You might also like
- BN Defender BrochureDocument16 pagesBN Defender BrochurePieter BastiaansNo ratings yet
- 0070362408-Stick and Rudder by Wolfgang LangewiescheDocument6 pages0070362408-Stick and Rudder by Wolfgang LangewiescheAnonymous qTsFKXO0% (5)
- F 18 A - 2001Document489 pagesF 18 A - 2001Leo von Lüttichau100% (1)
- US Navy - Aircraft Mishap InvestigationDocument231 pagesUS Navy - Aircraft Mishap InvestigationmbgillisNo ratings yet
- Question Pool On Ncaa ExamsDocument40 pagesQuestion Pool On Ncaa Examsjouadi91% (11)
- Vintage Airplane - Dec 1993Document36 pagesVintage Airplane - Dec 1993Aviation/Space History Library100% (1)
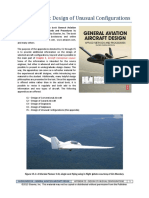
- App-C5-Design of Unusual Configurations PDFDocument22 pagesApp-C5-Design of Unusual Configurations PDFmiguelNo ratings yet
- 1.2 ICAO - EUR - UPRT (Airbus)Document64 pages1.2 ICAO - EUR - UPRT (Airbus)cdb8h5gjpg100% (1)
- s25 FullDocument6 pagess25 FullMayra Cervantes AvilezNo ratings yet
- Challenges For TelemedicineDocument4 pagesChallenges For Telemedicineluis11256No ratings yet
- WandayuyiuuyDocument5 pagesWandayuyiuuyluthfia awandaNo ratings yet
- TreadmillDocument3 pagesTreadmillInter FantasticNo ratings yet
- Air Medical Transport of Cardiac PatientsDocument9 pagesAir Medical Transport of Cardiac Patientswahyu pamungkasNo ratings yet
- Transfusion-Related Acute Lung Injury: A Literature Review: ReviewarticleDocument9 pagesTransfusion-Related Acute Lung Injury: A Literature Review: ReviewarticlekereklovagNo ratings yet
- Cardiovascular Risk Factors in Airline PilotsDocument4 pagesCardiovascular Risk Factors in Airline Pilotsluis11256No ratings yet
- Guidance Document: Medical Emergencies: Managing In-Flight Medical EventsDocument12 pagesGuidance Document: Medical Emergencies: Managing In-Flight Medical EventsAbinaya SNo ratings yet
- Evaluation and Management of The Physiologically.16Document11 pagesEvaluation and Management of The Physiologically.16alveteNo ratings yet
- Aviation and healthcarervw-JRSM 2015Document10 pagesAviation and healthcarervw-JRSM 2015mnovemberNo ratings yet
- BTS Clinical Statement On Air TravelDocument22 pagesBTS Clinical Statement On Air TravelAli SemajNo ratings yet
- Tsuchiya 2019Document11 pagesTsuchiya 2019Olivia Chandra DeviNo ratings yet
- Perioperative Lung ProtectionDocument6 pagesPerioperative Lung ProtectionWilliamRayCassidyNo ratings yet
- Jurnal Reading 3Document4 pagesJurnal Reading 3dezafarista_44587428No ratings yet
- Cateter Arteria Pulmonar 2011Document7 pagesCateter Arteria Pulmonar 2011jerodriguez82No ratings yet
- AIDA-MC - Medical Recommendations For Organizers of Competitons V1-1Document6 pagesAIDA-MC - Medical Recommendations For Organizers of Competitons V1-1MJ ChenNo ratings yet
- COVID-Statement June2020Document6 pagesCOVID-Statement June2020Tuan HaiNo ratings yet
- Risk Stratification in Lung ResectionDocument9 pagesRisk Stratification in Lung ResectionBarbara Daniela Gonzalez EspinozaNo ratings yet
- Aritm 2Document15 pagesAritm 2Sudar Pecinta ParawaliNo ratings yet
- Preemptive Mechanical Ventilation (VENTILACION M PREVENTIVA)Document26 pagesPreemptive Mechanical Ventilation (VENTILACION M PREVENTIVA)Jesus FrancoNo ratings yet
- Sickle Cell Anemia Trait in The Military Aircrew Population: A Report From The Military Aviation Safety Subcommittee of The Aviation Safety Committee, AsmaDocument4 pagesSickle Cell Anemia Trait in The Military Aircrew Population: A Report From The Military Aviation Safety Subcommittee of The Aviation Safety Committee, AsmaV HerryNo ratings yet
