You might also like
- Nursing 212 Medical - Surgical Nursing 1 PDFDocument178 pagesNursing 212 Medical - Surgical Nursing 1 PDFzarka wahid buxNo ratings yet
- Pharmacology and The Nursing ProcessDocument28 pagesPharmacology and The Nursing ProcessEdralyn MatalangNo ratings yet
- Google Doc - Mark K NCLEX Study GuideDocument62 pagesGoogle Doc - Mark K NCLEX Study Guideezinne obinna-umaNo ratings yet
- Pedia Prevous Board Questions PDFDocument103 pagesPedia Prevous Board Questions PDFJulius Matthew LuzanaNo ratings yet
- AaDocument5 pagesAaYusril Marhaen100% (1)
- EndocrineDocument23 pagesEndocrinensvickneswaranNo ratings yet
- EndocrinologyDocument46 pagesEndocrinology[161]Shuaib AktherNo ratings yet
- Dermatology Images (All in One Merged)Document692 pagesDermatology Images (All in One Merged)Woo Rin Park100% (2)
- LeukemiasDocument8 pagesLeukemiasharideepNo ratings yet
- Pharma Review NotesDocument9 pagesPharma Review NotesYves100% (1)
- 8.male Genitourinary CancersDocument7 pages8.male Genitourinary CancersWoo Rin ParkNo ratings yet
- Lower Respiratory Tract InfectionsDocument8 pagesLower Respiratory Tract InfectionsHappy Peachy AilenNo ratings yet
- A Visual Guide To ECG Interpretation 2e 40 Jan 1 2017 41 40 1496321537 41 40 LWW 41Document1,578 pagesA Visual Guide To ECG Interpretation 2e 40 Jan 1 2017 41 40 1496321537 41 40 LWW 41xtineNo ratings yet
- Intrahepatic Cholestasis of Pregnancy: Clinical Obstetrics and Gynecology Volume 63, Number 1, 134-151Document19 pagesIntrahepatic Cholestasis of Pregnancy: Clinical Obstetrics and Gynecology Volume 63, Number 1, 134-151Von BernalNo ratings yet
- Diagnostic Tests PDFDocument2 pagesDiagnostic Tests PDFBenedict AlvarezNo ratings yet
- Pathophysiology Notes: - Glomerulus - Proximal Convoluted TubuleDocument14 pagesPathophysiology Notes: - Glomerulus - Proximal Convoluted TubuleHaifa ibrahimNo ratings yet
- Mythos World Resources Vol 1Document20 pagesMythos World Resources Vol 1Dániel Sebestyén100% (1)
- Maternity Antepartum Genetic TestingDocument21 pagesMaternity Antepartum Genetic TestingBobbie N Melinda RussellNo ratings yet
- NCM 112 Study Guide MidtermDocument42 pagesNCM 112 Study Guide MidtermMark Nathaniel ValerioNo ratings yet
- Peripheral Vascular Disease-1Document52 pagesPeripheral Vascular Disease-1Johiarra Madanglog Tabigne100% (1)
- MEdical Surgical REVEWERDocument86 pagesMEdical Surgical REVEWERennaedNo ratings yet
- Psycho PharmaDocument8 pagesPsycho PharmaMark JosephNo ratings yet
- NCLEX Practice Exam For Pediatric Nursing 1: Start StartDocument9 pagesNCLEX Practice Exam For Pediatric Nursing 1: Start StartLot RositNo ratings yet
- 4 Series CPTDocument13 pages4 Series CPTPraviiNo ratings yet
- Nursing CS CroupDocument1 pageNursing CS Croupreuben kadarajaNo ratings yet
- Goulds Pathophysiology For The Health Professions 6th Edition Vanmeter Test BankDocument8 pagesGoulds Pathophysiology For The Health Professions 6th Edition Vanmeter Test BankJessicaHardysrbxd100% (11)
- Maternity Nursing 2Document133 pagesMaternity Nursing 2Rick100% (1)
- Universally Accepted AbbreviationsDocument4 pagesUniversally Accepted AbbreviationsPamela Dela Cerna BrionesNo ratings yet
- 01 Intro Pcol-MergedDocument19 pages01 Intro Pcol-MergedlumpiaNo ratings yet
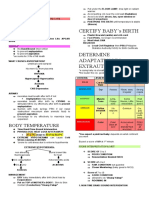
- Certify Baby'S Birth: Body TemperatureDocument9 pagesCertify Baby'S Birth: Body TemperatureJobelle Acena100% (1)
