You might also like
- Deathwatch Game Master's Kit (Screen) PDFDocument2 pagesDeathwatch Game Master's Kit (Screen) PDFSergio Morales100% (1)
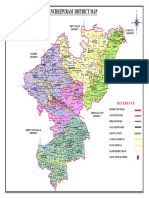
- Kancheepuram District Map 2021021047Document1 pageKancheepuram District Map 2021021047Vaishnavi JayakumarNo ratings yet
- Panduan Isoman CovidDocument13 pagesPanduan Isoman CovidUjang AbdillahNo ratings yet
- MoHP Protocol For COVID19 November 2020Document28 pagesMoHP Protocol For COVID19 November 2020medya dostorNo ratings yet
- Tim Redmer AccountingDocument204 pagesTim Redmer AccountingDax100% (5)
- Krsnadasa Kaviraja-Govinda LilamrtaDocument89 pagesKrsnadasa Kaviraja-Govinda LilamrtadouramaterNo ratings yet
- Comprehensive Guidelines For Management of COVID-19 In: ChildrenDocument11 pagesComprehensive Guidelines For Management of COVID-19 In: ChildrenAyushi GuptaNo ratings yet
- Comprehensive Guidelines For Management of COVID-19 In: ChildrenDocument13 pagesComprehensive Guidelines For Management of COVID-19 In: ChildrenVaibhav Tiwari100% (1)
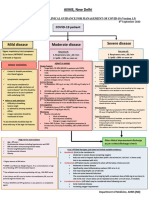
- Directorate General of Health Services, Mohfw, Goi Comprehensive Guidelines For Management of Covid-19 Patients Asymptomatic Mild Moderate SevereDocument2 pagesDirectorate General of Health Services, Mohfw, Goi Comprehensive Guidelines For Management of Covid-19 Patients Asymptomatic Mild Moderate SevereSpecial OPD SVMCHRCNo ratings yet
- Barnet Primary Care Guide During Covid-19: Contents PageDocument32 pagesBarnet Primary Care Guide During Covid-19: Contents PageGreta Tanushi KukaNo ratings yet
- Comprehensive Guidelines For Management of COVID-19 In: Children AdolescentsDocument12 pagesComprehensive Guidelines For Management of COVID-19 In: Children AdolescentsDheeraj kambleNo ratings yet
- Guidelines For Management of COVID-19 in Children (Below 18 Years)Document10 pagesGuidelines For Management of COVID-19 in Children (Below 18 Years)Juhi NeogiNo ratings yet
- Home Care For CovidDocument18 pagesHome Care For CovidiSmayli (smyle-smayl)No ratings yet
- NIV ProformaDocument10 pagesNIV ProformaWael N Sh GadallaNo ratings yet
- Asthma Guidelines 2016Document21 pagesAsthma Guidelines 2016Varun ArunagiriNo ratings yet
- Treatment Guidance For COVID-19 - 6 December 2020Document1 pageTreatment Guidance For COVID-19 - 6 December 2020meiraimNo ratings yet
- Covid 19 Infection Prevention and Control CasicsDocument46 pagesCovid 19 Infection Prevention and Control CasicsCainta Mpl Jail TanNo ratings yet
- Bronchiolitis - The Quick Guide: Assessment of Severity of DiseaseDocument2 pagesBronchiolitis - The Quick Guide: Assessment of Severity of Diseasebaiq dessyNo ratings yet
- AIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaDocument1 pageAIIMS/ ICMR-COVID-19 National Task Force/ Joint Monitoring Group (Dte - GHS) Ministry of Health & Family Welfare, Government of IndiaSomnath Das GuptaNo ratings yet
- Long Covid An Update Full Presentation Final VersionDocument99 pagesLong Covid An Update Full Presentation Final VersionJjuuko EdrinNo ratings yet
- Long Covid An Update Full Presentation Final VersionDocument99 pagesLong Covid An Update Full Presentation Final VersionyudistiraanwarNo ratings yet
