You might also like
- Basic Principles in Occupational Hygiene: Evah MainaDocument35 pagesBasic Principles in Occupational Hygiene: Evah MainaMokua FedinardNo ratings yet
- Clinical Pathology MCQs and Ansewrs PDFDocument29 pagesClinical Pathology MCQs and Ansewrs PDFAmeer MattaNo ratings yet
- SOP On Cleaning and Sanitization in PharmaceuticalljhiuDocument13 pagesSOP On Cleaning and Sanitization in PharmaceuticalljhiuMahadi Hasan Khan0% (1)
- Rtac IomDocument130 pagesRtac Iomfarshan296015No ratings yet
- AHA-ECC Guidance For Resuscitation For Patients With Suspected or Confirmed COVID-19 - Version 9 May 2020 (Ali Haedar)Document66 pagesAHA-ECC Guidance For Resuscitation For Patients With Suspected or Confirmed COVID-19 - Version 9 May 2020 (Ali Haedar)Herru Komarudin100% (2)
- Principle, Instrumentation and Application of HPLC: High Performance Liquid Chromatography (HPLCDocument48 pagesPrinciple, Instrumentation and Application of HPLC: High Performance Liquid Chromatography (HPLCMahadi Hasan Khan100% (3)
- Outdoors Club-7Document2 pagesOutdoors Club-7Nguyễn Huyền Trang100% (2)
- Xavier University - Ateneo de Cagayan College of Nursing S.Y. 2020-2021Document5 pagesXavier University - Ateneo de Cagayan College of Nursing S.Y. 2020-2021Dudil GoatNo ratings yet
- Purification Rundown Delivery Manual PDFDocument251 pagesPurification Rundown Delivery Manual PDFjohnloftus100% (1)
- General Dental Syllabus and Guidance NotesDocument23 pagesGeneral Dental Syllabus and Guidance NotesRajitha DilhanNo ratings yet
- Know Your Customer Details FormatDocument21 pagesKnow Your Customer Details FormatNiklesh ChandakNo ratings yet
- Physical Education: Quarter 4Document15 pagesPhysical Education: Quarter 4BookNo ratings yet
- Department of Public Works and Highways: Central OfficeDocument17 pagesDepartment of Public Works and Highways: Central OfficeJohn Bert OnrubiaNo ratings yet
- A Protocol of Infection Control For Mechanical Thrombectomy in Possible COVID-19 Patients: Tokai University COVID-19 ManualDocument5 pagesA Protocol of Infection Control For Mechanical Thrombectomy in Possible COVID-19 Patients: Tokai University COVID-19 ManualMartha OktaviaNo ratings yet
- It Wasn't Raining When Noah Built The ArkDocument4 pagesIt Wasn't Raining When Noah Built The ArkocramusNo ratings yet
- Precautions For Operating Room Team Members During The COVID-19 PandemicDocument4 pagesPrecautions For Operating Room Team Members During The COVID-19 Pandemicjhon neiffer alberto mosquera zeaNo ratings yet
- Anest, 12 ChaiwatDocument4 pagesAnest, 12 ChaiwatHainey GayleNo ratings yet
- Jamaotolaryngology Givi 2020 SC 200001Document6 pagesJamaotolaryngology Givi 2020 SC 200001dina ayu SeptianiNo ratings yet
- Jama Kibbe 2020 VP 200172 1600712179.77638Document2 pagesJama Kibbe 2020 VP 200172 1600712179.77638Gleice ReinertNo ratings yet
- RRL 1Document5 pagesRRL 1Boy MadNo ratings yet
- Managing Surgical Patients With A COVID-19 Infection in The Operating Experience Indonesia - Gezy Elsevier 2021Document9 pagesManaging Surgical Patients With A COVID-19 Infection in The Operating Experience Indonesia - Gezy Elsevier 2021Fransisca Dewi KumalaNo ratings yet
- Diagnostic Ultrasound Services During The Coronavirus Disease (COVID-19) PandemicDocument6 pagesDiagnostic Ultrasound Services During The Coronavirus Disease (COVID-19) Pandemiczahra ebrahimiNo ratings yet
