You might also like
- Stages of Anaesthesia NotesDocument2 pagesStages of Anaesthesia NotesNomathamsanqa Khumalo100% (2)
- The Neurology of Consciousness: Cognitive Neuroscience and NeuropathologyFrom EverandThe Neurology of Consciousness: Cognitive Neuroscience and NeuropathologyRating: 5 out of 5 stars5/5 (5)
- Nursing Care Plan PDFDocument6 pagesNursing Care Plan PDFEngely MercaderNo ratings yet
- Science Form 1 - Chapter 2Document20 pagesScience Form 1 - Chapter 2Beevy GB85% (39)
- Tool Box Talk - Working in Hot WeatherDocument1 pageTool Box Talk - Working in Hot WeatherMobashir MahmoodNo ratings yet
- AnesthesiaDocument7 pagesAnesthesiajgcriste100% (9)
- Basic Concept of General AnesthesiaDocument97 pagesBasic Concept of General Anesthesiasanjivdas100% (1)
- General AnesthesiaDocument2 pagesGeneral AnesthesiadhaineyNo ratings yet
- MUCLecture 2023 101956636Document27 pagesMUCLecture 2023 101956636علي الاسديNo ratings yet
- StageDocument2 pagesStageRonel ResurricionNo ratings yet
- Thuy Functional DimensionDocument3 pagesThuy Functional DimensionTweetie PieNo ratings yet
- What Is HAART Therapy?: Rhonchi Are Continuous Low Pitched, Rattling Lung SoundsDocument9 pagesWhat Is HAART Therapy?: Rhonchi Are Continuous Low Pitched, Rattling Lung SoundskingpinNo ratings yet
- 2.3 General AnesthesiaDocument8 pages2.3 General AnesthesiaLA BriguelaNo ratings yet
- Anesthesia Stage 2: Excitement: SedationDocument4 pagesAnesthesia Stage 2: Excitement: Sedationim. EliasNo ratings yet
- The SURGICAL Experience: AnesthesiaDocument43 pagesThe SURGICAL Experience: AnesthesiaAngela CamilleNo ratings yet
- 1 Intraop Narration - FinalDocument65 pages1 Intraop Narration - Finalclaire yowsNo ratings yet
- Pharmacology of General Anesthetics: Heidi N Boyda, PH.DDocument33 pagesPharmacology of General Anesthetics: Heidi N Boyda, PH.DDian Laksamana HatiNo ratings yet
- Lesson 4: Seizure: The Underlying Cause Is AnDocument6 pagesLesson 4: Seizure: The Underlying Cause Is AnRocelyn CristobalNo ratings yet
- Surgical MS General Anesthesiology Information PDFDocument10 pagesSurgical MS General Anesthesiology Information PDFjoNo ratings yet
- Assis - Lec. Mohammed ResenDocument22 pagesAssis - Lec. Mohammed Resenعلي الاسديNo ratings yet
- Planes of AnaesthesiaDocument3 pagesPlanes of AnaesthesiaChrisNo ratings yet
- 5324 Planes of AnaesthesiaDocument3 pages5324 Planes of AnaesthesiaJulius RiazondaNo ratings yet
- Accidental Awareness During General Anaesthesia - A Narrative ReviewDocument12 pagesAccidental Awareness During General Anaesthesia - A Narrative ReviewBianca CaterinalisendraNo ratings yet
- Intraoperative NursingDocument41 pagesIntraoperative NursingBryan Mae H. Degorio100% (11)
- General Anaesthesia: Welcome ToDocument21 pagesGeneral Anaesthesia: Welcome Toفرسان الدعوةNo ratings yet
- Awareness in Anesthesia FinalisedDocument42 pagesAwareness in Anesthesia FinalisedLean CyNo ratings yet
- Types of Anesthesia: Presented byDocument74 pagesTypes of Anesthesia: Presented byPratima SharmaNo ratings yet
- Anesthesia PlainDocument39 pagesAnesthesia PlainMIKAELA DAVIDNo ratings yet
- Anesthesia: Anesthesia-Is A State of Narcosis (Severe CNC Depression Produce by Pharmacologic Agent)Document4 pagesAnesthesia: Anesthesia-Is A State of Narcosis (Severe CNC Depression Produce by Pharmacologic Agent)Donna Rezielle HayagNo ratings yet
- AsddddDocument7 pagesAsddddEphraim LuzaNo ratings yet
- Anesthetic MonitoringDocument11 pagesAnesthetic Monitoring102022No ratings yet
- Cns FormattedDocument59 pagesCns FormattedbrihaspathiacademyNo ratings yet
