You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- CBSE Sample Paper For Class 6 Maths With Solutions - Mock Paper-2Document14 pagesCBSE Sample Paper For Class 6 Maths With Solutions - Mock Paper-2arun_ioclNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Fill in The Short Vowel PDFDocument1 pageFill in The Short Vowel PDFarun_ioclNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- NewGSG CamtasiaCombined2014 PDFDocument11 pagesNewGSG CamtasiaCombined2014 PDFarun_ioclNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Medical Bill 2Document1 pageMedical Bill 2arun_ioclNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Toll Receipt 2 - WB30AB1837Document1 pageToll Receipt 2 - WB30AB1837arun_ioclNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Fill in The Short VowelDocument1 pageFill in The Short Vowelarun_ioclNo ratings yet
- Novel Configuration For Near-IR Analysis of Refinery LPG Composition and ControlDocument5 pagesNovel Configuration For Near-IR Analysis of Refinery LPG Composition and Controlarun_ioclNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Branch: Krishnagar, Dist: Nadia, W.B. (Any Nationalised Banks)Document1 pageBranch: Krishnagar, Dist: Nadia, W.B. (Any Nationalised Banks)SoumyadipHoreNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- CSR Assistance Application FormDocument3 pagesCSR Assistance Application Formarun_ioclNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Dr. Shivaji Basu: Medeguide Doctor eCVDocument1 pageDr. Shivaji Basu: Medeguide Doctor eCVarun_ioclNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- AcknowledgementDocument1 pageAcknowledgementarun_ioclNo ratings yet
- ERNiCu 7Document1 pageERNiCu 7arun_ioclNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Notice OCTT WT RescheduledDocument1 pageNotice OCTT WT Rescheduledarun_ioclNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
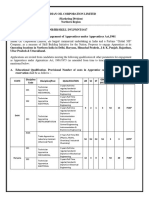
- Indian Oil Apprentice Recruitment 2017Document7 pagesIndian Oil Apprentice Recruitment 2017nidhi tripathiNo ratings yet
- Completion CertificateDocument1 pageCompletion Certificatearun_ioclNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Gail e ReceiptDocument1 pageGail e Receiptarun_ioclNo ratings yet
- Measurement Sheet: Haldia RefineryDocument2 pagesMeasurement Sheet: Haldia Refineryarun_ioclNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Measurement Sheet: Haldia RefineryDocument2 pagesMeasurement Sheet: Haldia Refineryarun_ioclNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- SAIL Bokaro Payment ReceiptDocument1 pageSAIL Bokaro Payment Receiptarun_ioclNo ratings yet
- VenuDocument4 pagesVenuarun_ioclNo ratings yet
- Time Sheet PB Aug16Document1 pageTime Sheet PB Aug16arun_ioclNo ratings yet
- IFFCO Third Party LiabilityDocument3 pagesIFFCO Third Party Liabilityarun_ioclNo ratings yet
- Time Sheet PB Sept 2016Document1 pageTime Sheet PB Sept 2016arun_ioclNo ratings yet
- Time Sheet PB July16Document1 pageTime Sheet PB July16arun_ioclNo ratings yet
- PDSBT-ST43-VP Manual: 1. Key Features 4. LED Light IndicationsDocument2 pagesPDSBT-ST43-VP Manual: 1. Key Features 4. LED Light Indicationsarun_ioclNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Gate Pass RenewalDocument1 pageGate Pass Renewalarun_ioclNo ratings yet
- PCN Level III BrochureDocument5 pagesPCN Level III Brochuremayav1100% (1)
- Bleeding in A NeonateDocument36 pagesBleeding in A NeonateDrBibek AgarwalNo ratings yet
- Oral Airway InsertionDocument3 pagesOral Airway InsertionSajid HolyNo ratings yet