- Current Problems in Diagnostic Radiology 50 (2021) 284 287Document4 pagesCurrent Problems in Diagnostic Radiology 50 (2021) 284 287Leonard AcsinteNo ratings yet
- Surgery in Covid19 - 2Document4 pagesSurgery in Covid19 - 2Anonymous VV4iStxLNo ratings yet
- COVID-19: A Quick Look at Aspects of Critical CareDocument5 pagesCOVID-19: A Quick Look at Aspects of Critical CareJbarrianNo ratings yet
- Jurnal Deskriptif IngDocument6 pagesJurnal Deskriptif IngAulin putri damayantiNo ratings yet
- Radiology Department Strategies To Protect RadioloDocument5 pagesRadiology Department Strategies To Protect RadioloeugeniaNo ratings yet
- Setup of A Dedicated Coronavirus Intensive Care Unit: Logistical AspectsDocument3 pagesSetup of A Dedicated Coronavirus Intensive Care Unit: Logistical AspectsBAGUIO CATSNo ratings yet
- Guidance For Resuscitation For Patients With Suspected or Confirmed COVID-19 - Version 9 May 2020 (Ali Haedar)Document66 pagesGuidance For Resuscitation For Patients With Suspected or Confirmed COVID-19 - Version 9 May 2020 (Ali Haedar)Ammey JoizeNo ratings yet
- Surgery in Covid-19Document7 pagesSurgery in Covid-19Anonymous VV4iStxLNo ratings yet
- Ippolito 2020Document9 pagesIppolito 2020KalpanaNo ratings yet
- How Can Mobile Suction Systems Help You and Your Patients?Document1 pageHow Can Mobile Suction Systems Help You and Your Patients?Nanang YlNo ratings yet
- Tx. COVID 19 en UCIDocument6 pagesTx. COVID 19 en UCIVictor Augusto Ávila HernándezNo ratings yet
- COVID-19 Management in HongKongDocument1 pageCOVID-19 Management in HongKongShahzad KamranNo ratings yet
- Departmental Experience and Lessons Learned With Accelerated Introduction of Telemedicine During The COVID-19 CrisisDocument8 pagesDepartmental Experience and Lessons Learned With Accelerated Introduction of Telemedicine During The COVID-19 Crisistresy kalawaNo ratings yet
- Molecular Screening and Diagnosis of SARDocument6 pagesMolecular Screening and Diagnosis of SARgygyNo ratings yet
- Intensive & Critical Care Nursing: M. Sanz-Moncusí, J. Rosselló-Sancho, J.M. Garcia-AlaminoDocument3 pagesIntensive & Critical Care Nursing: M. Sanz-Moncusí, J. Rosselló-Sancho, J.M. Garcia-AlaminoJimena Vásquez RodríguezNo ratings yet
- Impact of Coronavirus (COVID-19) On Otolaryngologic Surgery: Brief CommentaryDocument8 pagesImpact of Coronavirus (COVID-19) On Otolaryngologic Surgery: Brief CommentaryHesbon MomanyiNo ratings yet
- CGH PPT - CCCDocument45 pagesCGH PPT - CCCIan GreyNo ratings yet
- Jamda: Richard M. Lynch PHD, Reginald Goring BsDocument2 pagesJamda: Richard M. Lynch PHD, Reginald Goring BsWidarma Atmaja, I KomangNo ratings yet
- Prone Position Pressure Sores in The COVID 19 PANDEMIC THE MADRID EXPERIENCEDocument8 pagesProne Position Pressure Sores in The COVID 19 PANDEMIC THE MADRID EXPERIENCEduckjqtNo ratings yet
- 2020 Article 1361-2Document3 pages2020 Article 1361-2Maria Alejandra AconchaNo ratings yet
- Perioperative Considerstions in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic PatientsDocument23 pagesPerioperative Considerstions in Urgent Surgical Care of Suspected and Confirmed COVID-19 Orthopaedic PatientsDoctor's BettaNo ratings yet
- Airway Management of Patients With COVID-19 by Specialist Tracheal Intubation TeamsDocument8 pagesAirway Management of Patients With COVID-19 by Specialist Tracheal Intubation TeamsFaisal ShamimNo ratings yet
