You might also like
- F 111 Final A 1 41Document41 pagesF 111 Final A 1 41Woestyn100% (1)
- Airline Transport Pilot and Aircraft Type Rating Practical Test StandardsDocument87 pagesAirline Transport Pilot and Aircraft Type Rating Practical Test Standardsmustang12484No ratings yet
- 727 ManualDocument211 pages727 ManualMarcela Arias Castro86% (7)
- ATA 23 - CommunicationsDocument70 pagesATA 23 - CommunicationsQuoc Tan HuynhNo ratings yet
- Airbus - CalloutsDocument32 pagesAirbus - CalloutsCarlos RicoNo ratings yet
- ApacheDocument22 pagesApacheAbhimanyu Singh100% (1)
- AIRBUS A320 Removal Power PlantDocument28 pagesAIRBUS A320 Removal Power PlantPanagiotis Diakidis100% (3)
- FAA Form 8070-1Document2 pagesFAA Form 8070-1Kivanc NerogluNo ratings yet
- Volare Questions - AerodynamicsDocument45 pagesVolare Questions - Aerodynamicspontoo67% (3)
- SFAR 88 Final RuleDocument30 pagesSFAR 88 Final RulePoshak Prasad GnawaliNo ratings yet
- Storage Periodic Ground ChecksDocument27 pagesStorage Periodic Ground ChecksJivendra KumarNo ratings yet
- 09 - Towing and TaxiingDocument56 pages09 - Towing and TaxiingMartin FeldmanNo ratings yet
- Powerplant Level 1rDocument220 pagesPowerplant Level 1rAbil Gilang -No ratings yet
- B1.1 Syllabus For WebsiteDocument40 pagesB1.1 Syllabus For WebsiteHannan Pasha100% (1)
- 47fueltankinerting 161122021407Document70 pages47fueltankinerting 161122021407coralonsoNo ratings yet
- BOEING 787 AIR CONDITIONING SYSTEM, Nasr, Ahmad Samir Ahmed A. AMTA 329 3BDocument9 pagesBOEING 787 AIR CONDITIONING SYSTEM, Nasr, Ahmad Samir Ahmed A. AMTA 329 3BBENo100% (1)
- 777F Air Conditioning Smoke or Fumes Odor v5Document4 pages777F Air Conditioning Smoke or Fumes Odor v5arizonaflyer1_732976No ratings yet
- 03 Documentation - 2Document54 pages03 Documentation - 2Renanto SuryadinataNo ratings yet
- SFAR88 EASA FueltanksafetyDocument95 pagesSFAR88 EASA FueltanksafetyEduardo RuizNo ratings yet
- Boeing 787 and Lithium Ion Battery FailureDocument3 pagesBoeing 787 and Lithium Ion Battery Failuresenkum812002No ratings yet
- 3.powerplant Level 1rDocument310 pages3.powerplant Level 1rChairul Ichwan100% (1)
- Layover Inspection Schedule Issue 06Document17 pagesLayover Inspection Schedule Issue 06Pankaj Khondge100% (1)
- 2007 - An Overview of Trends in Aircraft Maintenance Program DevelopmentDocument10 pages2007 - An Overview of Trends in Aircraft Maintenance Program DevelopmentJorgeCanoRamirez100% (1)
- A320fam Iae Ata80 Starting PDFDocument24 pagesA320fam Iae Ata80 Starting PDFshabbirjama103No ratings yet
- Flight Crew Operating Manual Preliminary Pages: Standard NomenclatureDocument10 pagesFlight Crew Operating Manual Preliminary Pages: Standard NomenclatureTyoNo ratings yet
- TTC Boeing 737CDocument4 pagesTTC Boeing 737CGuntur EkoNo ratings yet
- IGO Operations Manual PDFDocument2,251 pagesIGO Operations Manual PDFMardi Wirengkoso100% (1)
- Airbus H125 Airconditioning System - Caton Michael, Amta 329 3BDocument8 pagesAirbus H125 Airconditioning System - Caton Michael, Amta 329 3BBENoNo ratings yet
- ATA 49 RedactedDocument106 pagesATA 49 RedactedАлександър ГиневNo ratings yet
- Flight Control Surfaces RDocument23 pagesFlight Control Surfaces Rni'am tamami100% (1)
