You might also like
- Neuro Written II TablesDocument10 pagesNeuro Written II TablesSolomon Seth SallforsNo ratings yet
- Test Questions and Answers Near The End: Direct Force Indirect Force Hearing Loss Ringing Bleed OtalgiaDocument19 pagesTest Questions and Answers Near The End: Direct Force Indirect Force Hearing Loss Ringing Bleed OtalgialeeNo ratings yet
- Fammed Family Life CycleDocument3 pagesFammed Family Life CycleTMC PGI GENER MICKONo ratings yet
- 1.1 - SURG1 - Wound HealingDocument10 pages1.1 - SURG1 - Wound HealingGeriz Daniella VigoNo ratings yet
- (DERMA) 03 TineasDocument9 pages(DERMA) 03 TineasJolaine ValloNo ratings yet
- RADIOLOGY 2.1e Skull FracturesDocument1 pageRADIOLOGY 2.1e Skull FracturesZazaNo ratings yet
- Imaging of The Reproductive SystemDocument15 pagesImaging of The Reproductive SystemAbi SulitNo ratings yet
- Embryology of The EarDocument3 pagesEmbryology of The EarJem MontañaNo ratings yet
- Pathology 5.05b Vagina and Vulva - DR - Dy (Final Edit)Document11 pagesPathology 5.05b Vagina and Vulva - DR - Dy (Final Edit)Dranreb Berylle MasangkayNo ratings yet
- UROLOGY 2020 (Doc BarcenasDocument33 pagesUROLOGY 2020 (Doc BarcenasJüdith Marie Reyes BauntoNo ratings yet
- Current Trends in Management of CholedocholithiasisDocument35 pagesCurrent Trends in Management of Choledocholithiasisrajan kumar100% (6)
- (Basic Surg A) Immunology and TransplantationDocument7 pages(Basic Surg A) Immunology and TransplantationAimie DagaleaNo ratings yet
- Breast Cancer - McMaster Pathophysiology Review PDFDocument8 pagesBreast Cancer - McMaster Pathophysiology Review PDFAprilla Ayu W.No ratings yet
- BURNS - Surgery Trans2Document9 pagesBURNS - Surgery Trans2JAMPTNo ratings yet
- Surgery Trans CheckedDocument5 pagesSurgery Trans CheckedHaloula MINo ratings yet
- Breast CancerDocument4 pagesBreast CancerMaikka IlaganNo ratings yet
- Malignant Thyroid PDFDocument4 pagesMalignant Thyroid PDFOliver QuiambaoNo ratings yet
- Spindle Cell LesionsDocument8 pagesSpindle Cell LesionsdrmanishsharmaNo ratings yet
- The Spleen - A Surgical Perspective: by Col. Abrar Hussain ZaidiDocument43 pagesThe Spleen - A Surgical Perspective: by Col. Abrar Hussain Zaidiabrar_zaidiNo ratings yet
- (Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Document15 pages(Surg 3A) Spleen and Friends-Dr. Segismundo, Dr. Broqueza (Aisle Paler, Joseph Tolentino)Aria Jean MostajoNo ratings yet
- Schwartz 9th Ed: Chapter Outline: The SpleenDocument22 pagesSchwartz 9th Ed: Chapter Outline: The SpleenKathryn Reunilla100% (1)
- ENT Benign Laryngeal DisordersDocument6 pagesENT Benign Laryngeal DisordersLucyellowOttemoesoeNo ratings yet
- Distal To Ligament of Treitz: CausesDocument8 pagesDistal To Ligament of Treitz: CausesKiara GovenderNo ratings yet
- IKD9 - Radiological Evaluation of Renal CystsDocument26 pagesIKD9 - Radiological Evaluation of Renal CystsRenal Association MauritiusNo ratings yet
- ENT Benign Neck MassesDocument2 pagesENT Benign Neck MassesLucyellowOttemoesoeNo ratings yet
- Surgical Oncology and Breast BiopsyDocument12 pagesSurgical Oncology and Breast Biopsybo gum parkNo ratings yet
- Schwartz Hour - BurnDocument62 pagesSchwartz Hour - BurnM3 SURGERY100% (1)
- L7.1 - SURG - Plastic and Reconstructive Surgery (Sep3022)Document4 pagesL7.1 - SURG - Plastic and Reconstructive Surgery (Sep3022)Erald PaderangaNo ratings yet
- Salivary Gland TumorDocument62 pagesSalivary Gland Tumordeepak kumarNo ratings yet