- Managing COVID-19 in Low-And Middle-Income Countries: The Public Health ResponseDocument2 pagesManaging COVID-19 in Low-And Middle-Income Countries: The Public Health ResponseNuzlaNo ratings yet
- Prolonged Prone Position Ventilation For Sars-Cov-2 Patients Is Feasible and EffectiveDocument3 pagesProlonged Prone Position Ventilation For Sars-Cov-2 Patients Is Feasible and Effectivecarlos_julianNo ratings yet
- 10 1016@j Breast 2020 04 006Document9 pages10 1016@j Breast 2020 04 006Alberto AlexandruNo ratings yet
- Aerosol-Generating Procedures inDocument5 pagesAerosol-Generating Procedures inHaris WidodoNo ratings yet
- Acute Care PT For Covid 19 PatientsDocument17 pagesAcute Care PT For Covid 19 PatientsSelvi SoundararajanNo ratings yet
- A K N H: Evidence Based Clinical Practice Guidelines For The Management of COVID-19Document15 pagesA K N H: Evidence Based Clinical Practice Guidelines For The Management of COVID-19AL AHLINo ratings yet
- Jama Murthy 2020 It 200008Document2 pagesJama Murthy 2020 It 200008jorgeNo ratings yet
- Infection Prevention and Control (IPC) Protocol For Surgical Procedures During COVID-19: AdultDocument8 pagesInfection Prevention and Control (IPC) Protocol For Surgical Procedures During COVID-19: AdultbasukiNo ratings yet
- Guiding Airway Management and Personal Protective Equipment For COVID-19 Intubation TeamsDocument2 pagesGuiding Airway Management and Personal Protective Equipment For COVID-19 Intubation TeamsahmdamnnNo ratings yet
- 2 Epitaxis Covid19Document3 pages2 Epitaxis Covid19andinNo ratings yet
- N 5 RFTKV BGYTs 6 N Vyd 7 GMC 3 CDocument18 pagesN 5 RFTKV BGYTs 6 N Vyd 7 GMC 3 CGeysel SuarezNo ratings yet
- Clinical Commentary On An Auricular Marker Associated With COVID-19Document2 pagesClinical Commentary On An Auricular Marker Associated With COVID-19yan92120No ratings yet
- Screening and Triage of Patients With Suspected or Confirmed COVID-19Document24 pagesScreening and Triage of Patients With Suspected or Confirmed COVID-19LinaRizaNavalesMonteroNo ratings yet
- Recommendations For Local-Regional Anesthesia During The COVID-19 PandemicDocument6 pagesRecommendations For Local-Regional Anesthesia During The COVID-19 PandemictitalitaNo ratings yet
- Mja2 50598Document10 pagesMja2 50598Andi Astrid AmaliaNo ratings yet
- Consensus Statement: Safe Airway Society Principles of Airway Management and Tracheal Intubation Specific To The COVID-19 Adult Patient GroupDocument10 pagesConsensus Statement: Safe Airway Society Principles of Airway Management and Tracheal Intubation Specific To The COVID-19 Adult Patient GroupMeska AmeliaNo ratings yet
- COVID 19 and ENT SurgeryDocument6 pagesCOVID 19 and ENT SurgeryYukiko CalimutanNo ratings yet
- Intensive Care Unit Setup For COVID-19Document7 pagesIntensive Care Unit Setup For COVID-19BAGUIO CATSNo ratings yet
- Review: Key MessagesDocument12 pagesReview: Key MessagesLuis Fernando PantojaNo ratings yet
- Adapting Urology Residency Training PIIS0090429520304520Document5 pagesAdapting Urology Residency Training PIIS0090429520304520Nidhin MathewNo ratings yet
- 2004 06912Document9 pages2004 06912Gaurav GaggarNo ratings yet
- Hygeia - An Automated Disinfection Booth Using FAR UVCDocument6 pagesHygeia - An Automated Disinfection Booth Using FAR UVCIOER International Multidisciplinary Research Journal ( IIMRJ)No ratings yet
