You might also like
- Mastering The BDS 2nd Year Hemant Gupta, 8th Ed PDFDocument807 pagesMastering The BDS 2nd Year Hemant Gupta, 8th Ed PDFSatvika67% (3)
- Gods WhispersDocument23 pagesGods WhispersRocíoEncarnaciónNo ratings yet
- Clinical Teaching Plan DRDocument10 pagesClinical Teaching Plan DRMARY ANGELICA AQUINO100% (2)
- IMH100 1st Handout - Introduction To Immunohematology, Genetics, Basic ImmunologyDocument2 pagesIMH100 1st Handout - Introduction To Immunohematology, Genetics, Basic ImmunologynicholeNo ratings yet
- Crozier Revised 2010 P02568 The History of PsychiatryDocument11 pagesCrozier Revised 2010 P02568 The History of Psychiatrygae24341No ratings yet
- Four Love StoriesDocument56 pagesFour Love Storiesyanuar esthoNo ratings yet
- Transplant Surgery: A Brief History of Renal TransplantationDocument26 pagesTransplant Surgery: A Brief History of Renal TransplantationAnonymous wLXDuQNo ratings yet
- Cardiac TransplantDocument135 pagesCardiac TransplantNakka SrikanthNo ratings yet
- P28 Transplantacija U Suvremenoj MediciniDocument41 pagesP28 Transplantacija U Suvremenoj MediciniLara TomašićNo ratings yet
- Трансплантація печінкиDocument6 pagesТрансплантація печінкиDasha TereshenkoNo ratings yet
- Chirurgia de Transplant - Curs1Document39 pagesChirurgia de Transplant - Curs1Anonymous wLXDuQNo ratings yet
- The History of Renal Transplantation:: From Imagination To RealityDocument61 pagesThe History of Renal Transplantation:: From Imagination To Realitydrj1981No ratings yet
- Overview - Tema ProiectDocument5 pagesOverview - Tema ProiectTeodora PristavuNo ratings yet
- 21 GMS Bedah JantungDocument140 pages21 GMS Bedah JantungNuravif SetianingrumNo ratings yet
- Anesthesia For Kidney Transplant: Fayez Takla, MDDocument6 pagesAnesthesia For Kidney Transplant: Fayez Takla, MDLisa NguyenNo ratings yet
- Transplantation of The Liver: Ronald W. Busuttil, MD, PHDDocument21 pagesTransplantation of The Liver: Ronald W. Busuttil, MD, PHDPaul ElidaNo ratings yet
- AKI Handout Updated 2019Document26 pagesAKI Handout Updated 2019Robert TurnbullNo ratings yet
- Renal 1Document11 pagesRenal 1hz6hkg2xm2No ratings yet
- Artificial Organs and Transplantation: G. Splendiani, S. Cipriani, A. Vega, and C. U. CascianiDocument8 pagesArtificial Organs and Transplantation: G. Splendiani, S. Cipriani, A. Vega, and C. U. CascianiIstván PortörőNo ratings yet
- Stats - CFM: ReferrenceDocument7 pagesStats - CFM: ReferrenceMunawwarah IsmailNo ratings yet
- End-Stage Renal Disease: by Jason KleinDocument11 pagesEnd-Stage Renal Disease: by Jason KleinNabighah ZukriNo ratings yet
- 1 IhDocument29 pages1 IhGennelyn Ross Delos ReyesNo ratings yet
- Organ Transplantation Historial Perspective and Current PracticeDocument14 pagesOrgan Transplantation Historial Perspective and Current Practicehkdawnwong100% (1)
- Moderator: Mr. Ram Singh (Lecturer) Deptt. of Radio-Diagnosis & Imaging, PGIMER, ChandigarhDocument119 pagesModerator: Mr. Ram Singh (Lecturer) Deptt. of Radio-Diagnosis & Imaging, PGIMER, ChandigarhMunish DograNo ratings yet
- Renal TransplantationDocument15 pagesRenal Transplantationhussain AltaherNo ratings yet
- Organ TransplantationDocument17 pagesOrgan TransplantationKushal PathakNo ratings yet
- Vte HandoutDocument55 pagesVte HandoutYantoNo ratings yet
- TransplantologyDocument41 pagesTransplantologySam InvincibleNo ratings yet