- Air Travel and PneumothorakDocument7 pagesAir Travel and PneumothorakRojullun TaufikNo ratings yet
- Algorithms For Difficult Airway Management: A ReviewDocument9 pagesAlgorithms For Difficult Airway Management: A ReviewParvathy R NairNo ratings yet
- Comparison of International Guideline Recommendations For Rhe Diagnosis Pulmonary EmbolismDocument14 pagesComparison of International Guideline Recommendations For Rhe Diagnosis Pulmonary EmbolismdrjavierbuenfilNo ratings yet
- PM1ch25 Aviation MedicineDocument13 pagesPM1ch25 Aviation MedicineLee SmithNo ratings yet
- A Review of Intraoperative Protective Ventilation: Review Article Open AccessDocument9 pagesA Review of Intraoperative Protective Ventilation: Review Article Open AccessLeiniker NavarroNo ratings yet
- Pulmonary Embolism:percutaneous Treatment 2022Document16 pagesPulmonary Embolism:percutaneous Treatment 2022Saikat MitraNo ratings yet
- Managing The Physiologically Difcult Airway in Critically Ill AdultsDocument7 pagesManaging The Physiologically Difcult Airway in Critically Ill AdultsVinicyus FariaNo ratings yet
- Fphys 12 712628Document21 pagesFphys 12 712628Tun Thit SaNo ratings yet
- Hipertensi Di PenerbanganDocument3 pagesHipertensi Di PenerbanganEri YunianNo ratings yet
- ESC Heart Failure - 2022 - Montero - Time Course Factors Related To and Prognostic Impact of Venoarterial ExtracorporealDocument10 pagesESC Heart Failure - 2022 - Montero - Time Course Factors Related To and Prognostic Impact of Venoarterial ExtracorporealMedicina Critica FcvNo ratings yet
- ASE Statement On Point-of-Care Ultrasound During The 2019 Novel Coronavirus PandemicDocument4 pagesASE Statement On Point-of-Care Ultrasound During The 2019 Novel Coronavirus PandemicTuan HaiNo ratings yet
- Critical Incidents of The Respiratory SystemDocument6 pagesCritical Incidents of The Respiratory SystemLia Whulan11No ratings yet
- JAA Manual of Civil Aviation Medicine Amdt 6Document329 pagesJAA Manual of Civil Aviation Medicine Amdt 6kamillimakNo ratings yet
- Acute Respiratory Distress Syndrome - Epidemiology, Pathophysiology, Pathology, and Etiology in Adults - UpToDateDocument27 pagesAcute Respiratory Distress Syndrome - Epidemiology, Pathophysiology, Pathology, and Etiology in Adults - UpToDateFrancisco MuñozNo ratings yet
- An Analysis of In-Flight Passenger Injuries and Medical ConditionsDocument30 pagesAn Analysis of In-Flight Passenger Injuries and Medical ConditionsvonmanoNo ratings yet
- Prevalenceof Fatigueina Groupof Airline PilotsDocument6 pagesPrevalenceof Fatigueina Groupof Airline PilotsNoel ShibuNo ratings yet
- Jurnal 2Document3 pagesJurnal 2zahroNo ratings yet
- 5 OriginalResearch AerotoxicSyndrom ENGDocument14 pages5 OriginalResearch AerotoxicSyndrom ENGvonmanoNo ratings yet
- Editorial: Acute Respiratory Failure: Pathophysiological Basis From A Multidisciplinary Clinical ApproachDocument2 pagesEditorial: Acute Respiratory Failure: Pathophysiological Basis From A Multidisciplinary Clinical ApproachAgil Rumboko SumitroNo ratings yet
- Journal Reading Marsya Y. Loppies (201283003)Document9 pagesJournal Reading Marsya Y. Loppies (201283003)joions gilberth oppiesNo ratings yet
- Spirometry: Predicting Risk and Outcome: Alessandro Brunelli, MD, Gaetano Rocco, MD, FRCSDocument8 pagesSpirometry: Predicting Risk and Outcome: Alessandro Brunelli, MD, Gaetano Rocco, MD, FRCSAfien MuktiNo ratings yet