- Basic Emergency Skills in Trauma Part 3 - Penetrating Abdoninal Injury - Dr. Oliver BelarmaDocument3 pagesBasic Emergency Skills in Trauma Part 3 - Penetrating Abdoninal Injury - Dr. Oliver BelarmaRaquel ReyesNo ratings yet
- Approach To Anemia: - Reticulocyte Count Is Most Important TestDocument15 pagesApproach To Anemia: - Reticulocyte Count Is Most Important TestJanella SuerteNo ratings yet
- GYNE 4.01b InfertilityDocument4 pagesGYNE 4.01b InfertilityGray SnellNo ratings yet
- Medicine 6.1b Approach To Cancer Patients - FernandoDocument7 pagesMedicine 6.1b Approach To Cancer Patients - FernandoAbigail LausNo ratings yet
- 4 PEDIA 8 - Bleeding DisordersDocument5 pages4 PEDIA 8 - Bleeding DisordersRainy Liony DuhNo ratings yet
- Oral Cavity PharynxDocument9 pagesOral Cavity PharynxKezia MondonedoNo ratings yet
- GYNE 4.05a Bening Ang Malignant Lesions of The VulvaDocument11 pagesGYNE 4.05a Bening Ang Malignant Lesions of The VulvaGray SnellNo ratings yet
- (RADIO 250) LEC 03 Genitourinary and KUB ImagingDocument7 pages(RADIO 250) LEC 03 Genitourinary and KUB ImagingWilliam PinzonNo ratings yet
- 7 Abdominal TraumaDocument9 pages7 Abdominal TraumaMyrtle Yvonne RagubNo ratings yet
- Surgery QuestionsDocument19 pagesSurgery QuestionsdocaliNo ratings yet
- 3 Surgery - Mediastinum and PleuraDocument6 pages3 Surgery - Mediastinum and PleuraCassey Koi FarmNo ratings yet
- Jaw Tumors: DR - Sudipta Bera PDT 1 Year Plastic and Reconstructive Surgery SSKM & IpgmerDocument28 pagesJaw Tumors: DR - Sudipta Bera PDT 1 Year Plastic and Reconstructive Surgery SSKM & Ipgmerdevinchi09No ratings yet
- Parotid TumorDocument37 pagesParotid TumorRiyan SaputraNo ratings yet
- Schreibman - Bone Tumors in 1 Simple ChartDocument31 pagesSchreibman - Bone Tumors in 1 Simple ChartborstNo ratings yet
- VulvaDocument7 pagesVulvaJose SirittNo ratings yet
- Laryngitis: SpasmDocument13 pagesLaryngitis: Spasm44-Shruti paghdalNo ratings yet
- Eczema, Psoriasis, Cutaneous Infections, Acne, and Other Common Skin DisordersDocument6 pagesEczema, Psoriasis, Cutaneous Infections, Acne, and Other Common Skin DisordersElrey InocianNo ratings yet
- Pitfalls in Diagnosis of HsilDocument1 pagePitfalls in Diagnosis of HsilMaryam ZainalNo ratings yet
- Principles of Management of Soft Tissue SarcomaDocument33 pagesPrinciples of Management of Soft Tissue Sarcomabashiruaminu100% (1)
- Exam OS 214: Nephrology: Lec 08: Pathology of Tubular DiseasesDocument5 pagesExam OS 214: Nephrology: Lec 08: Pathology of Tubular DiseasesKarl Jimenez SeparaNo ratings yet
- (Surg2) 5.2 Urology Part 1 - Dr. YusiDocument18 pages(Surg2) 5.2 Urology Part 1 - Dr. YusiAlloiBialbaNo ratings yet
- Basal Cell Vs SquamousDocument2 pagesBasal Cell Vs SquamousnysNo ratings yet
- (MICROA - 2.1) Myeloid Tissue HistologyDocument6 pages(MICROA - 2.1) Myeloid Tissue HistologyHenryboi CañasNo ratings yet
- Cytology II: Gynae and Non-Gynae CytologyDocument126 pagesCytology II: Gynae and Non-Gynae Cytologybusiness onlyyouNo ratings yet
- Surgery PDFDocument4 pagesSurgery PDFJanine Maita BalicaoNo ratings yet
- (6-7) PATH - Colonic Polyps and CarcinomaDocument11 pages(6-7) PATH - Colonic Polyps and Carcinomaaaron mbindyoNo ratings yet
- Gyne ReflectionDocument18 pagesGyne ReflectionKC Dela RosaNo ratings yet
- Pathology of Common Skin Diseases With Clinical CorrelatesDocument15 pagesPathology of Common Skin Diseases With Clinical CorrelatesAdrien LoNo ratings yet