- Updated Covid-19 Protocols: Based On The Latest Guidelines From Doh, Psmid, CDC and WhoDocument62 pagesUpdated Covid-19 Protocols: Based On The Latest Guidelines From Doh, Psmid, CDC and WhoN CNo ratings yet
- COVID19Document79 pagesCOVID19Mohamad El SharNo ratings yet
- Edited Cme Covid 19 Clinical ManagementDocument35 pagesEdited Cme Covid 19 Clinical ManagementikhlaslivingNo ratings yet
- Respiratory Distress and CPAP: Maternity and Neonatal Clinical GuidelineDocument32 pagesRespiratory Distress and CPAP: Maternity and Neonatal Clinical GuidelinePediatri UnsratNo ratings yet
- Summary of Joint Guideline On The Management of Long COVID: Steve ChaplinDocument3 pagesSummary of Joint Guideline On The Management of Long COVID: Steve ChaplinRahmanu ReztaputraNo ratings yet
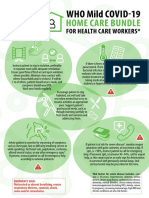
- WHO COVID-19-Home-Care-BundleDocument2 pagesWHO COVID-19-Home-Care-BundleOCSAF - P2LT PUNSALAN MCNo ratings yet
- Self Care Guide Pantai 1Document33 pagesSelf Care Guide Pantai 1puterishaliza272No ratings yet
- Kpj's Covid-19 BookletDocument62 pagesKpj's Covid-19 BookletKan Mi YiewNo ratings yet
- Dialysis Inovative Facility Policies and ProceduresDocument3 pagesDialysis Inovative Facility Policies and ProceduresFrancis Marven Lee LocsinNo ratings yet
- Pneumonia AdultDocument1 pagePneumonia AdultRoi LevinzonNo ratings yet
- Mental Health and Psychosocial Resilience in The Time of PandemicDocument64 pagesMental Health and Psychosocial Resilience in The Time of Pandemicreginald_adia_1No ratings yet
- Session 4-Management of Paediatric COVID19Document24 pagesSession 4-Management of Paediatric COVID19Uncertain NeuronNo ratings yet
- COVID19 Management Algorithm 22042021 v1Document1 pageCOVID19 Management Algorithm 22042021 v1shivani shindeNo ratings yet
- COVID 19 MG Protocol FinalDocument13 pagesCOVID 19 MG Protocol FinalajiNo ratings yet
- 1.nurse Preparedness Training Against 3rd Wave of CovidDocument52 pages1.nurse Preparedness Training Against 3rd Wave of CovidyeshumasihNo ratings yet
- TIH COVID Guideline AdultDocument24 pagesTIH COVID Guideline AdultMr MWSKNo ratings yet
- Edited COVID19 HANDOUT Requina SindiongDocument5 pagesEdited COVID19 HANDOUT Requina SindiongJannen CasasNo ratings yet
- Bu BudiDocument32 pagesBu Budinoi javuNo ratings yet
- Covid-19 Management: FAQs by HCWsDocument31 pagesCovid-19 Management: FAQs by HCWsKabirNo ratings yet
- COVID Guideline v2 8 5 21Document14 pagesCOVID Guideline v2 8 5 21Abdul JalilNo ratings yet
- Child With Fever in ER Non Covid 19Document6 pagesChild With Fever in ER Non Covid 19Suwandi AlghozyNo ratings yet
- Indirect Inguinal HerniaDocument32 pagesIndirect Inguinal HerniaJohn Michael CabitNo ratings yet
- What We Should Know About COVID-19!Document25 pagesWhat We Should Know About COVID-19!Frank ThomasNo ratings yet
- Sample Case Studies of COVID-19 in PregnancyDocument29 pagesSample Case Studies of COVID-19 in PregnancyAbdibaset Mohamed AdenNo ratings yet
- COVID Guideline v2 6 5 21Document14 pagesCOVID Guideline v2 6 5 21Kamrul AhsanNo ratings yet
- PHC ILI Guidlines COVID-19 FinalDocument4 pagesPHC ILI Guidlines COVID-19 Finalyalmas ugloNo ratings yet