- Neurophysiology: Introduction ToDocument50 pagesNeurophysiology: Introduction ToSuardimanAchoNo ratings yet
- Multiple TraumaDocument5 pagesMultiple TraumaChristabel EdithNo ratings yet
- Ether (CH CH) O: 19 Century Physician Administering ChloroformDocument10 pagesEther (CH CH) O: 19 Century Physician Administering ChloroformbobNo ratings yet
- Introduction To AnaesthesiaDocument5 pagesIntroduction To AnaesthesiaAndrew CheongNo ratings yet
- Pulse Controlled Laser Acupuncture - The RAC / VASDocument12 pagesPulse Controlled Laser Acupuncture - The RAC / VASbob marleyNo ratings yet
- AnesthesiaDocument2 pagesAnesthesiakitten14No ratings yet
- General AnesthesiaDocument11 pagesGeneral AnesthesiaGERSON RYANTONo ratings yet
- W2 - MEDSURG Guidelines For Nursing Interventions On Coma PatientsDocument6 pagesW2 - MEDSURG Guidelines For Nursing Interventions On Coma PatientsKyla L. Madjad100% (1)
- Defining CharacteristicsDocument2 pagesDefining CharacteristicsAngel MayNo ratings yet
- BSBMED301: Assessment 1: What You Have To DoDocument8 pagesBSBMED301: Assessment 1: What You Have To DoPrayas AmatyaNo ratings yet
- Administer Medications As IndicatedDocument4 pagesAdminister Medications As IndicatedYza WagayenNo ratings yet
- Sedation and Analgesia in The Interventional Radiology DepartmentDocument10 pagesSedation and Analgesia in The Interventional Radiology DepartmentAhmed ElshewiNo ratings yet
- #4.inhalational Anesthesia: Stages of General Anesthesia HistoryDocument4 pages#4.inhalational Anesthesia: Stages of General Anesthesia HistoryCms CSUNo ratings yet
- Group 1 Nursing Diagnosis FinalDocument59 pagesGroup 1 Nursing Diagnosis FinalChristian Angelo LeonorNo ratings yet
- Phys 2S12 General Senses 1Document9 pagesPhys 2S12 General Senses 1adnilsallyNo ratings yet
- Nursing Care Plan # 1:: Assessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationDocument11 pagesNursing Care Plan # 1:: Assessment Diagnosis Scientific Basis Planning Nursing Interventions Rationale EvaluationGj PaguidianNo ratings yet
- Comprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference TipsDocument3 pagesComprehensive Life Support Tutorial Case 1: Question/Action Information Note/Reference Tipshyukkie minnieNo ratings yet
- Handouts Last Quarter HealthcareDocument15 pagesHandouts Last Quarter HealthcareClarisseNo ratings yet
- 290 Residual Neuromuscular Blockade PDFDocument8 pages290 Residual Neuromuscular Blockade PDFade winataNo ratings yet
- Assignment: Student Nurses' CommunityDocument3 pagesAssignment: Student Nurses' CommunityShafiq Ur RahmanNo ratings yet
- Types of AnesthesiaDocument3 pagesTypes of AnesthesiaAudrey LeonarNo ratings yet
- Approach To TremorDocument8 pagesApproach To TremorPrithvi RameshNo ratings yet
- Diagnostic Table 11Document9 pagesDiagnostic Table 11api-404185844No ratings yet
- ANAESTHESIADocument15 pagesANAESTHESIAshailendra.chauhan887No ratings yet
- History: AnestheticsDocument4 pagesHistory: AnestheticsMahnoor ArshadNo ratings yet
- General Anesthesia NEJM 2010 DR Emeri BrownDocument16 pagesGeneral Anesthesia NEJM 2010 DR Emeri BrownJuli OrtixNo ratings yet
- MODERATOR: DR Shreesh Mehrotra PRESENTER: DR Medha BhardwajDocument55 pagesMODERATOR: DR Shreesh Mehrotra PRESENTER: DR Medha BhardwajMilind Kothiyal100% (1)
- The Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaFrom EverandThe Psychology of Hysteria - A Selection of Classic Articles on the Analysis and Symptoms of HysteriaNo ratings yet
- Anes Airway-IntubationDocument12 pagesAnes Airway-IntubationSGD5Christine MendozaNo ratings yet
