada Lanjut UsiaEla NurlaelaNo ratings yet
- Relationship Between Narcissism and Aggression - A Meta-Analysis PDFDocument14 pagesRelationship Between Narcissism and Aggression - A Meta-Analysis PDFGiorgi PirtskhalaishviliNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Ayantu MekonnenDocument30 pagesAyantu Mekonnenmbgeletu1221No ratings yet
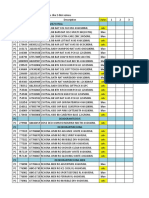
- MONITORING OOS MAR GMH ELIS 30 Maret 21)Document37 pagesMONITORING OOS MAR GMH ELIS 30 Maret 21)Andi ApriatnaNo ratings yet
- Loss, Grief and Grieving ProcessDocument28 pagesLoss, Grief and Grieving ProcessSuper .K. music lyricsNo ratings yet
- Disaster Management AgencyDocument72 pagesDisaster Management AgencyMichael PompeoNo ratings yet
- Manual of Microbiological Culture Media - 14Document1 pageManual of Microbiological Culture Media - 14Amin TaleghaniNo ratings yet
- The Next 8760 HOURS WORKSHEETDocument17 pagesThe Next 8760 HOURS WORKSHEETJejen AlimudinNo ratings yet
- Hiwot SeminarDocument77 pagesHiwot SeminarShemshedin AliyiNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Models of Emotional IntelligenceDocument2 pagesModels of Emotional Intelligencegsgopalsamy100% (4)
- Good Laboratory Practices (GLP) : What Is A Science Laboratory? General Hazard SymbolsDocument3 pagesGood Laboratory Practices (GLP) : What Is A Science Laboratory? General Hazard SymbolsTrese ShanelleNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Zoom Sales Script - Mortgage Protection 2Document1 pageZoom Sales Script - Mortgage Protection 2Chad EgglestonNo ratings yet
- Đề Thi Thử Lần 9.2019Document5 pagesĐề Thi Thử Lần 9.2019Hoa ĐỗNo ratings yet
- The Role of Ngos in Tribal Development in IndiaDocument13 pagesThe Role of Ngos in Tribal Development in IndiaSaurabh Shrivastava33% (3)
- Histamine, Serotonin and Ergot AlkaloidsDocument36 pagesHistamine, Serotonin and Ergot AlkaloidsSteph Taylor Reyes Radan100% (3)
- Msds Klorin LengkapDocument5 pagesMsds Klorin LengkapDarzya OllongNo ratings yet
- Experiment 1 PharmacoDocument3 pagesExperiment 1 PharmacoNur NabilahNo ratings yet
- Chemistry - Investigatory Food Adulteration by Prakhar Srivastava 12 A 2023-24Document18 pagesChemistry - Investigatory Food Adulteration by Prakhar Srivastava 12 A 2023-24PRAKHAR SRIVASTAVANo ratings yet
- Adverse Effects Pine Bark ExtractDocument4 pagesAdverse Effects Pine Bark ExtractAvelox FloxNo ratings yet
- Brief Description and Activities of Jibon Bima Corporation: OfficeDocument4 pagesBrief Description and Activities of Jibon Bima Corporation: OfficeMozaffor HossainNo ratings yet
- Theories of Personality 3 (Alfred Adler)Document42 pagesTheories of Personality 3 (Alfred Adler)Anne Jeanneth DiazNo ratings yet
- UB Gummies InfoDocument16 pagesUB Gummies InfoJagesh NDCNo ratings yet
- Betaland National Drugs ListDocument27 pagesBetaland National Drugs ListJumana AlharaziNo ratings yet
- Office/School/Clc Workweek Plan To The Personnel Division/Section/UnitDocument1 pageOffice/School/Clc Workweek Plan To The Personnel Division/Section/UnitRecy Beth EscopelNo ratings yet
- Ailing and Failing Us Dental ImplantsDocument12 pagesAiling and Failing Us Dental ImplantsCharlyBoeingNo ratings yet
- Raid Home Insect Killer EDocument8 pagesRaid Home Insect Killer EFillo IbrahimNo ratings yet
- 1 Seventh Day Adventist Theology of HealthDocument15 pages1 Seventh Day Adventist Theology of HealthYunus ElonNo ratings yet
- Medical 19.08.2023Document20 pagesMedical 19.08.2023Дмитрий ПирусNo ratings yet
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (5)