You might also like
- Motoric Central Nervous System: Dr. Ridwan Harrianto MHSC (Om) SP - Ok, PakDocument47 pagesMotoric Central Nervous System: Dr. Ridwan Harrianto MHSC (Om) SP - Ok, PakMahasiswa StrugleNo ratings yet
- Physiology of Motor TractsDocument34 pagesPhysiology of Motor TractsNiko MartinNo ratings yet
- Jingying T.A. Department of PhysiologyDocument19 pagesJingying T.A. Department of Physiologyapi-19916399No ratings yet
- Central Components of The Motorsystemand Clinical Syndromes of Lesions Affecting ThemDocument5 pagesCentral Components of The Motorsystemand Clinical Syndromes of Lesions Affecting ThemItzel RomualdoNo ratings yet
- Methodic Materials MovementDocument20 pagesMethodic Materials MovementKapil PancholiNo ratings yet
- Motor System: G. Arveladze N. MalashkhiaDocument17 pagesMotor System: G. Arveladze N. MalashkhialuckyNo ratings yet
- Pyramidal 2012 PDFDocument63 pagesPyramidal 2012 PDFlovelots1234No ratings yet
- 2.motor Cotex and Tracts IDocument7 pages2.motor Cotex and Tracts Im6000000No ratings yet
- Neuro anatomy, motor neuronDocument9 pagesNeuro anatomy, motor neuronMichele Silva PiresNo ratings yet
- Neurophysiology II 2023Document90 pagesNeurophysiology II 2023trsvscpz79No ratings yet
- Descending TractsDocument24 pagesDescending Tractssalmankhan09215No ratings yet
- Motor System: Department of Anatomy, Yonsei University College of MedicineDocument60 pagesMotor System: Department of Anatomy, Yonsei University College of MedicineJetindar PuriNo ratings yet
- UMNL vs LMNLDocument14 pagesUMNL vs LMNLasif charsiNo ratings yet
- Motor SystemDocument49 pagesMotor SystemAhaisibwe GordonNo ratings yet
- Control of Posture & MovementDocument10 pagesControl of Posture & MovementPatterson MachariaNo ratings yet
- LECTURE On Spinal CordDocument11 pagesLECTURE On Spinal CordElijah KamaniNo ratings yet
- CORTICAL & BRAINSTEM CONTROL OF MOTOR FUNCTIONSDocument268 pagesCORTICAL & BRAINSTEM CONTROL OF MOTOR FUNCTIONSsaraNo ratings yet
- Motoric System: Anggraeni Janar WulanDocument44 pagesMotoric System: Anggraeni Janar WulanNadiarosmaliaNo ratings yet
- 3motor TestingDocument74 pages3motor Testing2013SecBNo ratings yet
- Motor Systems 10 05Document11 pagesMotor Systems 10 05souvik5000100% (1)
- Lecture 3 Figure 1 - Motor TractsDocument9 pagesLecture 3 Figure 1 - Motor TractsSusanaGonzálezFernándezNo ratings yet
- R.N. Kapoor Memorial Homoeopathic Hospital & Medical College, INDOREDocument12 pagesR.N. Kapoor Memorial Homoeopathic Hospital & Medical College, INDOREvinay patidar100% (1)
- L1 Motor Function of CNSDocument48 pagesL1 Motor Function of CNSAhmed JawdetNo ratings yet
- Motor Pathways Anatomy LecturesDocument24 pagesMotor Pathways Anatomy LecturesSindile MchunuNo ratings yet
- Motor TractDocument4 pagesMotor TractRaden Achmad Candra PutraNo ratings yet
- Types of ParaparesisDocument4 pagesTypes of ParaparesisMohamad Arbian KarimNo ratings yet
- 07c - Spinal Cord - Descending Tracts - DR Najeeb VideosDocument19 pages07c - Spinal Cord - Descending Tracts - DR Najeeb Videoshiba jasimNo ratings yet
- Upper and Lower Motor NeuronDocument22 pagesUpper and Lower Motor NeuronSry Hartaty WahidNo ratings yet
- The White Matter of The Spinal CordDocument7 pagesThe White Matter of The Spinal Cordalywaly2003No ratings yet