- Ob Basic-UltrasoundDocument115 pagesOb Basic-UltrasoundSGD5Christine MendozaNo ratings yet
- Ob - Abnormal Uterine BleedingDocument127 pagesOb - Abnormal Uterine BleedingSGD5Christine MendozaNo ratings yet
- Topic Outline: APR 14, 2021 Dr. Michelle BuelaDocument5 pagesTopic Outline: APR 14, 2021 Dr. Michelle BuelaSGD5Christine MendozaNo ratings yet
- ANS Skeletal Muscle AssignmentDocument4 pagesANS Skeletal Muscle AssignmentAkinsanya Oyinkansola ChristineNo ratings yet
- Muscular System Histology and Physiology 9.1-9.3 (Seeley's 12th Edition)Document2 pagesMuscular System Histology and Physiology 9.1-9.3 (Seeley's 12th Edition)Bullosos, Siera Jade Anne R.No ratings yet
- Newborn Care LectureDocument65 pagesNewborn Care LectureNichole daFonsecaNo ratings yet
- Breathing Exercises ReportDocument9 pagesBreathing Exercises ReportErica SironNo ratings yet
- Sim Muscle TutorialDocument20 pagesSim Muscle TutorialKiran KumarNo ratings yet
- Asthma: Dr. Raed ShudifatDocument36 pagesAsthma: Dr. Raed ShudifatRema WaleedNo ratings yet
- PHARMA 06. Introduction To Autonomic PharmacologyDocument6 pagesPHARMA 06. Introduction To Autonomic PharmacologyCindy Mae MacamayNo ratings yet
- Piezos Thrive Under PressureDocument13 pagesPiezos Thrive Under PressureВладимир ДружининNo ratings yet
- Cells and Tissues: Gross CellularDocument10 pagesCells and Tissues: Gross Cellularsasa sasadzeNo ratings yet
- Cell Types: Plant and Animal TissuesDocument40 pagesCell Types: Plant and Animal TissuesMARY ANN PANGANNo ratings yet
- Konsep Nyeri Dan Manajemen NyeriDocument36 pagesKonsep Nyeri Dan Manajemen NyeriFira AlumanNo ratings yet
- How Pranayam WorksDocument1 pageHow Pranayam WorkssachinisloorNo ratings yet
- Project 1 Final DraftDocument8 pagesProject 1 Final Draftapi-741172597No ratings yet
- Fundamentals of Human Energy TransferDocument46 pagesFundamentals of Human Energy TransferVidhisha Pai100% (1)
- Jurnal - Komponen DarahDocument6 pagesJurnal - Komponen Darahvivi maykasariNo ratings yet
- The Sleeping Habits of Selected Grade 10 Students in Dalandanan National High School and Its Effect in Their Academic PerformanceDocument18 pagesThe Sleeping Habits of Selected Grade 10 Students in Dalandanan National High School and Its Effect in Their Academic PerformanceJeffrey Dela CruzNo ratings yet
- Pe Lecture NotesDocument7 pagesPe Lecture NotesAnonymous LJrX4dzNo ratings yet
- Altered Body TemperatureDocument10 pagesAltered Body TemperatureMelvin VrNo ratings yet
- (Lib-Ebooks Com) 240820202341 PDFDocument193 pages(Lib-Ebooks Com) 240820202341 PDFDr. Hisham Abdul MajeedNo ratings yet
- Clinmed 21 3 E275Document8 pagesClinmed 21 3 E275Carlos CoronaNo ratings yet
- Photosynthesis: A2 Biology (9700) 2022-2023Document31 pagesPhotosynthesis: A2 Biology (9700) 2022-2023Youssef AhmedNo ratings yet
- GLUCONEOGENESISDocument18 pagesGLUCONEOGENESISKundaNo ratings yet
- Peripheral Vascular Assessment - StudentDocument3 pagesPeripheral Vascular Assessment - StudentSherinne Jane CariazoNo ratings yet
- Chemistry of HormonesDocument10 pagesChemistry of HormonesRuqayya ImranNo ratings yet
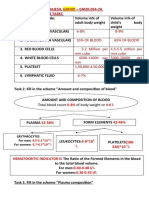
- Name - Soni Ritika Rajesh, Group - GM20-054-2A Physiology Week 03 TasksDocument10 pagesName - Soni Ritika Rajesh, Group - GM20-054-2A Physiology Week 03 TasksRitika SoniNo ratings yet
- Stroke Script - ABACDocument6 pagesStroke Script - ABACLee AndrewNo ratings yet
- Laboratory Exercise 34 BloodDocument2 pagesLaboratory Exercise 34 BloodNikki RodriguezNo ratings yet
- Mark Scheme Question OneDocument6 pagesMark Scheme Question OnesulthanramizNo ratings yet