- UntitledDocument6 pagesUntitledFritz Angelo BullonNo ratings yet
- Human Papillomavirus (HPV) : Evann R. Casoy, RN Nurse Deployment ProjectDocument19 pagesHuman Papillomavirus (HPV) : Evann R. Casoy, RN Nurse Deployment ProjectEva CastuloNo ratings yet
- Musculoskeletal-System NLE ReviewDocument124 pagesMusculoskeletal-System NLE ReviewRitamaria0% (1)
- Clinical Features of Renal DiseaseDocument80 pagesClinical Features of Renal DiseaseIdiAmadouNo ratings yet
- Disorders of The Reproductive SystemDocument10 pagesDisorders of The Reproductive SystemRose Kathreen Quintans AuxteroNo ratings yet
- 9 ECG Strips On The NCLEX: 1. Normal Sinus RhythmDocument4 pages9 ECG Strips On The NCLEX: 1. Normal Sinus RhythmH T (Ah Ki)No ratings yet
- 4a's LESSON PLAN FOR GRADE 8 - HealthDocument2 pages4a's LESSON PLAN FOR GRADE 8 - HealthDremie Works100% (1)
- Schizophrenia and Psychotic DisordersDocument6 pagesSchizophrenia and Psychotic DisordersfededelveliNo ratings yet
- Sleep and Sleep-Wake DisordersDocument5 pagesSleep and Sleep-Wake DisordersfededelveliNo ratings yet
- Study Questions Answered by Sir Charles MCDocument13 pagesStudy Questions Answered by Sir Charles MCTakudzwa ChirumeNo ratings yet
- Medical Terms in Lay Language2Document7 pagesMedical Terms in Lay Language2Mavra zNo ratings yet
- Normal Laboratory Values With Nursing Consideration - UsnganDocument8 pagesNormal Laboratory Values With Nursing Consideration - UsnganPrincess Nasima M. UsnganNo ratings yet
- CHP 66 Common Problems of Critical Care PatientsDocument18 pagesCHP 66 Common Problems of Critical Care Patientshops23No ratings yet
- Notes: Amyotrophic Lateral Sclerosis (Als)Document6 pagesNotes: Amyotrophic Lateral Sclerosis (Als)H SHABANANo ratings yet
- HeartFailure Nursing FIK 2014Document101 pagesHeartFailure Nursing FIK 2014Putri NurlaeliNo ratings yet
- 1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingDocument14 pages1st Lecture (NCM106 ABC I) Care of Clients in Cellular Aberrations, ABC, Emergency and Disaster NursingKamx Mohammed100% (1)
- Pharmacology - Section 23 - Antibiotics 2Document5 pagesPharmacology - Section 23 - Antibiotics 2Pathalee ThalpavilaNo ratings yet
- Hema2 Lec PrefinalDocument9 pagesHema2 Lec Prefinallai cruzNo ratings yet
- Fmge De'C. 2017Document21 pagesFmge De'C. 2017Subhodeep MondalNo ratings yet
- Nyeri KepalaDocument6 pagesNyeri KepalaAydhing Nathasya JapNo ratings yet
- Sexually Transmitted DiseasesDocument5 pagesSexually Transmitted Diseasesreghpineda28No ratings yet
- NCM 212 - Pharmacokinetics and PharmacodynamicsDocument11 pagesNCM 212 - Pharmacokinetics and PharmacodynamicsLYRIZZA LEA BHEA DESIATANo ratings yet
- Anatomy Reproductive SystemDocument8 pagesAnatomy Reproductive SystemjisooNo ratings yet
- Medical Surgical Nursing - LectureDocument77 pagesMedical Surgical Nursing - LecturePink Majaila GludoNo ratings yet
- Approach To Unconscious PatientDocument23 pagesApproach To Unconscious Patienttantw880% (1)
- Urinary System DisordersDocument14 pagesUrinary System DisordersGideon P. CasasNo ratings yet
- Pharmacology: General Anaesthetic AgentsDocument65 pagesPharmacology: General Anaesthetic AgentsSharifa DarayanNo ratings yet
- Pre Hos TraumaDocument11 pagesPre Hos TraumaGel OmugtongNo ratings yet
- 1538 Exam 4 Cell Reg & GriefDocument35 pages1538 Exam 4 Cell Reg & GriefJade EdanoNo ratings yet
- Ncm104 10th CD IIDocument20 pagesNcm104 10th CD IIKamx MohammedNo ratings yet