- Ata 21aircond l1Document42 pagesAta 21aircond l1svyat_kNo ratings yet
- Atr Airconditioning System MarzoDocument4 pagesAtr Airconditioning System MarzoBENoNo ratings yet
- De-Anti Icing of Aircraft On The Ground-Technical Information FormDocument48 pagesDe-Anti Icing of Aircraft On The Ground-Technical Information FormMurat DemirbaşNo ratings yet
- 74 L3 Oct07 XDocument20 pages74 L3 Oct07 XJimmy HaddadNo ratings yet
- Set12 Metallurgy 2,3,4,5,6Document19 pagesSet12 Metallurgy 2,3,4,5,6Pritamjit RoutNo ratings yet
- AMM - IGO - A318/A319/A320/A321 REV DATE: Aug 01/2021 Tail Number - MSN - FSN: VT-ILN - 10151 - 431Document6 pagesAMM - IGO - A318/A319/A320/A321 REV DATE: Aug 01/2021 Tail Number - MSN - FSN: VT-ILN - 10151 - 431Rameswar PradhanNo ratings yet
- Airbus A220 FamilyDocument1 pageAirbus A220 Familystrokeu02No ratings yet
- Aircraft Maintenace ProgrammDocument39 pagesAircraft Maintenace Programm4587560No ratings yet
- A318/A319/A320/A321: Service BulletinDocument23 pagesA318/A319/A320/A321: Service BulletinPradeep K sNo ratings yet
- Global Series Environmental Corrosion Guidelines - December 2016Document53 pagesGlobal Series Environmental Corrosion Guidelines - December 2016Faraz Khan100% (1)
- Planning and Design Fundamentals of AirportDocument17 pagesPlanning and Design Fundamentals of AirportFatima Ramilo Villanueva100% (1)
- SB PolicyDocument5 pagesSB PolicyEduardo MercadejasNo ratings yet
- On The Design and Structural Analysis o Fjet Engine Fan Blade StructuresDocument11 pagesOn The Design and Structural Analysis o Fjet Engine Fan Blade StructuresNico ScheggiaNo ratings yet
- Abbreviation Full Form Airbus AbbreviatiDocument106 pagesAbbreviation Full Form Airbus AbbreviatiDian PrasetyoNo ratings yet
- A F D X: Vionics Ull Uple Switched EthernetDocument61 pagesA F D X: Vionics Ull Uple Switched EthernetNiranjan MukeshNo ratings yet
- 71-00-00-710-006-B - Minimum Idle CheckDocument6 pages71-00-00-710-006-B - Minimum Idle CheckEder LucianoNo ratings yet
- 飞机英文缩写Document52 pages飞机英文缩写Haliunaa BatboldNo ratings yet
- Diapo AIRBUS - PpsDocument30 pagesDiapo AIRBUS - PpsbekarNo ratings yet
- An Overview of The Integrated Modular Avionics (Ima) ConceptDocument4 pagesAn Overview of The Integrated Modular Avionics (Ima) ConceptsofolaNo ratings yet
- Liebherr A380 Air Management PosterDocument1 pageLiebherr A380 Air Management PosterSathiya SeelanNo ratings yet
- Amm - 12 11 28 650 005 ADocument7 pagesAmm - 12 11 28 650 005 Araiday84No ratings yet
- Bei042 Aircraft InstrumentationDocument1 pageBei042 Aircraft Instrumentationgg.ganapathyNo ratings yet
- B 747 FPDocument11 pagesB 747 FPFayez Shakil AhmedNo ratings yet
- Modu 16 - Thrust Reversal SystemDocument10 pagesModu 16 - Thrust Reversal SystemHAFIDY RIZKY ILHAMSYAHNo ratings yet
- The 737 APUDocument1 pageThe 737 APUAhmad AlshiekhNo ratings yet
- ATA-22 TestDocument1 pageATA-22 TestJacob GallegosNo ratings yet
- A318/A319/A320/A321: Service BulletinDocument58 pagesA318/A319/A320/A321: Service BulletinPradeep K sNo ratings yet
- FRB Issue 2 Rev 0 July 2018 For Atr 42-320 For PrintingDocument33 pagesFRB Issue 2 Rev 0 July 2018 For Atr 42-320 For PrintingSujoy GhoshNo ratings yet
