You might also like
- The Effects of Depression On The Student's Academic Performances in STI Baliuag and Ways How To Cope With ItDocument18 pagesThe Effects of Depression On The Student's Academic Performances in STI Baliuag and Ways How To Cope With Itarisu100% (1)
- Thesis - EnglishDocument17 pagesThesis - EnglishKyle Cayaban100% (1)
- Depression Among College StudentsDocument17 pagesDepression Among College StudentsEqui TinNo ratings yet
- Review of Related Literature and StudiesDocument19 pagesReview of Related Literature and StudiesElla Austral AsokNo ratings yet
- Research ProposalDocument14 pagesResearch ProposalMergina MontañoNo ratings yet
- Depression ResearchDocument12 pagesDepression ResearchIsaiah Diunne Magat Semilla50% (2)
- Depression in StudentsDocument20 pagesDepression in StudentsIñaki Zuriel ConstantinoNo ratings yet
- Research Proposal Ir IDocument3 pagesResearch Proposal Ir Iapi-421413167No ratings yet
- How Senior High School Students of DNHS Handle Academic Depression During This PandemicDocument22 pagesHow Senior High School Students of DNHS Handle Academic Depression During This PandemicFlaky JamNo ratings yet
- BBDocument7 pagesBBmomo connor100% (1)
- Of Coping Mechanisms and Psychosocial Perspective of Teenage Mothers" Is ConductedDocument50 pagesOf Coping Mechanisms and Psychosocial Perspective of Teenage Mothers" Is ConductedKim100% (1)
- Final Report The Impact of Social Media On Mental Health and Emotional PDFDocument41 pagesFinal Report The Impact of Social Media On Mental Health and Emotional PDFMikhail LandichoNo ratings yet
- Glossophobia: An Assessment On Prevalence of Public Speaking Anxiety Among Student-Teachers of University of Cagayan ValleyDocument3 pagesGlossophobia: An Assessment On Prevalence of Public Speaking Anxiety Among Student-Teachers of University of Cagayan ValleyTobyNo ratings yet
- Term PaperDocument27 pagesTerm PaperKimberly MilaranNo ratings yet
- The Relationship of Mental Health and Academic Performance of College StudentsDocument5 pagesThe Relationship of Mental Health and Academic Performance of College StudentsLpc Geremy Impas OwelNo ratings yet
- A Thesis For DepressionDocument64 pagesA Thesis For Depressioncharlie besabellaNo ratings yet
- Anxiety Disorder Case StudiesDocument2 pagesAnxiety Disorder Case Studiescoleenllb_usa100% (1)
- Teenage DepressionDocument17 pagesTeenage Depressionvaaleentiinee85% (52)
- Mental HealthDocument15 pagesMental HealthFlaviah Kamanda100% (1)
- Related LiteratureDocument5 pagesRelated Literaturemsrch june0% (1)
- Personal Report of Public Speaking Anxiety (PRPSA)Document3 pagesPersonal Report of Public Speaking Anxiety (PRPSA)AHMED KHAN100% (1)
- The Problem and Its BackgroundDocument7 pagesThe Problem and Its BackgroundFrizie Jane Sacasac MagbualNo ratings yet
- The Impact of The COVID-19 Pandemic On Suicide Rates. QJMDocument17 pagesThe Impact of The COVID-19 Pandemic On Suicide Rates. QJMJose Fernando Díez ConchaNo ratings yet
- Factors that Cause Depression and Impact School Performance in Grade 10 StudentsDocument9 pagesFactors that Cause Depression and Impact School Performance in Grade 10 StudentsAimee HernandezNo ratings yet
- Impact of Mental Health on Students' Academic PerformanceDocument11 pagesImpact of Mental Health on Students' Academic PerformanceChristian VillaNo ratings yet
- Ped 121Document171 pagesPed 121Selenai SelenaiNo ratings yet
- Student Burnout - Peer ReviewedDocument14 pagesStudent Burnout - Peer ReviewedPyrex100% (1)
- Chapter IDocument38 pagesChapter IKhristal ChaeNo ratings yet
- Depression and Anxiety Among Medical StudentsDocument6 pagesDepression and Anxiety Among Medical StudentsAlejandro MartinezNo ratings yet
- Mental Health in The Pandemic TimesDocument13 pagesMental Health in The Pandemic TimesShubhanshu Dhakal100% (1)
- Factors Affecting Students' Academic PerformanceDocument62 pagesFactors Affecting Students' Academic PerformanceRheeanne Mae AmilasanNo ratings yet
- Pr2 (Chapter 2)Document5 pagesPr2 (Chapter 2)Marj CabasagNo ratings yet