- CCRH - Revised Guidelines For Homeopathy Practitioners For Home Isolated COVID 19 Patient-FDocument4 pagesCCRH - Revised Guidelines For Homeopathy Practitioners For Home Isolated COVID 19 Patient-FTisil KodithottamNo ratings yet
- Cap CPG 2020Document135 pagesCap CPG 2020Batch 2024 Internal MedicineNo ratings yet
- Clinical Management Guidelines For COVID-19 Infections - 1201Document8 pagesClinical Management Guidelines For COVID-19 Infections - 1201Ehtisham KhattakNo ratings yet
- Kerala State Covid 19 Treatment Guidelines V4 August 5Document124 pagesKerala State Covid 19 Treatment Guidelines V4 August 5Akshay RamakrishnanNo ratings yet
- AIIMS COVID Doc 1.6.1-1Document1 pageAIIMS COVID Doc 1.6.1-1mbhangaleNo ratings yet
- AIIMS COVID Algorithm 1.5-1 PDFDocument1 pageAIIMS COVID Algorithm 1.5-1 PDFAnutosh BhaskarNo ratings yet
- COVID 19 TRAINING FOR HEALTHCARE WORKERS Terapeutics Stanford UniversityDocument9 pagesCOVID 19 TRAINING FOR HEALTHCARE WORKERS Terapeutics Stanford University[JC]No ratings yet
- Covid in PregnancyDocument30 pagesCovid in Pregnancyvidhi chaudharyNo ratings yet
- Covid-19 For MRCP ExamsDocument6 pagesCovid-19 For MRCP ExamsZara VaraNo ratings yet
- FIP COVID-19 Webinar Slides Key Considerations FinalDocument49 pagesFIP COVID-19 Webinar Slides Key Considerations FinalCahyuni Saputri YusufNo ratings yet
- Guideline Managing Critically IllDocument8 pagesGuideline Managing Critically Illmisfatrianoor10No ratings yet
- Guidelines For DoctorsDocument4 pagesGuidelines For DoctorsNazar KaNo ratings yet
- Covid Antiviral Medications How To Prescribe Mar 10 2022Document38 pagesCovid Antiviral Medications How To Prescribe Mar 10 2022ABDULLAH SDNo ratings yet
- Journal Club Critique - HCQ in COVID-19Document4 pagesJournal Club Critique - HCQ in COVID-19Ivan ToscaniNo ratings yet
- HFNC 160915045634 PDFDocument25 pagesHFNC 160915045634 PDFTài NguyễnNo ratings yet
- Long Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingFrom EverandLong Covid - The Long Covid Book for Clinicians and Sufferers - Away from Despair and Towards UnderstandingNo ratings yet
- CDMP 2023Document804 pagesCDMP 2023Vaishnavi JayakumarNo ratings yet
- Adsi 2020 NCRB Full Report Accidental Deaths and Suicides Report IndiaDocument298 pagesAdsi 2020 NCRB Full Report Accidental Deaths and Suicides Report IndiaVaishnavi JayakumarNo ratings yet
- Urban Floods Chennai Report NGT Sep2021Document55 pagesUrban Floods Chennai Report NGT Sep2021Vaishnavi Jayakumar100% (1)
- Adsi 2016 Full Report 2016 Accidental Deaths & Suicides in India (ADSI) - 2016Document310 pagesAdsi 2016 Full Report 2016 Accidental Deaths & Suicides in India (ADSI) - 2016Vaishnavi JayakumarNo ratings yet
- Chennai Disaster Management Plan With Zonal Ready ReckonersDocument725 pagesChennai Disaster Management Plan With Zonal Ready ReckonersVaishnavi JayakumarNo ratings yet
- Chennai GCC Disaster Management Plan 2017Document117 pagesChennai GCC Disaster Management Plan 2017Vaishnavi JayakumarNo ratings yet
- Adsi 2019 Full Report Updated Accidental Deaths & Suicides in India - 2019Document310 pagesAdsi 2019 Full Report Updated Accidental Deaths & Suicides in India - 2019Vaishnavi JayakumarNo ratings yet