- Airbus AC A320 Jan16Document390 pagesAirbus AC A320 Jan16simon100% (1)
- List of Abbreviations: On A/C AllDocument102 pagesList of Abbreviations: On A/C AllKaren NersisyanNo ratings yet
- Ata 71 - B1 - Iae V2500Document61 pagesAta 71 - B1 - Iae V2500Abil Gilang -No ratings yet
- AtaDocument20 pagesAtaYousef AsmarNo ratings yet
- Development of Composite Fan SystemDocument5 pagesDevelopment of Composite Fan SystemnrNo ratings yet
- Avionics System (AVS) Aboard ATR - 600: ATA104-I General Familiarization Training CourseDocument19 pagesAvionics System (AVS) Aboard ATR - 600: ATA104-I General Familiarization Training CourseWilson Carlos SombiniNo ratings yet
- Aircraft ECS PDFDocument26 pagesAircraft ECS PDFrmdeca100% (1)
- A320neo FamilyDocument2 pagesA320neo FamilycarlosNo ratings yet
- ACARs Details PDFDocument5 pagesACARs Details PDFa pandaNo ratings yet
- Idg RemovalDocument12 pagesIdg Removalcristian reyes calbillanNo ratings yet
- A319 320 321 Autoflight PDFDocument0 pagesA319 320 321 Autoflight PDFDipendra SenNo ratings yet
- Stabilization and Dynamic of Premixed Swirling Flames: Prevaporized, Stratified, Partially, and Fully Premixed RegimesFrom EverandStabilization and Dynamic of Premixed Swirling Flames: Prevaporized, Stratified, Partially, and Fully Premixed RegimesNo ratings yet
- Aircraft Air-Conditionining System A340Document4 pagesAircraft Air-Conditionining System A340BENoNo ratings yet
- Amta 328Document17 pagesAmta 328BENoNo ratings yet
- MD369 Hughes 500: Maggay, Joana Marie V. Bs Aet - 3B AMTA 329 March 20, 2021Document3 pagesMD369 Hughes 500: Maggay, Joana Marie V. Bs Aet - 3B AMTA 329 March 20, 2021BENoNo ratings yet
- Rhezee Castillo Bs Aet 3B Airbus A320Document2 pagesRhezee Castillo Bs Aet 3B Airbus A320BENoNo ratings yet
- Dassault-Falcon7x Airconditioning System-John Rafael Ildefonso Am329 3BDocument7 pagesDassault-Falcon7x Airconditioning System-John Rafael Ildefonso Am329 3BBENoNo ratings yet
- Boeing 777 Airconditioning System, Juanillo 3BDocument3 pagesBoeing 777 Airconditioning System, Juanillo 3BBENoNo ratings yet
- Amta 329-Cabin Atmosphere Control System Dornier 328-JetDocument2 pagesAmta 329-Cabin Atmosphere Control System Dornier 328-JetBENoNo ratings yet
- Dornier 328 Airconditioning CuencaDocument3 pagesDornier 328 Airconditioning CuencaBENoNo ratings yet
- Boeing 737 Airconditioning System Arcilla Johnmark P Bsaet3b Amta329Document17 pagesBoeing 737 Airconditioning System Arcilla Johnmark P Bsaet3b Amta329BENoNo ratings yet
- B744, En-Route, South China Sea, 2008: Amtp 329 Banaybanay, Bansil, RosarioDocument5 pagesB744, En-Route, South China Sea, 2008: Amtp 329 Banaybanay, Bansil, RosarioBENoNo ratings yet
- Air Conditioning System of Airbus A310Document5 pagesAir Conditioning System of Airbus A310BENoNo ratings yet
- Amta 329 - RilloDocument2 pagesAmta 329 - RilloBENoNo ratings yet
- B744, En-Route, South China Sea, 2008: Amtp 329 Banaybanay BansilDocument5 pagesB744, En-Route, South China Sea, 2008: Amtp 329 Banaybanay BansilBENoNo ratings yet
- Amta329 DC9 Aircon Lava 3BDocument7 pagesAmta329 DC9 Aircon Lava 3BBENoNo ratings yet
- AMTA 329 - Abay-AbayDocument2 pagesAMTA 329 - Abay-AbayBENoNo ratings yet