- 2011 Understanding Pharmacology Essentials For Medication SafetyDocument1 page2011 Understanding Pharmacology Essentials For Medication SafetygloriyaNo ratings yet
- Thorax and LungsDocument2 pagesThorax and LungsHNo ratings yet
- NP1 BulletsDocument17 pagesNP1 BulletsJea VesagasNo ratings yet
- NICU Cheat SheetDocument4 pagesNICU Cheat SheetRichelle FrondaNo ratings yet
- 7.2 Patho6 - Cns Infection 2015bDocument8 pages7.2 Patho6 - Cns Infection 2015bMiguel Cuevas Dolot100% (1)
- Inflammatory Bowel DiseaseDocument8 pagesInflammatory Bowel Diseasevmc6gyvh9gNo ratings yet
- Notes: Chlamydia Species (Pneumonia)Document3 pagesNotes: Chlamydia Species (Pneumonia)Woo Rin ParkNo ratings yet
- Key Messages:: Easures For Supporting Domestic Markets During The Ovid Outbreak in FricaDocument6 pagesKey Messages:: Easures For Supporting Domestic Markets During The Ovid Outbreak in FricaWoo Rin ParkNo ratings yet
- Guidelines For Controlled Trials of Drugs in Migraine: Second EditionDocument22 pagesGuidelines For Controlled Trials of Drugs in Migraine: Second EditionWoo Rin ParkNo ratings yet
- Arena VirusesDocument2 pagesArena VirusesWoo Rin ParkNo ratings yet
- Notes: Chlamydia Species (Pneumonia)Document3 pagesNotes: Chlamydia Species (Pneumonia)Woo Rin ParkNo ratings yet
- ArenaviridaeDocument2 pagesArenaviridaeWoo Rin ParkNo ratings yet
- Comparative Efficacy and Safety of Urate-Lowering Therapy For The Treatment of Hyperuricemia: A Systematic Review and Network Meta-AnalysisDocument13 pagesComparative Efficacy and Safety of Urate-Lowering Therapy For The Treatment of Hyperuricemia: A Systematic Review and Network Meta-AnalysisWoo Rin ParkNo ratings yet
- 159 - Clinical Trials Chronic Migraine ChaDocument12 pages159 - Clinical Trials Chronic Migraine ChaWoo Rin ParkNo ratings yet
- Trematodes (Flatworms)Document6 pagesTrematodes (Flatworms)Woo Rin ParkNo ratings yet
- Guidelines For Controlled Trials of Drugs in Migraine: Third Edition. A Guide For InvestigatorsDocument33 pagesGuidelines For Controlled Trials of Drugs in Migraine: Third Edition. A Guide For InvestigatorsWoo Rin ParkNo ratings yet
- 157 - Clinical Trials Adverse Events ChaDocument6 pages157 - Clinical Trials Adverse Events ChaWoo Rin ParkNo ratings yet
- Streptococcus Agalactiae (Group B Strep) : NotesDocument6 pagesStreptococcus Agalactiae (Group B Strep) : NotesWoo Rin ParkNo ratings yet
- Notes: Eastern Equine Encephalitis Virus (Eeev)Document5 pagesNotes: Eastern Equine Encephalitis Virus (Eeev)Woo Rin ParkNo ratings yet
- Systemic MycosesDocument7 pagesSystemic MycosesWoo Rin ParkNo ratings yet
- Mid Islam Dan Budaya Tapanuli: D I S U S U N Oleh: NURINDAH NASUTION (17 401 00255)Document9 pagesMid Islam Dan Budaya Tapanuli: D I S U S U N Oleh: NURINDAH NASUTION (17 401 00255)Woo Rin ParkNo ratings yet
- Notes: Trypanosoma BruceiDocument5 pagesNotes: Trypanosoma BruceiWoo Rin ParkNo ratings yet
- 10.disorders of LaborDocument8 pages10.disorders of LaborWoo Rin ParkNo ratings yet
- Tricho MonaDocument2 pagesTricho MonaWoo Rin ParkNo ratings yet
- Mid Islam Dan Budaya Tapanuli: D I S U S U N Oleh: Nurindah Nasution (17 401 00255)Document9 pagesMid Islam Dan Budaya Tapanuli: D I S U S U N Oleh: Nurindah Nasution (17 401 00255)Woo Rin ParkNo ratings yet
- Coronaryarterydisease: Diagnosis and ManagementDocument17 pagesCoronaryarterydisease: Diagnosis and ManagementWoo Rin ParkNo ratings yet