- 2Q10 NewsletterDocument6 pages2Q10 NewslettercmarkdixonNo ratings yet
- Guidelines For Air Medical Dispatch PDFDocument23 pagesGuidelines For Air Medical Dispatch PDFDen SinyoNo ratings yet
- Recommendaton For The 2018 International Consensus Final PresentationDocument51 pagesRecommendaton For The 2018 International Consensus Final PresentationmaurinmarceoiaNo ratings yet
- ARDS PneumonectomieDocument13 pagesARDS PneumonectomieStéphanieNo ratings yet
- Practice Guidelines For Pulmonary Artery CatheterizationDocument27 pagesPractice Guidelines For Pulmonary Artery CatheterizationRadmila KaranNo ratings yet
- Air Pollution and Cardiovascular Disease: AHA Scientific StatementDocument17 pagesAir Pollution and Cardiovascular Disease: AHA Scientific StatementFeiky HerfandiNo ratings yet
- Hipercapnia PermisivaDocument18 pagesHipercapnia PermisivaARIADNA FABIOLA TRUJILLO RODRÍGUEZNo ratings yet
- Jurnal Pakai 6 (Patofisiologi, Diagnosis, Gejala)Document13 pagesJurnal Pakai 6 (Patofisiologi, Diagnosis, Gejala)Satrya DitaNo ratings yet
- Jurnal 1Document5 pagesJurnal 1RianNo ratings yet
- Percutaneous Treatment Options For Acute Pulmonary Embolism A Clinical ConsensusDocument16 pagesPercutaneous Treatment Options For Acute Pulmonary Embolism A Clinical ConsensusIlse Denise MarquezNo ratings yet
- Safe Surgery 2Document5 pagesSafe Surgery 2Masrun FatanahNo ratings yet
- Echocardiography in Pandemic Front Line Perspect - 2020 - Journal of The AmericDocument7 pagesEchocardiography in Pandemic Front Line Perspect - 2020 - Journal of The AmericANESTEGYONo ratings yet
- In-Flight Medical Emergencies A ReviewDocument11 pagesIn-Flight Medical Emergencies A ReviewSkechersUserNo ratings yet
- Esc Vs Aha Severe ASDocument17 pagesEsc Vs Aha Severe ASYogi AndrewNo ratings yet
- Acute Respiratory Distress Syndrome: Pathophysiology and Therapeutic OptionsDocument10 pagesAcute Respiratory Distress Syndrome: Pathophysiology and Therapeutic OptionsviviNo ratings yet
- COVID-19’s Consequences on the Cardiovascular System: Immediate, Intermediate, and Long-Term ComplicationsFrom EverandCOVID-19’s Consequences on the Cardiovascular System: Immediate, Intermediate, and Long-Term ComplicationsFabian Sanchis-GomarNo ratings yet
- JTM2021 5567063Document7 pagesJTM2021 5567063DEWI MEIRA ROSANo ratings yet
- Roma IV Desórdenes GastroduodenalesDocument13 pagesRoma IV Desórdenes GastroduodenalesJudith HMNo ratings yet
- Art I Colo Feeding IntoleranceDocument4 pagesArt I Colo Feeding IntoleranceDEWI MEIRA ROSANo ratings yet
- Ini PatologiDocument15 pagesIni PatologiDEWI MEIRA ROSANo ratings yet
- Student GovernmentDocument13 pagesStudent GovernmentDEWI MEIRA ROSANo ratings yet
- NIH Public Access: Gastrointestinal Stromal TumorsDocument21 pagesNIH Public Access: Gastrointestinal Stromal TumorsDEWI MEIRA ROSANo ratings yet
- Effect of Banana Isotonic Drink To Maintain Hydration Through Urine and Blood ElectrolytesDocument5 pagesEffect of Banana Isotonic Drink To Maintain Hydration Through Urine and Blood ElectrolytesDEWI MEIRA ROSANo ratings yet
- Blok 1.7: Friday, July 16, 2021 11:23 PMDocument2 pagesBlok 1.7: Friday, July 16, 2021 11:23 PMDEWI MEIRA ROSANo ratings yet
- Forgotten Hardware: How To Urinate in A Spacesuit: Historical PerspectivesDocument6 pagesForgotten Hardware: How To Urinate in A Spacesuit: Historical PerspectivesDEWI MEIRA ROSANo ratings yet
