You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
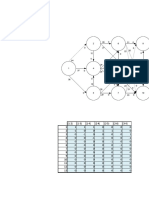
- Ejemplo Flujo MáximoDocument15 pagesEjemplo Flujo MáximoOMAR SANTIAGO LUQUE BARRERANo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Taller Simplex de RedesDocument46 pagesTaller Simplex de RedesOMAR SANTIAGO LUQUE BARRERANo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Verbos Irregulares en Inglés: Lista Completa - Profesordeingles - EuDocument7 pagesVerbos Irregulares en Inglés: Lista Completa - Profesordeingles - EuOMAR SANTIAGO LUQUE BARRERANo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Casos Especiales SimplexDocument12 pagesCasos Especiales SimplexOMAR SANTIAGO LUQUE BARRERANo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Simplex Gran MDocument6 pagesSimplex Gran MOMAR SANTIAGO LUQUE BARRERANo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Libro 1Document2 pagesLibro 1OMAR SANTIAGO LUQUE BARRERANo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Module 2 Lesson 1Document7 pagesModule 2 Lesson 1MelvinNo ratings yet
- PE3-Worksheet (LA No. 1)Document2 pagesPE3-Worksheet (LA No. 1)Peter Simon SantosNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
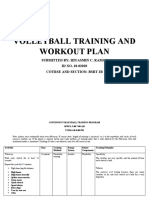
- Volleyball Training and Workout Plan: Submitted By: Hiyasmin C. Ramos ID NO. 18-02028 Course and Section: BSRT 2BDocument13 pagesVolleyball Training and Workout Plan: Submitted By: Hiyasmin C. Ramos ID NO. 18-02028 Course and Section: BSRT 2BJm100% (2)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Chapter 5Document96 pagesChapter 5Cheska AgrabioNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (842)
- TRX Essentials Flexibility Workout Guide PDFDocument15 pagesTRX Essentials Flexibility Workout Guide PDFtommyr6No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Activities - G7 Physical Education 1ST Quarter 5th and 6th WeekDocument5 pagesActivities - G7 Physical Education 1ST Quarter 5th and 6th WeekNerdboyNo ratings yet
- Lifetime Physical Fitness and Wellness A Personalized Program 13th Edition Hoeger Solutions ManualDocument12 pagesLifetime Physical Fitness and Wellness A Personalized Program 13th Edition Hoeger Solutions Manualjesseluongk6q100% (31)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Quiz 3Document7 pagesQuiz 3Rosemary DulalasNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- 97020080107Document15 pages97020080107Potnoodle75No ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- g7 Summative Test in Physical Education 1st QuarterDocument1 pageg7 Summative Test in Physical Education 1st QuarterJan Rey Francis Gregorio67% (6)
- PHYSICAL EDUCATIONQuarter 1 Module 1Document14 pagesPHYSICAL EDUCATIONQuarter 1 Module 1eonaarwen camorroNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- MAPEH 8 First Periodical TestDocument5 pagesMAPEH 8 First Periodical TestJestine ManotoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Applied Physiology For TennisDocument6 pagesApplied Physiology For TennisRodulfo AlvaradoNo ratings yet
- PE Quarter ExamDocument3 pagesPE Quarter ExamMARYANN RAUTNo ratings yet
- NCERT, CBSE Class 11 PHYSICAL EDUCATION MCQ Questions With AnswersDocument33 pagesNCERT, CBSE Class 11 PHYSICAL EDUCATION MCQ Questions With AnswersJOHN JOSHY100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Physical Medicine and Therapy. Means of PT. Therapeutic Exercise. Electrotherapy. Balneology and Climate MedicineDocument64 pagesPhysical Medicine and Therapy. Means of PT. Therapeutic Exercise. Electrotherapy. Balneology and Climate MedicineEcaterina GorganNo ratings yet
- Physical Fitness AssessmentDocument30 pagesPhysical Fitness AssessmentJingle BellsNo ratings yet
- Chest Aesthetics Training Routine PDFDocument8 pagesChest Aesthetics Training Routine PDFRamya SudarshanNo ratings yet
- Chapter-3 Physical Fitness, Wellness and LifestyleDocument13 pagesChapter-3 Physical Fitness, Wellness and LifestyleMeha 04No ratings yet
- Guide To Fix Flat FeetDocument16 pagesGuide To Fix Flat FeetLenka AnastasovskiNo ratings yet
- August 2016Document64 pagesAugust 2016Eric Santiago100% (1)
- Summer Strength ManualDocument124 pagesSummer Strength Manualdescooksey100% (2)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Physical Development: /.objectives of Physical EducationDocument6 pagesPhysical Development: /.objectives of Physical EducationAllyssa BalletaNo ratings yet
- Pe 111 CompleteDocument69 pagesPe 111 CompleteDanilo Jr Oribello Navaja100% (1)
- UNIT 1 - LEISURE ACTIVITIES - DoneDocument7 pagesUNIT 1 - LEISURE ACTIVITIES - Doneloan NguyễnNo ratings yet
- SHS Grade 11: Sports - Principles, Strategies and CoachingDocument12 pagesSHS Grade 11: Sports - Principles, Strategies and Coachingto diaryNo ratings yet
- Personal Health and Wellness 3 1Document131 pagesPersonal Health and Wellness 3 1Maan GasmenNo ratings yet
- Tutorial NotesDocument35 pagesTutorial Notesapi-401963473100% (2)
- Long Term Development in Swimming (Australia)Document11 pagesLong Term Development in Swimming (Australia)Clubear Clubear100% (1)
- Dinamik StretchingDocument38 pagesDinamik StretchingLing Lii Lik100% (2)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)