- The Effects of Anxiety and Depression in The Academic Performance of The Grade 12 STEM Students in Sta. Lucia High School S.Y. 2021 2022 STEM 3Document7 pagesThe Effects of Anxiety and Depression in The Academic Performance of The Grade 12 STEM Students in Sta. Lucia High School S.Y. 2021 2022 STEM 3Criscel Danica Sabater100% (1)
- An Assessment On The Level of Anxiety and Depression Among Millennials On Covid-19 Crisis: Basis For The Development of Online Mental Health SupportDocument36 pagesAn Assessment On The Level of Anxiety and Depression Among Millennials On Covid-19 Crisis: Basis For The Development of Online Mental Health SupportJ Patrick Lorenzo100% (1)
- Students' Level of Metacognitive Awareness As Correlates of Their Mathematics AchievementDocument8 pagesStudents' Level of Metacognitive Awareness As Correlates of Their Mathematics AchievementPsychology and Education: A Multidisciplinary JournalNo ratings yet
- The Influence of Facebook Use On Body ImDocument34 pagesThe Influence of Facebook Use On Body ImDivina Gracia De VeraNo ratings yet
- RRL Facebook and Self EsteemDocument7 pagesRRL Facebook and Self EsteemViola Hastings0% (1)
- The Impacts of Pandemic Lockdown To The Mental Health of Grade 12 Gas Students in CNH - Chap 2Document17 pagesThe Impacts of Pandemic Lockdown To The Mental Health of Grade 12 Gas Students in CNH - Chap 2Gerryanna MagbitangNo ratings yet
- Teenage DepressionDocument9 pagesTeenage DepressionMacie Deocampo EstuyaNo ratings yet
- Mental Health Awareness Is An Important Issue For All EducatorsDocument5 pagesMental Health Awareness Is An Important Issue For All Educatorsroneldayo62No ratings yet
- Impact of Social Media On Body Image and Self-Esteem Among Young Filipino Men and WomenDocument9 pagesImpact of Social Media On Body Image and Self-Esteem Among Young Filipino Men and WomenGianne Lalosa TebelinNo ratings yet
- Fatima, the War Nurse: Stories of Courage and CompassionDocument8 pagesFatima, the War Nurse: Stories of Courage and CompassionnicoleNo ratings yet
- Depression Treatment StrategiesDocument8 pagesDepression Treatment StrategiesFayasulhusain MuthalibNo ratings yet
- Stress Management's Impact on 4th Year Students' Academic SuccessDocument11 pagesStress Management's Impact on 4th Year Students' Academic SuccessErwin llabonNo ratings yet
- Practical Research (Qualitative) : THE IMPACT OF DISTANCE LEARNING ON THE MENTAL HEALTH OF GRADE 10 STUDENTS OF SAINT MARY'S ACADEMY IN AGOO, S.Y. 2020-2021Document14 pagesPractical Research (Qualitative) : THE IMPACT OF DISTANCE LEARNING ON THE MENTAL HEALTH OF GRADE 10 STUDENTS OF SAINT MARY'S ACADEMY IN AGOO, S.Y. 2020-2021Angella Mae Favia GamboaNo ratings yet
- Stressors and Coping Mechanisms of Psychologically Distressed MSU-IIT StudentsDocument22 pagesStressors and Coping Mechanisms of Psychologically Distressed MSU-IIT StudentsDarleen Rizel CalumbaNo ratings yet
- Domingo, John Paul CDocument4 pagesDomingo, John Paul CRyuko27No ratings yet
- Bullying Among Grade 10 Students in Tarlac National High SchoolDocument28 pagesBullying Among Grade 10 Students in Tarlac National High SchoolJuleta TipayNo ratings yet
- Factors Affecting Junior High School StudentsDocument49 pagesFactors Affecting Junior High School StudentsJardiolyn IbaleNo ratings yet
- Effect of Online Learning To Mental Health of Grade 12 H.E. Students in GIST Cogeo BranchDocument1 pageEffect of Online Learning To Mental Health of Grade 12 H.E. Students in GIST Cogeo BranchZach ChukachucksNo ratings yet
- The Mental Status ExaminationDocument16 pagesThe Mental Status Examinationeloisa.abcedeNo ratings yet
- Quantitative Research: Relationship Between Self Confidence and Academic Productivity of Senior High School Students at Pinamukan Integrated SchoolDocument11 pagesQuantitative Research: Relationship Between Self Confidence and Academic Productivity of Senior High School Students at Pinamukan Integrated SchoolAntonnette PagsinohinNo ratings yet