- Airbus A300 Air Conditioning System - Tandico, Al Rayan (Amta 329)Document3 pagesAirbus A300 Air Conditioning System - Tandico, Al Rayan (Amta 329)BENo0% (1)
- Amta 329 - Arcilla, Ayran, Castillo, SaquidoDocument6 pagesAmta 329 - Arcilla, Ayran, Castillo, SaquidoBENoNo ratings yet
- Amta 329 - MedallaDocument8 pagesAmta 329 - MedallaBENoNo ratings yet
- Aer Lingus Airbus A320-214 El-DVJ, 2015Document9 pagesAer Lingus Airbus A320-214 El-DVJ, 2015BENoNo ratings yet
- Memorandum TO:: Dean/Program Heads Online Instructors College & Shs StudentsDocument2 pagesMemorandum TO:: Dean/Program Heads Online Instructors College & Shs StudentsBENoNo ratings yet
- DML 3535 M1A1 Backdate SBSDocument2 pagesDML 3535 M1A1 Backdate SBSBENoNo ratings yet
- Package Leaflet': January 7, 2021Document66 pagesPackage Leaflet': January 7, 2021BENoNo ratings yet
- Sample Individual AssignmentDocument15 pagesSample Individual AssignmentZainuddin Abu Nasir100% (1)
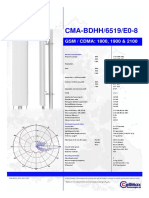
- Cma BDHH 6519 E0-8 PB1Document1 pageCma BDHH 6519 E0-8 PB1planning toolsNo ratings yet
- CTTP 2011 PDFDocument202 pagesCTTP 2011 PDFnavjyoth reddyNo ratings yet
- Dynamics of MachineryDocument49 pagesDynamics of Machinerykumar km0% (1)
- AIP MSSS - Ilopango IntlDocument2 pagesAIP MSSS - Ilopango IntlVicente CastilloNo ratings yet
- Thom Davis, B. J. Tomlinson, Jim Ledbetter (Auth.), R. G. Ross Jr. (Eds.) - Cryocoolers 11-Springer US (2002)Document797 pagesThom Davis, B. J. Tomlinson, Jim Ledbetter (Auth.), R. G. Ross Jr. (Eds.) - Cryocoolers 11-Springer US (2002)peraltajp_20No ratings yet
- Mohrs CircleDocument9 pagesMohrs CircleshrnbolonneNo ratings yet
- Brand Marketing Product Management Product(s) Portfolio: Key PeopleDocument7 pagesBrand Marketing Product Management Product(s) Portfolio: Key Peoplezoee2899No ratings yet
- HW 01 V4Document3 pagesHW 01 V4soulotmagic100% (1)
- FAA ADS-B Program Audit Report 9!11!14Document29 pagesFAA ADS-B Program Audit Report 9!11!14oussama27 fahemNo ratings yet
- Quality Assurance in The Manufacture of Light Unmanned Aircraft SystemDocument4 pagesQuality Assurance in The Manufacture of Light Unmanned Aircraft SystemAhmad Zubair RasulyNo ratings yet
- SyllabusDocument1 pageSyllabusBalajee MechNo ratings yet
- Cover Letter CumminsDocument2 pagesCover Letter CumminsAmeya JalaliNo ratings yet
- Aircraft System SDocument2 pagesAircraft System SPravin HandeNo ratings yet
- Experimental Determination of Dynamic Young's Modulus and Damping of An Aramid-Fabricpolyester Composite MaterialDocument4 pagesExperimental Determination of Dynamic Young's Modulus and Damping of An Aramid-Fabricpolyester Composite MaterialAzeNo ratings yet
- Hidrazina PDFDocument18 pagesHidrazina PDFPedddro96No ratings yet
- Efas and Ifas Air AsiaDocument12 pagesEfas and Ifas Air AsiaAbdul Rasyid Romadhoni33% (3)
- Gutierrez (Review Questions)Document2 pagesGutierrez (Review Questions)Jansen GutierrezNo ratings yet
- FSI Simulation of HALE UAVDocument32 pagesFSI Simulation of HALE UAV783255No ratings yet
- Sect 3. Emergency ProceduresDocument108 pagesSect 3. Emergency ProceduresCarlos ZablahNo ratings yet
- Projectile Motion PDFDocument28 pagesProjectile Motion PDFilyasheee901No ratings yet