- PIIS1201971220305294Document3 pagesPIIS1201971220305294kristina dewiNo ratings yet
- Int J Clinical Practice - 2021 - Acat - Comparison of Pirfenidone and Corticosteroid Treatments at The COVID 19 PneumoniaDocument12 pagesInt J Clinical Practice - 2021 - Acat - Comparison of Pirfenidone and Corticosteroid Treatments at The COVID 19 PneumoniaRebeca EscutiaNo ratings yet
- NUSRAT JAHAN MIM - ENG 105 Spring 2022 MidDocument13 pagesNUSRAT JAHAN MIM - ENG 105 Spring 2022 MidMahadi Hasan KhanNo ratings yet
- Essential Drugs Company Limited Job Circular 2022Document6 pagesEssential Drugs Company Limited Job Circular 2022Mahadi Hasan KhanNo ratings yet
- Choose The Best AnswerDocument4 pagesChoose The Best AnswerMahadi Hasan KhanNo ratings yet
- Nervous SystemDocument32 pagesNervous SystemMahadi Hasan KhanNo ratings yet
- AnswerDocument3 pagesAnswerMahadi Hasan KhanNo ratings yet
- Lecture-PPI 20230226Document25 pagesLecture-PPI 20230226Mahadi Hasan KhanNo ratings yet
- Intercultural CommunicationDocument4 pagesIntercultural CommunicationMahadi Hasan KhanNo ratings yet
- Biopharmaceutics-II - PHR 409 - One Compartmental Model - NSDocument66 pagesBiopharmaceutics-II - PHR 409 - One Compartmental Model - NSMahadi Hasan KhanNo ratings yet
- 0 - CNS BrainDocument21 pages0 - CNS BrainMahadi Hasan KhanNo ratings yet
- SOP On Cleaning and Sanitization in PharmaceuticalDocument7 pagesSOP On Cleaning and Sanitization in PharmaceuticalMahadi Hasan KhanNo ratings yet
- Standard Operating Procedure DeviationDocument4 pagesStandard Operating Procedure DeviationMahadi Hasan KhanNo ratings yet
- Access To Antibiotics in New Delhi, India: Implications For Antibiotic PolicyDocument13 pagesAccess To Antibiotics in New Delhi, India: Implications For Antibiotic PolicyMahadi Hasan KhanNo ratings yet
- Salivary SecretionDocument10 pagesSalivary SecretionMahadi Hasan KhanNo ratings yet
- PHA312L-Biochemistry and Molecular BiologyDocument13 pagesPHA312L-Biochemistry and Molecular BiologyMahadi Hasan KhanNo ratings yet
- Application of Microbiological Assay To Determine The Potency of Intravenous AntibioticsDocument5 pagesApplication of Microbiological Assay To Determine The Potency of Intravenous AntibioticsMahadi Hasan KhanNo ratings yet
- Assignment: Title: Physiological Functions, Regulation and Abnormalities of Cortisol SecretionDocument2 pagesAssignment: Title: Physiological Functions, Regulation and Abnormalities of Cortisol SecretionMahadi Hasan KhanNo ratings yet
- Assignment Cover Page FormatDocument3 pagesAssignment Cover Page FormatMahadi Hasan KhanNo ratings yet
- 209 Assignment Table 2Document6 pages209 Assignment Table 2Mahadi Hasan KhanNo ratings yet
- Draft 203 Gi TractDocument7 pagesDraft 203 Gi TractMahadi Hasan KhanNo ratings yet
- Sustainable Indoor Air Quality IAQ in Hospital BuiDocument7 pagesSustainable Indoor Air Quality IAQ in Hospital BuiMahadi Hasan KhanNo ratings yet
- Assignment Analysis Final2Document8 pagesAssignment Analysis Final2Mahadi Hasan KhanNo ratings yet
- Friday 17 January 2020: ChemistryDocument16 pagesFriday 17 January 2020: ChemistryMahadi Hasan KhanNo ratings yet
- Course Code: PHA 305 UV-Visible SpectrophotometryDocument38 pagesCourse Code: PHA 305 UV-Visible SpectrophotometryMahadi Hasan KhanNo ratings yet