- GYNE 4.03 Urinary IncontinenceDocument7 pagesGYNE 4.03 Urinary IncontinenceGray SnellNo ratings yet
- TRANS - Pediatric Patient ProblemsDocument4 pagesTRANS - Pediatric Patient ProblemsRencel Hope Bañez100% (1)
- 02 Revman Exercise Caffeine Articles JournalsDocument8 pages02 Revman Exercise Caffeine Articles JournalsKenneth TorresNo ratings yet
- B. Diagram: Predisposing Factors: Precipitating Factors EtiologyDocument3 pagesB. Diagram: Predisposing Factors: Precipitating Factors EtiologyKenneth Torres100% (1)
- Lyme Disease CmapDocument1 pageLyme Disease CmapKenneth TorresNo ratings yet
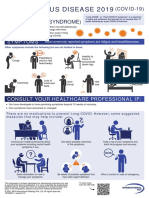
- ISOS - Long-COVID - A3 - Infographic Poster - English - v2Document1 pageISOS - Long-COVID - A3 - Infographic Poster - English - v2Kenneth TorresNo ratings yet
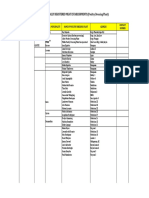
- Updated List of Poultry Dressing PlantDocument2 pagesUpdated List of Poultry Dressing PlantKenneth TorresNo ratings yet
- 2021 SAN BEDA NSIII - SEIZURE and EPILEPSY in Infants and ChildrenDocument57 pages2021 SAN BEDA NSIII - SEIZURE and EPILEPSY in Infants and ChildrenKenneth Torres100% (1)
- AUG 17 TELEMED Physical ExamDocument1 pageAUG 17 TELEMED Physical ExamKenneth TorresNo ratings yet
- 02 Revman Exercise Caffeine Articles JournalsDocument8 pages02 Revman Exercise Caffeine Articles JournalsKenneth TorresNo ratings yet
- 7.1 (LEC) - Functional Anatomy of Respiratory System and Mechanics of BreathingDocument9 pages7.1 (LEC) - Functional Anatomy of Respiratory System and Mechanics of BreathingKenneth TorresNo ratings yet
- 5.05a - Nucleotides - CruzDocument4 pages5.05a - Nucleotides - CruzKenneth TorresNo ratings yet
- Nose and Parasinuses: I. A. B. C. D. E. F. G. II. A. B. C. D. IiiDocument3 pagesNose and Parasinuses: I. A. B. C. D. E. F. G. II. A. B. C. D. IiiKenneth TorresNo ratings yet
- 5.05a - Nucleotides - CruzDocument4 pages5.05a - Nucleotides - CruzKenneth TorresNo ratings yet
- Auditory and Vestibular Apparatus: I. II. Iii. IV. V. VIDocument5 pagesAuditory and Vestibular Apparatus: I. II. Iii. IV. V. VIKenneth TorresNo ratings yet
- (SURG) 6.4 Surgical Metabolism and Nutrition - Dr. CatisDocument7 pages(SURG) 6.4 Surgical Metabolism and Nutrition - Dr. CatisKenneth TorresNo ratings yet
- (SURG) 5.4a Soft Tissue Sarcoma - Dr. RagazaDocument8 pages(SURG) 5.4a Soft Tissue Sarcoma - Dr. RagazaKenneth Torres100% (1)
- Pharynx and Larynx: A. B. C. D. E. F. G. II. A. B. C. D. E. F. G. Iii. IV. VDocument8 pagesPharynx and Larynx: A. B. C. D. E. F. G. II. A. B. C. D. E. F. G. Iii. IV. VKenneth TorresNo ratings yet
- 7.1 (LEC) - Functional Anatomy of Respiratory System and Mechanics of BreathingDocument9 pages7.1 (LEC) - Functional Anatomy of Respiratory System and Mechanics of BreathingKenneth TorresNo ratings yet
- Anat Lec 06 PDFDocument8 pagesAnat Lec 06 PDFKenneth TorresNo ratings yet
- FE 5 Part 2 of 2 PDFDocument12 pagesFE 5 Part 2 of 2 PDFKenneth TorresNo ratings yet
- Examination of Mental Status and Higher Cerebral FunctionsDocument9 pagesExamination of Mental Status and Higher Cerebral Functionsriczen vilaNo ratings yet
- Osce Cranial Nerves PDFDocument42 pagesOsce Cranial Nerves PDFriczen vilaNo ratings yet
- (Surg) - 1.3 Fluid and Electrolyte (Updated) . - Dr. Catis PDFDocument11 pages(Surg) - 1.3 Fluid and Electrolyte (Updated) . - Dr. Catis PDFKenneth TorresNo ratings yet