- Civil Supplies Disaster MGMT Plan 2017 18Document12 pagesCivil Supplies Disaster MGMT Plan 2017 18Vaishnavi JayakumarNo ratings yet
- Tiruvallur District Disaster Management Plan 2021070956Document297 pagesTiruvallur District Disaster Management Plan 2021070956Vaishnavi JayakumarNo ratings yet
- Tamil Nadu State Disaster Management Perspective Plan - SDMP-29-08Document202 pagesTamil Nadu State Disaster Management Perspective Plan - SDMP-29-08Vaishnavi Jayakumar100% (1)
- Chenglepet Disaster Management Plan - 2021100994Document470 pagesChenglepet Disaster Management Plan - 2021100994Vaishnavi JayakumarNo ratings yet
- Tamil Nadu Sustainable Urban Development Project. Storm Water Drains For The Selected Areas of Corporation of ChennaiDocument2 pagesTamil Nadu Sustainable Urban Development Project. Storm Water Drains For The Selected Areas of Corporation of ChennaiVaishnavi JayakumarNo ratings yet
- Current 20210513 Tamil Nadu Covid 19 Treatment Protocol - HFW - e - 239 - 2021Document6 pagesCurrent 20210513 Tamil Nadu Covid 19 Treatment Protocol - HFW - e - 239 - 2021Vaishnavi JayakumarNo ratings yet
- TNEB Disaster Management Plan August 2017Document105 pagesTNEB Disaster Management Plan August 2017Vaishnavi JayakumarNo ratings yet
- TN G.O. 386 Extending Lockdown With Further RestrictionsDocument5 pagesTN G.O. 386 Extending Lockdown With Further RestrictionsVaishnavi JayakumarNo ratings yet
- Tocilizumab Order 30 April 21Document3 pagesTocilizumab Order 30 April 21Vaishnavi JayakumarNo ratings yet
- Disaster Management Presentation by Sudesh MukhopadyayDocument66 pagesDisaster Management Presentation by Sudesh MukhopadyayVaishnavi JayakumarNo ratings yet
- CAG Union Performance Civil Mid Day Meal Report 2015Document156 pagesCAG Union Performance Civil Mid Day Meal Report 2015Vaishnavi JayakumarNo ratings yet
- Mid Day Meal Rules: Notifications Till June 2019Document25 pagesMid Day Meal Rules: Notifications Till June 2019Vaishnavi JayakumarNo ratings yet
- K. Muniasamythevar Vs Dy. Superintendent of Police and ... On 29 March, 2006Document7 pagesK. Muniasamythevar Vs Dy. Superintendent of Police and ... On 29 March, 2006Vaishnavi JayakumarNo ratings yet
- Jallikattu 2009 Death Statistics ReportDocument2 pagesJallikattu 2009 Death Statistics ReportVaishnavi JayakumarNo ratings yet
- Tamil Nadu Prevention of Cruelty To Animals (Conduct of Jallikattu) Rules, 2017Document5 pagesTamil Nadu Prevention of Cruelty To Animals (Conduct of Jallikattu) Rules, 2017Vaishnavi Jayakumar100% (1)
- Recovering From Psychosocial Traumas: The Place of Dargahs in MaharashtraDocument23 pagesRecovering From Psychosocial Traumas: The Place of Dargahs in MaharashtraVaishnavi JayakumarNo ratings yet
- NDMA NIMHANS Guidelines On Psycho-Social Support and Mental Health Services (PSSMHS) in DisastersDocument106 pagesNDMA NIMHANS Guidelines On Psycho-Social Support and Mental Health Services (PSSMHS) in DisastersVaishnavi JayakumarNo ratings yet
- Psychosocial Care in Disasters ToT NIDMDocument162 pagesPsychosocial Care in Disasters ToT NIDMVaishnavi JayakumarNo ratings yet
- Kerala DIDRR Peer Review FormatDocument141 pagesKerala DIDRR Peer Review FormatVaishnavi JayakumarNo ratings yet