- Neuroanatomy, Upper Motor Neuron Lesion - StatPearls - NCBI BookshelfDocument10 pagesNeuroanatomy, Upper Motor Neuron Lesion - StatPearls - NCBI BookshelfYanasta Yudo PratamaNo ratings yet
- C 55 Motor Cortex & Corticospinal TractDocument42 pagesC 55 Motor Cortex & Corticospinal TractpixiemedicNo ratings yet
- Sectn 1 Nervous Syst OrgnznDocument52 pagesSectn 1 Nervous Syst OrgnznAparna Mangalore MohanNo ratings yet
- Disorders of Upper and Lower Motor NeuronsDocument38 pagesDisorders of Upper and Lower Motor NeuronsDavid ParraNo ratings yet
- Motor Functions of Spinal CordDocument43 pagesMotor Functions of Spinal CordEugeniu CoretchiNo ratings yet
- Neuroanatomy, Extrapyramidal System: AuthorsDocument7 pagesNeuroanatomy, Extrapyramidal System: AuthorsDiana CastilloNo ratings yet
- The Motor System Lecture 1 OverviewDocument7 pagesThe Motor System Lecture 1 OverviewUsman Ali AkbarNo ratings yet
- Major Neurological Syndromes PDFDocument260 pagesMajor Neurological Syndromes PDFVirlan Vasile Catalin100% (1)
- SNC EEG MalmivuoDocument10 pagesSNC EEG MalmivuoAdam SamenezesNo ratings yet
- Motor Cortex Pyramidal ExtrapyramidalDocument22 pagesMotor Cortex Pyramidal ExtrapyramidalJOSE ARTURO LOZANO CRUZNo ratings yet
- Neuro AnatomyDocument26 pagesNeuro Anatomymeryclave345No ratings yet
- Motoric SystemDocument32 pagesMotoric SystemAnisa Zulfiya RahmahNo ratings yet
- Physio - Psych Chapter-8 - Control-Of-Movemnt - Fact-SheetDocument9 pagesPhysio - Psych Chapter-8 - Control-Of-Movemnt - Fact-SheetJustynmae JusainNo ratings yet
- Corticospinal Tract: Functions and Clinical RelevanceDocument4 pagesCorticospinal Tract: Functions and Clinical RelevanceNrs Sani Sule MashiNo ratings yet
- 2nd Year Key of SEQs 17-10-12Document7 pages2nd Year Key of SEQs 17-10-12Mudassar RoomiNo ratings yet
- SCI Management ExtrasDocument2 pagesSCI Management ExtrasLoredana TaclitNo ratings yet
- Neuroanatomy, Extrapyramidal System - StatPearls - NCBI BookshelfDocument7 pagesNeuroanatomy, Extrapyramidal System - StatPearls - NCBI Bookshelfhermalina sabruNo ratings yet
- Spinal Cord Physiology & Anatomy: ObjectivesDocument9 pagesSpinal Cord Physiology & Anatomy: ObjectivesgrabearteNo ratings yet
- Lo 1 Week 5 NeuroDocument36 pagesLo 1 Week 5 NeuroInna DamaNo ratings yet
- Cerebellum and Basal Ganglia Anatomy and FunctionsDocument12 pagesCerebellum and Basal Ganglia Anatomy and Functionssimi yNo ratings yet
- Neuroanatomy SAQs AssignmentDocument8 pagesNeuroanatomy SAQs Assignmentaimy.palawataraNo ratings yet
- The descending pathways that control motor activityDocument2 pagesThe descending pathways that control motor activityalmastar officeNo ratings yet
- Introduction To Nervous SystemDocument4 pagesIntroduction To Nervous SystemErnie G. Bautista II, RN, MD100% (1)
- Brachial PlexusDocument6 pagesBrachial PlexusMuhamad SdeqNo ratings yet
- Spinal Cord LesionsDocument110 pagesSpinal Cord Lesionsgtaha80100% (1)
- Brachial Plexus InjuriesDocument46 pagesBrachial Plexus Injuriesnams orthoNo ratings yet
- Modern Review: Gross Anatomy of BrainDocument32 pagesModern Review: Gross Anatomy of BrainVENU B ANo ratings yet
- Upper Motor Neuron Lesion Symptoms and ManagementDocument14 pagesUpper Motor Neuron Lesion Symptoms and ManagementAnonymous 6MGui8dqNo ratings yet
- LBM 2 THTDocument20 pagesLBM 2 THTelly nurkhikmahNo ratings yet