- FE 5 Part 2 of 2 PDFDocument12 pagesFE 5 Part 2 of 2 PDFKenneth TorresNo ratings yet
- OppDocument48 pagesOppDEDY100% (2)
- 1 Prescription FinalDocument62 pages1 Prescription FinalDonzzkie DonNo ratings yet
- EncephaloceleDocument24 pagesEncephaloceledepan_dkb32No ratings yet
- ABG Made EasyDocument10 pagesABG Made EasyMayer Rosenberg100% (38)
- AdvocacyDocument3 pagesAdvocacyGc Borres100% (2)
- Anticoagulants 161120143945Document29 pagesAnticoagulants 161120143945Roshan SahuNo ratings yet
- Assessment of Tumor Response To Percutaneous Ablation by Using Glyceraldehyde-3-Phosphate Dehydrogenase AntagonistsDocument12 pagesAssessment of Tumor Response To Percutaneous Ablation by Using Glyceraldehyde-3-Phosphate Dehydrogenase Antagonistsnguyen hoang nganNo ratings yet
- School Based Pei Program Logic Model ExampleDocument3 pagesSchool Based Pei Program Logic Model Exampleapi-410743934No ratings yet
- Clinical Manifestations and Diagnosis of Acute Pancreatitis PDFDocument32 pagesClinical Manifestations and Diagnosis of Acute Pancreatitis PDFChumas VidalNo ratings yet
- MoringaDocument14 pagesMoringaAnonymous 6Ych0RXi7100% (1)
- Understanding Narcisistic PersonalityDocument11 pagesUnderstanding Narcisistic PersonalityCarla RiveraNo ratings yet
- Edamame InfoDocument4 pagesEdamame InfoFredericYudhistiraDharmawataNo ratings yet
- Acute Intestinal ObstructionDocument38 pagesAcute Intestinal ObstructiondinahzrNo ratings yet
- Small IntestineDocument2 pagesSmall Intestineiron100% (1)
- Active Living: January 2017Document20 pagesActive Living: January 2017mgruender1No ratings yet
- Manual of Management DH, PU and RHDocument166 pagesManual of Management DH, PU and RHarunikalNo ratings yet
- Catgut Chromic Gauge 2 0 4-0-75 CM On 15 MM 1 2 Circle Round BodiedDocument3 pagesCatgut Chromic Gauge 2 0 4-0-75 CM On 15 MM 1 2 Circle Round BodiedEffort Welday HoppingNo ratings yet
- CHPPM How To Write and Exercise PrescriptionDocument160 pagesCHPPM How To Write and Exercise PrescriptionJackie NepomucenoNo ratings yet
- Highlights For 2019 Taiwan-Korea Young Stroke Investigator Joint SymposiumDocument3 pagesHighlights For 2019 Taiwan-Korea Young Stroke Investigator Joint Symposium台灣中風醫誌No ratings yet
- DafpusDocument3 pagesDafpusAbdi BencanaNo ratings yet
- SagarDocument10 pagesSagarSagar PardeshiNo ratings yet
- Guselkumab in Psoriatic ArthritisDocument12 pagesGuselkumab in Psoriatic ArthritisMr. LNo ratings yet
- Sample Questions For HAAD, Prometric and DHA For NursesDocument23 pagesSample Questions For HAAD, Prometric and DHA For Nurseskichoo185% (97)
- From GROW To GROUP Theoretical Issues and A Practical Model For Group Coaching in OrganisationsDocument17 pagesFrom GROW To GROUP Theoretical Issues and A Practical Model For Group Coaching in OrganisationsMardhiah RamlanNo ratings yet
- Munro 2007Document17 pagesMunro 2007Jose RodriguezNo ratings yet
- What Is OCDDocument2 pagesWhat Is OCDshiviNo ratings yet
- Epidemiology of Skin DiseasesDocument33 pagesEpidemiology of Skin DiseasesMahmoud AbuAwadNo ratings yet
- MicDocument75 pagesMicUwizeye HerouNo ratings yet
- ASEAN Manual of Food Analysis PDFDocument196 pagesASEAN Manual of Food Analysis PDFCristina PlesaNo ratings yet
- Splinting For The Prevention Correction of Contractures in Adults With Neurological Dysfunction Quick ReferDocument12 pagesSplinting For The Prevention Correction of Contractures in Adults With Neurological Dysfunction Quick ReferDaniel MarvasoNo ratings yet