- British Cardiovascular Society Conference 2017: Maximizing Digital Data in HealthcareDocument6 pagesBritish Cardiovascular Society Conference 2017: Maximizing Digital Data in HealthcareDEWI MEIRA ROSANo ratings yet
- Review Article: Effect of Stress On Autonomic and Cardiovascular Systems in Military Population: A Systematic ReviewDocument9 pagesReview Article: Effect of Stress On Autonomic and Cardiovascular Systems in Military Population: A Systematic ReviewDEWI MEIRA ROSANo ratings yet
- Clean Sheet - Clean Start: Exclusive In-Flight ExperienceDocument1 pageClean Sheet - Clean Start: Exclusive In-Flight ExperienceBenknobi TVNo ratings yet
- Qatar ResumeDocument3 pagesQatar ResumeVema SaidattavamsikrishnaNo ratings yet
- Fdap-P13 - Moqa Program Sky AirlineDocument102 pagesFdap-P13 - Moqa Program Sky AirlineFannyng EdithNo ratings yet
- PDF N FCTM Mmo TF N Eu 20220817 fctm.364 366Document2 pagesPDF N FCTM Mmo TF N Eu 20220817 fctm.364 366Shadli Abu senNo ratings yet
- Aff Course: Student ManualDocument53 pagesAff Course: Student ManualAlexperabrxNo ratings yet
- Aircraft Act 1935 and 1937Document4 pagesAircraft Act 1935 and 1937shaik akhilNo ratings yet
- Percentage of Private Flights That Result in A CrashDocument16 pagesPercentage of Private Flights That Result in A Crashzuka jioshviliNo ratings yet
- Carta ADC SBMKDocument3 pagesCarta ADC SBMKThaynanNo ratings yet
- Airport Briefing: Bogota, Colombia Skbo/Bog Bogota, Colombia Skbo/BogDocument22 pagesAirport Briefing: Bogota, Colombia Skbo/Bog Bogota, Colombia Skbo/BogyhgfnyghyNo ratings yet
- 32-20-00-810-801-A01 - Grinding Noise From The NLG During Taxiing or Towing (Troubleshooting Procedure Weight On Wheels)Document3 pages32-20-00-810-801-A01 - Grinding Noise From The NLG During Taxiing or Towing (Troubleshooting Procedure Weight On Wheels)saiful hidayatNo ratings yet
- LANDING GEAR - The Flying EngineerDocument11 pagesLANDING GEAR - The Flying Engineerparbhoos1610No ratings yet
- The Basic How To' Guide: Helicopter's Private Pilot LicenseDocument3 pagesThe Basic How To' Guide: Helicopter's Private Pilot LicenseGrazy1982No ratings yet
- History of Propeller Cornelio CelesteDocument6 pagesHistory of Propeller Cornelio Celestecarmela celesteNo ratings yet
- Notam Manual enDocument140 pagesNotam Manual enEdwin SinginiNo ratings yet
- Nacdec 6 NewDocument18 pagesNacdec 6 NewKARTHIGA BNo ratings yet
- 21 Preventive Maintenance Aa PDFDocument20 pages21 Preventive Maintenance Aa PDFMaleficaruMTNo ratings yet
- Boarding Pass (SXR-BLR) PDFDocument2 pagesBoarding Pass (SXR-BLR) PDFAnamika DasNo ratings yet
- Cockpit : Ecam WarningDocument11 pagesCockpit : Ecam WarningAnh TuanNo ratings yet
- Air New Zealand DC 10 Flight 901 NOVEMBER 28,1979 (Erebus Disaster)Document38 pagesAir New Zealand DC 10 Flight 901 NOVEMBER 28,1979 (Erebus Disaster)noor_emelliaNo ratings yet
- Storming Ahead: How UK Has Kept Tempest On TrackDocument30 pagesStorming Ahead: How UK Has Kept Tempest On TrackGabriel FerrarioNo ratings yet
- NTSB Crash Preliminary Report of Buncombe County Plane CrashDocument4 pagesNTSB Crash Preliminary Report of Buncombe County Plane CrashDillon DavisNo ratings yet
- Carriage by AirDocument32 pagesCarriage by AirShashwat MalhotraNo ratings yet
- SI 129-01 Amdt. 0 - Validation and Surveillance of Foreign Air OperatorsDocument78 pagesSI 129-01 Amdt. 0 - Validation and Surveillance of Foreign Air Operatorsindra lessyNo ratings yet