- 209 Assignment TableDocument9 pages209 Assignment TableMahadi Hasan KhanNo ratings yet
- ASSIGNMENT On FLUOROMETRY AND POLARIMETRY Pha 305 Sec-1 Group-08Document30 pagesASSIGNMENT On FLUOROMETRY AND POLARIMETRY Pha 305 Sec-1 Group-08Mahadi Hasan KhanNo ratings yet
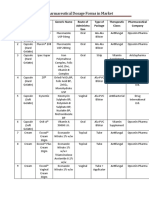
- Some Pharmaceutical Dosage Forms in MarketDocument6 pagesSome Pharmaceutical Dosage Forms in MarketMahadi Hasan KhanNo ratings yet
- Mark Scheme (Results) January 2020Document34 pagesMark Scheme (Results) January 2020Mahadi Hasan KhanNo ratings yet
- Research ArticleDocument4 pagesResearch ArticleBharathi RagavanNo ratings yet
- Ielts GT Writing Task 2Document20 pagesIelts GT Writing Task 2Raga SownthariyaNo ratings yet
- Wasike Esker: Personal ProfileDocument3 pagesWasike Esker: Personal ProfileprincewNo ratings yet
- Build A HomeDocument160 pagesBuild A HomepacoNo ratings yet
- Management of Neck Pain and Associated DisordersDocument24 pagesManagement of Neck Pain and Associated DisordersManuel OlarteNo ratings yet
- Business Plan 2018-2021: Potatoes Export ToDocument4 pagesBusiness Plan 2018-2021: Potatoes Export ToSumati Vidya KendraNo ratings yet
- Stok Opname Ok Feb 2021Document14 pagesStok Opname Ok Feb 2021fiannysjahjadiNo ratings yet
- Response To Stress PresentationDocument27 pagesResponse To Stress PresentationMohit PunaniNo ratings yet
- Kelly Gerhart: Work ExperienceDocument3 pagesKelly Gerhart: Work ExperienceJay KulkarniNo ratings yet
- Nursing Care Plan: Cues Nursing Diagnosis Goals Adnd Desired Outcome Nursing Intervention Implementation EvaluationDocument5 pagesNursing Care Plan: Cues Nursing Diagnosis Goals Adnd Desired Outcome Nursing Intervention Implementation EvaluationNur SanaaniNo ratings yet
- MSDS - Fuel-Protect, Keep Clean Solution, For Diesel InjectorDocument5 pagesMSDS - Fuel-Protect, Keep Clean Solution, For Diesel InjectorDaniel OlanoNo ratings yet
- Alcohol Abuse Among The Youths of The Northern Cape Province, South AfricaDocument7 pagesAlcohol Abuse Among The Youths of The Northern Cape Province, South AfricaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Navigating Cultures For Health EquityDocument5 pagesNavigating Cultures For Health EquityRootNo ratings yet
- RA-Vocabulary (U1-L1-family Relation and Friendship)Document2 pagesRA-Vocabulary (U1-L1-family Relation and Friendship)Kiên ĐinhNo ratings yet
- CMCM Prestations 2022 EN-WebDocument28 pagesCMCM Prestations 2022 EN-WebMichel Bou MoussaNo ratings yet
- Siddha Maruthuva ArignarDocument3 pagesSiddha Maruthuva ArignarDead Squad GamingNo ratings yet
- Discharge Plan For Dengue Fever 1Document4 pagesDischarge Plan For Dengue Fever 1Cecille Ursua0% (1)
- Group 4 QuestionnaireDocument9 pagesGroup 4 QuestionnaireJohn Denver De la CruzNo ratings yet
- Causes and Effects of TerrorismDocument3 pagesCauses and Effects of TerrorismSharjeel Hashmi100% (3)
- End-Of-life Care Volunteers A Systematic Review of The LiteratureDocument4 pagesEnd-Of-life Care Volunteers A Systematic Review of The LiteratureafmzuiffugjdffNo ratings yet
- At The End of The Course, Students Are Expected ToDocument3 pagesAt The End of The Course, Students Are Expected ToTEOFILO PALSIMON JR.No ratings yet
- The Soloist - Critical AnalysisDocument1 pageThe Soloist - Critical AnalysisShraddhaNo ratings yet