- Cardiac Stab WoundDocument7 pagesCardiac Stab WoundYogi Permana AgustaNo ratings yet
- Immunohematolog y and Blood Banking: Prerequisites - Immunology and Serology - CytogeneticsDocument6 pagesImmunohematolog y and Blood Banking: Prerequisites - Immunology and Serology - CytogeneticsMarj MendezNo ratings yet
- C.G, Vipin Shankar Iii Sem Msc. BiochemistryDocument75 pagesC.G, Vipin Shankar Iii Sem Msc. BiochemistryVipin100% (8)
- Historical Article: The First Human Renal TransplantsDocument3 pagesHistorical Article: The First Human Renal TransplantsRossalia VisserNo ratings yet
- Kidney Transplant: DefinitionDocument4 pagesKidney Transplant: Definitionetenom27No ratings yet
- Organtransplantation 130429210618 Phpapp02Document36 pagesOrgantransplantation 130429210618 Phpapp02ayan_tokNo ratings yet
- Introduction To BBDocument58 pagesIntroduction To BBRich Darlene Dela CruzNo ratings yet
- Organ TransplantationDocument37 pagesOrgan TransplantationLaila Abdul100% (1)
- SYNCOPEDocument21 pagesSYNCOPEPeter BockarieNo ratings yet
- Primary Care - Nephrology Interface: Providing Coordinated CKD CareDocument158 pagesPrimary Care - Nephrology Interface: Providing Coordinated CKD CarecamidocNo ratings yet
- Anestesiología Anestesiología AnestesiologíaDocument16 pagesAnestesiología Anestesiología AnestesiologíaIqbal HarzikyNo ratings yet
- 20th & 21st Century Medicine NewDocument22 pages20th & 21st Century Medicine NewJulian GordonNo ratings yet
- How To Start and Set A Transplant Center - Last RevisionDocument27 pagesHow To Start and Set A Transplant Center - Last RevisionChristian Nurtanto PutraNo ratings yet
- EBMT Handbook of HSCTDocument901 pagesEBMT Handbook of HSCTtonnywongso100% (2)
- Trasplante Reanl WFSADocument6 pagesTrasplante Reanl WFSAEva Eugenia Garcia MrtinezNo ratings yet
- Liver Biopsy: Mary Raina Angeli Fujiyoshi, MDDocument10 pagesLiver Biopsy: Mary Raina Angeli Fujiyoshi, MDRaina FujiyoshiNo ratings yet
- HaemodialysisDocument98 pagesHaemodialysisali aliNo ratings yet
- Project Organ Transplantation.2Document24 pagesProject Organ Transplantation.2Kunal Mahadik100% (2)
- Ezra CHF - To SsDocument91 pagesEzra CHF - To SsEzraNo ratings yet
- Locally Pelvic Advanced Rectal Cancer Kidney Complicating Adjuvant Radiation TherapyDocument4 pagesLocally Pelvic Advanced Rectal Cancer Kidney Complicating Adjuvant Radiation TherapyPaul AsturbiarisNo ratings yet
- HaemodialysisDocument98 pagesHaemodialysisKo Zin100% (1)
- Acute Mushroom Poisoning. Facebook Saves Lifes!: Mihai Popescu, MD, PHDDocument60 pagesAcute Mushroom Poisoning. Facebook Saves Lifes!: Mihai Popescu, MD, PHDMihai PopescuNo ratings yet
- Renal TransplantDocument29 pagesRenal TransplantSujith Kuttan100% (1)
- Design and Construction of Dialysis UnitsDocument4 pagesDesign and Construction of Dialysis UnitsRidho Wahyutomo100% (1)
- Heart TransplationDocument20 pagesHeart Transplationbinojdaniel17No ratings yet
- Nejm 199803263381304Document6 pagesNejm 199803263381304Syafrial BarawasNo ratings yet
- Hemodialysis: Navigation SearchDocument14 pagesHemodialysis: Navigation SearchepingNo ratings yet
- Rcpe Top20 ListDocument2 pagesRcpe Top20 ListDA WAENo ratings yet
- Transplant Surgery: "From Immunology To Surgery"Document39 pagesTransplant Surgery: "From Immunology To Surgery"lovelots1234No ratings yet
- Lesson 7 - Organ TransplantationDocument14 pagesLesson 7 - Organ Transplantationapi-307592530No ratings yet