- Reorganization of a Spinal Motoneuron Nucleus following Autologous Nerve Graft in the RatFrom EverandReorganization of a Spinal Motoneuron Nucleus following Autologous Nerve Graft in the RatNo ratings yet
- Drug Abuse in WorkplaceDocument2 pagesDrug Abuse in Workplacesimi yNo ratings yet
- Benign Ovarian TumorsDocument38 pagesBenign Ovarian Tumorssimi yNo ratings yet
- Inflammation DetailedDocument12 pagesInflammation Detailedsimi yNo ratings yet
- Chapter-Spinal CordDocument57 pagesChapter-Spinal Cordsimi yNo ratings yet
- Pharma Mcq'sDocument47 pagesPharma Mcq'ssimi yNo ratings yet
- Safety and Health at Workplace During The Times of COVID-19Document1 pageSafety and Health at Workplace During The Times of COVID-19simi yNo ratings yet
- Chronic Otitis Media (Mesotympanitis. Epitympanitis) - Otogenous Intracranial ComplicationsDocument53 pagesChronic Otitis Media (Mesotympanitis. Epitympanitis) - Otogenous Intracranial Complicationssimi yNo ratings yet
- Physiological Mechanisms of Recovery ProcessesDocument2 pagesPhysiological Mechanisms of Recovery Processessimi yNo ratings yet
- Benign Tumors of Female Genital OrgansDocument37 pagesBenign Tumors of Female Genital Organssimi yNo ratings yet
- Acute Appendicitis Complications and TreatmentDocument28 pagesAcute Appendicitis Complications and Treatmentsimi yNo ratings yet
- Antral Puncture and LavageDocument9 pagesAntral Puncture and Lavagesimi yNo ratings yet
- Spinal Orthotics LectureDocument80 pagesSpinal Orthotics Lecturesimi y100% (1)
- Fibromyalgia PDFDocument14 pagesFibromyalgia PDFsimi yNo ratings yet
- Throat Pharynx AcuteTonsillitisQuinsy ENT LecturesDocument25 pagesThroat Pharynx AcuteTonsillitisQuinsy ENT LecturesNoviera LarasatiNo ratings yet
- Myofascial Pain SyndromeDocument10 pagesMyofascial Pain Syndromesimi yNo ratings yet
- Bedsores PDFDocument13 pagesBedsores PDFsimi yNo ratings yet
- Clinical Cases NeurologyDocument200 pagesClinical Cases Neurologysimi y100% (1)
- Glucose-6-Phosphate Dehydrogenase Deficiency Medical ResearchDocument2 pagesGlucose-6-Phosphate Dehydrogenase Deficiency Medical Researchsimi yNo ratings yet
- Everything You Need to Know About Megag.comDocument572 pagesEverything You Need to Know About Megag.comsimi y100% (3)
- Cerebellum and Basal Ganglia Anatomy and FunctionsDocument12 pagesCerebellum and Basal Ganglia Anatomy and Functionssimi yNo ratings yet
- Obesity PDFDocument8 pagesObesity PDFsimi yNo ratings yet
- Teast Questions (Gynecology)Document41 pagesTeast Questions (Gynecology)simi yNo ratings yet
- Opthalmlogy MCQsDocument19 pagesOpthalmlogy MCQssimi y100% (2)
- MCQDocument20 pagesMCQPeter Osundwa Kiteki100% (1)
- Key Points:: Questions For StudentsDocument19 pagesKey Points:: Questions For Studentssimi yNo ratings yet
- Gynecological diagnoses and treatment tacticsDocument19 pagesGynecological diagnoses and treatment tacticssimi yNo ratings yet
- Opthalmlogy MCQsDocument19 pagesOpthalmlogy MCQssimi y100% (2)
- Spinal CordDocument15 pagesSpinal Cordsimi y100% (1)
- ENT TraumasDocument8 pagesENT Traumassimi yNo ratings yet
- Lamotrigine and Other Antiepileptics On Sleep Architecture - No Effect PDFDocument5 pagesLamotrigine and Other Antiepileptics On Sleep Architecture - No Effect PDFNones NoneachNo ratings yet
- CT ReportsDocument3 pagesCT Reportssukesh sukesh100% (1)