- Radial Lead Varistors LA Varistor SeriesDocument13 pagesRadial Lead Varistors LA Varistor SeriesLeman SihotangNo ratings yet
- Basic Concepts and Applied Aspect of Sharir RachnaDocument122 pagesBasic Concepts and Applied Aspect of Sharir RachnaRam Krish100% (1)
- Ctaa040 - Ctaf080 - Test 4 Solution - 2023Document7 pagesCtaa040 - Ctaf080 - Test 4 Solution - 2023Given RefilweNo ratings yet
- Eye Essentials Cataract Assessment Classification and ManagementDocument245 pagesEye Essentials Cataract Assessment Classification and ManagementKyros1972No ratings yet
- Air Compressors: Instruction, Use and Maintenance ManualDocument66 pagesAir Compressors: Instruction, Use and Maintenance ManualYebrail Mojica RuizNo ratings yet
- Helicopter Logging Operations - ThesisDocument7 pagesHelicopter Logging Operations - ThesisAleš ŠtimecNo ratings yet
- Bio1 11 - 12 Q1 0501 FDDocument23 pagesBio1 11 - 12 Q1 0501 FDIsabelle SchollardNo ratings yet
- Positioning Strategy - Mineral WaterDocument2 pagesPositioning Strategy - Mineral WaterRakesh SelvamNo ratings yet
- CASE 1. Non-Cash Assets Are Sold For P 580,000Document3 pagesCASE 1. Non-Cash Assets Are Sold For P 580,000Riza Mae AlceNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ListwarehouseDocument1 pageListwarehouseKautilya KalyanNo ratings yet
- Emergency War Surgery Nato HandbookDocument384 pagesEmergency War Surgery Nato Handbookboubiyou100% (1)
- Theoretical Background: Theories Relevance To The Study SourcesDocument3 pagesTheoretical Background: Theories Relevance To The Study SourcesAdelfa Mae BerdonNo ratings yet
- PP Aaa PP1 141Document30 pagesPP Aaa PP1 141Rabah AmidiNo ratings yet
- Work Environment Act (1977:1160) : Chapter 1 Purpose and Scope of The ActDocument26 pagesWork Environment Act (1977:1160) : Chapter 1 Purpose and Scope of The ActNatalie BlackmoreNo ratings yet
- Pentacon Six-02Document28 pagesPentacon Six-02Melissa Moreira TYNo ratings yet
- Anti-Bribery and Corruption PolicyDocument2 pagesAnti-Bribery and Corruption PolicyAJAY PatilNo ratings yet
- CGMP Training ToolDocument21 pagesCGMP Training Toolbabusure99No ratings yet
- Rifle Threat Performance Matrix: SeriesDocument1 pageRifle Threat Performance Matrix: SeriesKuhnNo ratings yet
- Gut Health Elimination Diet Meal Plan FINALDocument9 pagesGut Health Elimination Diet Meal Plan FINALKimmy BathamNo ratings yet
- Case Analysis: Beth OwensDocument8 pagesCase Analysis: Beth OwensPhillip CookNo ratings yet
- Director's Update Our StudentsDocument23 pagesDirector's Update Our StudentsAdrian MojicaNo ratings yet
- Molarity, Molality, Normality, and Mass Percent Worksheet II Answer Key 11-12 PDFDocument3 pagesMolarity, Molality, Normality, and Mass Percent Worksheet II Answer Key 11-12 PDFGerald KamulanjeNo ratings yet
- 2-Phase Synchronous-Rectified Buck Controller For Mobile GPU PowerDocument18 pages2-Phase Synchronous-Rectified Buck Controller For Mobile GPU PowerMax Assistência TécnicaNo ratings yet
- MPX-200 Service Manual PDFDocument90 pagesMPX-200 Service Manual PDFvivijaNo ratings yet
- Final PR 2 CheckedDocument23 pagesFinal PR 2 CheckedCindy PalenNo ratings yet
- EASA Ops ProceduresDocument11 pagesEASA Ops ProceduresMoslem Grimaldi100% (4)
- Rovers - CH - 2 - Drug TherapyDocument28 pagesRovers - CH - 2 - Drug TherapyKhalid Bin AliNo ratings yet
- The Allied Valve Spares Manufacturer Company Maharashtra IndiaDocument10 pagesThe Allied Valve Spares Manufacturer Company Maharashtra IndiaThe Allied Valve Spares Manufacturer CompanyNo ratings yet