- Effects of social media, verbal abuse, and cleanliness on student performanceDocument4 pagesEffects of social media, verbal abuse, and cleanliness on student performancejake doinogNo ratings yet
- Thesis BodyDocument13 pagesThesis Bodyreginexanthe100% (1)
- The Effect of Social Media On TeenagersDocument3 pagesThe Effect of Social Media On TeenagersKarol Sanchez100% (1)
- Bullying in SchoolsDocument8 pagesBullying in Schoolssaras qt0% (1)
- Reaction Paper 1 - Autism PsychologyDocument4 pagesReaction Paper 1 - Autism Psychologyapi-306687159No ratings yet
- JCC Academy Students' Academic Performance Before and During Online ClassesDocument39 pagesJCC Academy Students' Academic Performance Before and During Online ClassesJOHN GLAUBEN J. CADUANNo ratings yet
- Asian Institute of Computer StudiesDocument9 pagesAsian Institute of Computer StudiesBoss OralcNo ratings yet
- Tapos Na PaghihirapDocument41 pagesTapos Na Paghihirapharreh hotdoggssNo ratings yet
- Group 9 EnglishDocument35 pagesGroup 9 EnglishKimberly NgNo ratings yet
- Summary of Academic and CoDocument1 pageSummary of Academic and CoKimberly NgNo ratings yet
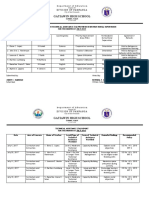
- Department of Education: Month: NOVEMBERDocument2 pagesDepartment of Education: Month: NOVEMBERKimberly NgNo ratings yet
- Number of Vaccinated Students Grade Level and SectionDocument1 pageNumber of Vaccinated Students Grade Level and SectionKimberly NgNo ratings yet
- Gatiawin High School: Division of PampangaDocument3 pagesGatiawin High School: Division of PampangaKimberly NgNo ratings yet
- Ways On How Teenagers Cope Up With Thenegative Effects of Social MediaDocument16 pagesWays On How Teenagers Cope Up With Thenegative Effects of Social MediaKimberly NgNo ratings yet
- Archivetempattack On Titan - PremiumDocument9 pagesArchivetempattack On Titan - PremiumKimberly NgNo ratings yet
- What Is Review Related Literature?Document17 pagesWhat Is Review Related Literature?Kimberly NgNo ratings yet
- Group 6 10 - IsaiahDocument10 pagesGroup 6 10 - IsaiahKimberly NgNo ratings yet
- Department of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Document4 pagesDepartment of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Kimberly NgNo ratings yet
- Research AddictionDocument6 pagesResearch AddictionKimberly NgNo ratings yet
- Baby Thesis For English 10Document31 pagesBaby Thesis For English 10Kimberly NgNo ratings yet
- 3RD Quarter Grade 8 PeDocument11 pages3RD Quarter Grade 8 PeKath Leen100% (3)
- Music 8: Guided Learning Activity SheetsDocument17 pagesMusic 8: Guided Learning Activity SheetsDonalyn Veruela Abon100% (1)
- Department of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Document4 pagesDepartment of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Kimberly NgNo ratings yet
- Department of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Document4 pagesDepartment of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Kimberly NgNo ratings yet
- Department of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Document5 pagesDepartment of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Kimberly NgNo ratings yet
- Group 1 EnglishDocument9 pagesGroup 1 EnglishKimberly NgNo ratings yet
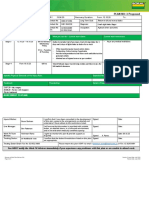
- Weekly ESP Home Learning PlanDocument4 pagesWeekly ESP Home Learning PlanKimberly NgNo ratings yet
- Department of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Document5 pagesDepartment of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Kimberly NgNo ratings yet
- Department of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Document4 pagesDepartment of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Kimberly NgNo ratings yet
- Department of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Document4 pagesDepartment of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Kimberly NgNo ratings yet
- JoshuaDocument18 pagesJoshuaKimberly NgNo ratings yet
- Department of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Document4 pagesDepartment of Education: Name: Jemilyn P. Dela Cruz Grade Level: Grade 10 Learning Area: ESP 10Kimberly NgNo ratings yet