- A Vision-Based Method For The Detection of Missing Rail FastenersDocument6 pagesA Vision-Based Method For The Detection of Missing Rail FastenersShivaprasad.b.kNo ratings yet
- Boeing Case SolutionDocument6 pagesBoeing Case SolutionNeha SinghNo ratings yet
- MCQ CPWA Code Chapter-10Document14 pagesMCQ CPWA Code Chapter-10Biswajit JenaNo ratings yet
- Olga Ujhelly, PHD During My Science in Biotalentum, Gödöllő, Hungary 25-29.1Document12 pagesOlga Ujhelly, PHD During My Science in Biotalentum, Gödöllő, Hungary 25-29.1My Science Programme for Young JournalistsNo ratings yet
- PDFtothepointrbimDocument5 pagesPDFtothepointrbimmaria83No ratings yet
- Sre ProjectDocument13 pagesSre ProjectSadatur RahmanNo ratings yet
- MA Tata Institute of Social Sciences Mumbai: Sardar SarovarDocument5 pagesMA Tata Institute of Social Sciences Mumbai: Sardar SarovarGauravNo ratings yet
- Cost Volume Profit Analysis: Meaning Purpose Assumptions TechniquesDocument36 pagesCost Volume Profit Analysis: Meaning Purpose Assumptions TechniquesreaderNo ratings yet
- CMS-016 Scope of Work Guide v1 0Document12 pagesCMS-016 Scope of Work Guide v1 0ChrisNo ratings yet
- RFI Checklist Site BELOPARANG (Infill - SSul37)Document5 pagesRFI Checklist Site BELOPARANG (Infill - SSul37)Adhyatma RaufNo ratings yet
- Upsetting of Bimetallic Components in Closed DieDocument6 pagesUpsetting of Bimetallic Components in Closed DieSatyajeet BeheraNo ratings yet
- TRN (Submersible Aerator)Document3 pagesTRN (Submersible Aerator)buattugasmetlitNo ratings yet
- Blind StitchDocument27 pagesBlind StitchSiddharth JhaNo ratings yet
- Groom Packing ListDocument1 pageGroom Packing ListmyselfanjalisainiNo ratings yet
- Instruction Manual Juki LK 1903A PDFDocument37 pagesInstruction Manual Juki LK 1903A PDFMaskusyaniNo ratings yet
- Cultivation of Algae - Photobioreactor - Oilgae - Oil From AlgaeDocument10 pagesCultivation of Algae - Photobioreactor - Oilgae - Oil From Algaeswetha chandrasekaranNo ratings yet
- Lab 4Document7 pagesLab 4HEMANILASHINII A P R THARMALINGAMNo ratings yet
- PPA StructuringDocument34 pagesPPA StructuringRaj Tha100% (1)
- TX 2017 PDFDocument265 pagesTX 2017 PDFSigit CahyoNo ratings yet
- FE Credit System SyllabusDocument36 pagesFE Credit System SyllabusHarshvardhanUpadhyayNo ratings yet
- Group I Study Material, Telugu Medium & English Medium, Sakshieducation2Document1 pageGroup I Study Material, Telugu Medium & English Medium, Sakshieducation2Ravi Kumar MogilsettiNo ratings yet
- Overview of Geophysical MethodsDocument41 pagesOverview of Geophysical MethodsVaqas Ali KhanNo ratings yet
- The Cambridge History of Science, Volume 6Document660 pagesThe Cambridge History of Science, Volume 6Jesus DamascenoNo ratings yet
- White Genoa ID ResearchDocument7 pagesWhite Genoa ID ResearchКлиментий РанчуковNo ratings yet
- Matheiu Function DocumentationDocument23 pagesMatheiu Function DocumentationSabitabrata BanerjeeNo ratings yet
- Bespoke Benchmarking PDFDocument2 pagesBespoke Benchmarking PDFDurga PrasadNo ratings yet
- Instant Download Human Development A Life Span View 7th Edition Kail Test Bank PDF Full ChapterDocument32 pagesInstant Download Human Development A Life Span View 7th Edition Kail Test Bank PDF Full Chapterhaodienb6qj100% (8)