- Malignant TumorsDocument8 pagesMalignant TumorsWoo Rin ParkNo ratings yet
- Hair-Related DiseasesDocument3 pagesHair-Related DiseasesWoo Rin ParkNo ratings yet
- Papulosquamous DisordersDocument6 pagesPapulosquamous DisordersWoo Rin ParkNo ratings yet
- Vesiculobullous DiseasesDocument4 pagesVesiculobullous DiseasesWoo Rin ParkNo ratings yet
- Urticaria and ErythemaDocument5 pagesUrticaria and ErythemaWoo Rin ParkNo ratings yet
- Pigmentation DisordersDocument5 pagesPigmentation DisordersWoo Rin ParkNo ratings yet
- Dermatitis and EczemaDocument6 pagesDermatitis and EczemaWoo Rin ParkNo ratings yet
- Inflammatory Bowel Disease: Ruchita BhavsarDocument34 pagesInflammatory Bowel Disease: Ruchita BhavsarShinta MayasariNo ratings yet
- Hypertensive Disorders in Pregnancy: Abdallah Al-MawazrehDocument36 pagesHypertensive Disorders in Pregnancy: Abdallah Al-MawazrehAbdallahMousaNo ratings yet
- Coping With Diabetes-Denial, AngerDocument13 pagesCoping With Diabetes-Denial, AngerShwetal ShindeNo ratings yet
- Pe103-Course-Guide-And-Module-Sem. 2022-2023Document55 pagesPe103-Course-Guide-And-Module-Sem. 2022-2023Thomas Danjo ManulatNo ratings yet
- Nursing Care Plan For A Person With Croup Nursing DiagnosisDocument2 pagesNursing Care Plan For A Person With Croup Nursing DiagnosisMonica Rivera100% (1)
- Gcse Mock TestsDocument5 pagesGcse Mock TestsTrung Tran VanNo ratings yet
- 03-Personal Hygiene Practices & Entry ProcedureDocument2 pages03-Personal Hygiene Practices & Entry ProcedurekitekNo ratings yet
- Boone 19e c04 PPTDocument40 pagesBoone 19e c04 PPTJohn RitssNo ratings yet
- 4217 - First Aid and Safety EducationDocument6 pages4217 - First Aid and Safety EducationSalahuddeen AbubakarNo ratings yet
- Pulsatile Drug Delivery System: BY C.V. Saikrishna Reddy M.Pharm I Year JJ College of PharmacyDocument20 pagesPulsatile Drug Delivery System: BY C.V. Saikrishna Reddy M.Pharm I Year JJ College of PharmacyAakash SahaNo ratings yet
- Dengue Fever: University of Southern Philippines Foundation Salinas Drive, Lahug, Cebu City College of NursingDocument5 pagesDengue Fever: University of Southern Philippines Foundation Salinas Drive, Lahug, Cebu City College of NursingJayson OlileNo ratings yet
- Medicine Ophthalmology Slide14Document4 pagesMedicine Ophthalmology Slide14testNo ratings yet
- Health Sector Reform in IndiaDocument21 pagesHealth Sector Reform in Indiajouhar21No ratings yet
- Primary Surgery - AbscessDocument14 pagesPrimary Surgery - Abscessjackblack2001100% (1)
- Covid 19 Pandemic With KeyDocument2 pagesCovid 19 Pandemic With KeyNan LibraNo ratings yet
- News Bulletin Script TemplateDocument2 pagesNews Bulletin Script TemplateSantisha Chattergoon100% (3)
- dotAIO V2 LiteDocument1 pagedotAIO V2 LiteStevanusNo ratings yet
- Abnormal Psychology: Historical and Modern Perspectives: Total Assessment Guide (T.A.G.)Document29 pagesAbnormal Psychology: Historical and Modern Perspectives: Total Assessment Guide (T.A.G.)Rachelle SalcedoNo ratings yet
- Renal 20nutrition 20web 1Document57 pagesRenal 20nutrition 20web 1Qurat ul Ain Arif Sethi Pharmacy PracticeNo ratings yet
- Cardiology-5 DysrhythmiaDocument16 pagesCardiology-5 DysrhythmiaMahmoud RamadanNo ratings yet
- Preanesthetic Assessment of Cardiac Patients UndDocument42 pagesPreanesthetic Assessment of Cardiac Patients UndParvathy R NairNo ratings yet
- Case 76Document3 pagesCase 76Yelrebmik OdranrebNo ratings yet