- Writing The Research Conclusion: GroupDocument13 pagesWriting The Research Conclusion: GroupKimberly NgNo ratings yet
- Weekly ESP Home Learning PlanDocument4 pagesWeekly ESP Home Learning PlanKimberly NgNo ratings yet
- Practicum Portfolio: LDM 2 Course FORDocument20 pagesPracticum Portfolio: LDM 2 Course FORKimberly NgNo ratings yet
- Practicum Portfolio - Airish Joan GatusDocument16 pagesPracticum Portfolio - Airish Joan GatusKimberly NgNo ratings yet
- Department of Education: Summative Test in Music 8Document2 pagesDepartment of Education: Summative Test in Music 8Kimberly NgNo ratings yet
- Pain Dr. HenryDocument36 pagesPain Dr. Henryreagan setiawanNo ratings yet
- Pharmacy Practice National Seminar BrochureDocument4 pagesPharmacy Practice National Seminar BrochureWajid KNo ratings yet
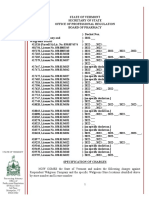
- Walgreens Specification of ChargesDocument40 pagesWalgreens Specification of ChargesMichael Cusanelli100% (2)
- Epidemic and Pandemic Differences Additional InformationDocument4 pagesEpidemic and Pandemic Differences Additional InformationPsyZeroNo ratings yet
- Scope of Nursing CareersDocument33 pagesScope of Nursing Careersmaria jacobNo ratings yet
- FIP Cat TreatmentDocument14 pagesFIP Cat TreatmentRaihanNo ratings yet
- Sai Kiran Hospital & Kiran Infertility Center PVT - LTD - DR Samit SekharDocument8 pagesSai Kiran Hospital & Kiran Infertility Center PVT - LTD - DR Samit SekharKiran IVFNo ratings yet
- AlgesiaDocument2 pagesAlgesiaNanen Camince100% (1)
- WBC MorphologyDocument47 pagesWBC MorphologyMuhammad ZakriaNo ratings yet
- Dental HygienistDocument3 pagesDental Hygienistapi-5081861230% (1)
- Recover at Work Plan 5 ProposedDocument2 pagesRecover at Work Plan 5 ProposedSiosiana DenhamNo ratings yet
- Schwannoma Vestibular ChristienDocument68 pagesSchwannoma Vestibular ChristienMaria Christien Agustie SitumorangNo ratings yet
- PQCNC CMOP/NAS/PFE LS2 McCaffreyDocument23 pagesPQCNC CMOP/NAS/PFE LS2 McCaffreykcochranNo ratings yet
- Ovario Poliquístico/Polycystic Ovary SyndromeDocument14 pagesOvario Poliquístico/Polycystic Ovary SyndromeJosé María Lauricella100% (1)
- 2 Phlebotomy Notes Taken From The Lecture of Sir Antonio Pascua JR RMTDocument5 pages2 Phlebotomy Notes Taken From The Lecture of Sir Antonio Pascua JR RMTRhoda Mae CubillaNo ratings yet
- 18 OctDocument82 pages18 OctAseel AlsheeshNo ratings yet
- Diabetes Urdu OnDocument35 pagesDiabetes Urdu OnShahid AminNo ratings yet
- Dermoscopy ChallengeDocument2 pagesDermoscopy ChallengegongutzNo ratings yet
- Aragaw 206714-1 364272Document1 pageAragaw 206714-1 364272zeine omerNo ratings yet
- Pre Feasibility Report of Pharmacy Business in PakistanDocument26 pagesPre Feasibility Report of Pharmacy Business in Pakistanzaheer100% (1)
- SJT Practice Paper 2 Large PrintDocument82 pagesSJT Practice Paper 2 Large PrintezzezzatNo ratings yet
- Susuk X RayDocument2 pagesSusuk X RayMasjid Bandar Bukit PuchongNo ratings yet
- White LabelDocument1 pageWhite LabelDee BelarminoNo ratings yet
- Clinical Epidemiology - Principles, Methods, and Applications For Clinical Research (PDFDrive)Document487 pagesClinical Epidemiology - Principles, Methods, and Applications For Clinical Research (PDFDrive)khalid balsha100% (1)
- Critical Nursing IntroductionDocument4 pagesCritical Nursing IntroductionJo Traven AzueloNo ratings yet
- Bachelor of Science in Medical Technology 2014Document6 pagesBachelor of Science in Medical Technology 2014Maxine TaeyeonNo ratings yet
- Dementia Drug StudyDocument2 pagesDementia Drug StudyBilljan TagapulotNo ratings yet
- Silingan Naka IUD, Namatay Man Gud", As Verbalized by TheDocument3 pagesSilingan Naka IUD, Namatay Man Gud", As Verbalized by TheMaxenia FaboresNo ratings yet
- Hospital Documentation ActivityDocument4 pagesHospital Documentation ActivityJANNIE BELLE RODRIGUEZNo ratings yet
- A Healthy Dose of Humor: How Laughter Benefits Mind and BodyDocument3 pagesA Healthy Dose of Humor: How Laughter Benefits Mind and BodyBen Hussa100% (2)