- Drugs Acting On Respiratory SystemDocument15 pagesDrugs Acting On Respiratory SystemQusai BassamNo ratings yet
- Ophthalmology (Final) PDFDocument15 pagesOphthalmology (Final) PDFadi100% (2)
- Estradiol 10mcg (Vagifen)Document13 pagesEstradiol 10mcg (Vagifen)asdwasdNo ratings yet
- Wu Et Al. - 2013 - Phenytoin A Guide To Therapeutic Drug MonitoringDocument5 pagesWu Et Al. - 2013 - Phenytoin A Guide To Therapeutic Drug MonitoringfachriybalafifNo ratings yet
- MATERNALDocument14 pagesMATERNALjhenwilliamsNo ratings yet
- Morbidity and Mortality Review for December and JanuaryDocument68 pagesMorbidity and Mortality Review for December and Januaryndifor bonnyNo ratings yet
- Elderly HandbookDocument95 pagesElderly HandbookJojo ChuaNo ratings yet
- Nursing Test 2 (NP Iii)Document19 pagesNursing Test 2 (NP Iii)Yuxin LiuNo ratings yet
- Beyond Bowels: Understanding Co-existing Symptoms in IBSDocument8 pagesBeyond Bowels: Understanding Co-existing Symptoms in IBSparthibanemails5779No ratings yet
- Super Simplified Pathology Hematology - Dr. Priyanka SachdevDocument500 pagesSuper Simplified Pathology Hematology - Dr. Priyanka SachdevMohd SaquibNo ratings yet
- The Urinary System: Organs, Nephrons, and Urine FormationDocument36 pagesThe Urinary System: Organs, Nephrons, and Urine FormationSura MaduNo ratings yet
- Dental Considerations in AnemiaDocument26 pagesDental Considerations in AnemiaKalpanaNo ratings yet
- Clinical Neurophysiology of The Vestibular System (001-057) PDFDocument57 pagesClinical Neurophysiology of The Vestibular System (001-057) PDFAriel CarterNo ratings yet
- Identifying Chromosomes 12 and 14Document3 pagesIdentifying Chromosomes 12 and 14AstatinNo ratings yet
- Systemic Sclerosis in Adults Part II Management and Therapeutics 2Document23 pagesSystemic Sclerosis in Adults Part II Management and Therapeutics 2วสุชล ชัยชาญNo ratings yet
- Mur. - Magnesia Phos.: The Tissue RemediesDocument23 pagesMur. - Magnesia Phos.: The Tissue RemediesSundar RajanNo ratings yet
- Harrison2003 Hair Loss ChildrenDocument14 pagesHarrison2003 Hair Loss ChildrenErnawati HidayatNo ratings yet
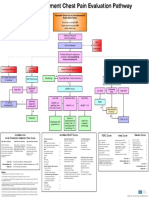
- Emergency Department Chest Pain Evaluation PathwayDocument2 pagesEmergency Department Chest Pain Evaluation Pathwaymuhammad sajidNo ratings yet
- Intro To TDM and ToxicologyDocument46 pagesIntro To TDM and ToxicologyAl-hadad AndromacheNo ratings yet
- Gen Path Case StudyDocument3 pagesGen Path Case Studydex7reme0% (1)
- Anemia.: Seminar OnDocument24 pagesAnemia.: Seminar OnAlma Susan100% (1)
- Post Natal AssessmentDocument8 pagesPost Natal Assessmentmohapatra devNo ratings yet
- Motor Speech Disorders: Clues To Neurologic Diagnosis: Joseph R. DuffyDocument19 pagesMotor Speech Disorders: Clues To Neurologic Diagnosis: Joseph R. DuffyCindy Arriagada CarrascoNo ratings yet
- CNS case proforma for stroke evaluationDocument2 pagesCNS case proforma for stroke evaluationRiyaSingh100% (1)
- Vildagliptin + Metformin (Eucreas) PDFDocument19 pagesVildagliptin + Metformin (Eucreas) PDFddandan_2No ratings yet
- Clinical Radiology For PediatriciansDocument221 pagesClinical Radiology For PediatriciansMihaela100% (2)
- Eidon - Atlas Catalog WebDocument51 pagesEidon - Atlas Catalog Webefze71No ratings yet
- Curcumin Role in ParaproteinemiaDocument18 pagesCurcumin Role in ParaproteinemiaINDIRAKALYANINo ratings yet