- Critical Care for Potential Liver Transplant CandidatesFrom EverandCritical Care for Potential Liver Transplant CandidatesDmitri BezinoverNo ratings yet
- The Graft: How a Pioneering Operation Sparked the Modern Age of Organ TransplantsFrom EverandThe Graft: How a Pioneering Operation Sparked the Modern Age of Organ TransplantsRating: 5 out of 5 stars5/5 (1)
- Heart Stories: About Patients and the Great Pioneers Who Saved ThemFrom EverandHeart Stories: About Patients and the Great Pioneers Who Saved ThemNo ratings yet
- Principles of Managing Severe Acute MalnutritionDocument31 pagesPrinciples of Managing Severe Acute MalnutritionMohammad Farouq OmarNo ratings yet
- Final Thesis Otieno Churchill OchiengDocument102 pagesFinal Thesis Otieno Churchill OchiengOtieno Churchill OchiengNo ratings yet
- Dietary Supplements: What 'S in A Name? What's in The Bottle?Document3 pagesDietary Supplements: What 'S in A Name? What's in The Bottle?chrissNo ratings yet
- Ambulatory CareDocument2 pagesAmbulatory CareKarla JavierNo ratings yet
- Rle Activity No. 3Document4 pagesRle Activity No. 3Louel VicitacionNo ratings yet
- Seat Matrix JENPAS (UG) - 2021Document4 pagesSeat Matrix JENPAS (UG) - 2021Kundan JhaNo ratings yet
- CH 136: GI Infections and Enterotoxigenic Poisonings SELF-ASSESSMENT QUESTIONSDocument4 pagesCH 136: GI Infections and Enterotoxigenic Poisonings SELF-ASSESSMENT QUESTIONSTop VidsNo ratings yet
- Health 10 Health Professionals and FacilitiesDocument33 pagesHealth 10 Health Professionals and FacilitiesJM GuerreroNo ratings yet
- Acellular MatricesDocument16 pagesAcellular MatricesElo MediavillaNo ratings yet
- Nej Mo A 2310307Document11 pagesNej Mo A 2310307Víctor C. ValverdeNo ratings yet
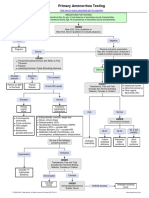
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- DKA ProtocolDocument3 pagesDKA Protocolpinky222255554100% (1)
- Cefepime-Induced NeurotoxicityDocument1 pageCefepime-Induced NeurotoxicityPetrosNo ratings yet
- History of Developmrnt of Nursing ProfessionDocument10 pagesHistory of Developmrnt of Nursing ProfessionHanison MelwynNo ratings yet
- Husel Lawsuit Against Mount Carmel-Trinity 12.26.19Document52 pagesHusel Lawsuit Against Mount Carmel-Trinity 12.26.19WOSUNo ratings yet
- Cafe Au Lait SpotsDocument2 pagesCafe Au Lait SpotsDanushNo ratings yet
- 2019 I BH PresentationDocument25 pages2019 I BH PresentationKennedy CoskerNo ratings yet
- Business Proposal: or Annual Periodic Medical Examination 2021 atDocument4 pagesBusiness Proposal: or Annual Periodic Medical Examination 2021 atsaanju87No ratings yet
- PS40 BloodMarrow Booklet 2023Document72 pagesPS40 BloodMarrow Booklet 2023wilkesgillinghamNo ratings yet
- EnoxaparinDocument9 pagesEnoxaparinMohsin AliNo ratings yet
- PolymyositisDocument5 pagesPolymyositisdeea03No ratings yet
- Club Drugs 08Document4 pagesClub Drugs 08ms15No ratings yet
- 2011 Medicare & You BookletDocument136 pages2011 Medicare & You Bookletgmen869101No ratings yet
- AssignmentDocument7 pagesAssignmentAmalina RozaniNo ratings yet
- Autoantibodies: Prof Sami Salman, FRCP, MRCP, DMR, Ces, MB CHBDocument40 pagesAutoantibodies: Prof Sami Salman, FRCP, MRCP, DMR, Ces, MB CHBamereNo ratings yet
- Antiphospholipid Syndrome: Antiphospholipid Syndrome or Antiphospholipid Antibody Syndrome (APS orDocument6 pagesAntiphospholipid Syndrome: Antiphospholipid Syndrome or Antiphospholipid Antibody Syndrome (APS orhikmat sheraniNo ratings yet