You might also like
- Philippine Blood Coordinating Council TOTAL QUALITY MANAGEMENT in Blood Service FacilitiesDocument11 pagesPhilippine Blood Coordinating Council TOTAL QUALITY MANAGEMENT in Blood Service FacilitiesDiane GaliNo ratings yet
- Family Medical History GenoGramDocument1 pageFamily Medical History GenoGramChristine Alvarez100% (1)
- Transport in Humans: Test Yourself 8.1 (Page 140)Document3 pagesTransport in Humans: Test Yourself 8.1 (Page 140)lee100% (3)
- Emergency Manajement and EffectDocument8 pagesEmergency Manajement and EffectTitik ErawatiNo ratings yet
- Heat SrokeDocument8 pagesHeat SrokeChristy BradyNo ratings yet
- Heat Stroke ArticleDocument29 pagesHeat Stroke ArticleIurascu GeaninaNo ratings yet
- Heat Illnes Ped Rev 2019Document13 pagesHeat Illnes Ped Rev 2019Sandra A. Sánchez GarcíaNo ratings yet
- Pathogenesis of Fever: Mohammad M. Sajadi - Philip A. MackowiakDocument7 pagesPathogenesis of Fever: Mohammad M. Sajadi - Philip A. MackowiakRyanNo ratings yet
- Epstein 2011Document7 pagesEpstein 2011lolNo ratings yet
- Diagnosis and Management of Heatstroke: I Gede Yasa AsmaraDocument8 pagesDiagnosis and Management of Heatstroke: I Gede Yasa AsmaraputryaNo ratings yet
- HyperthermiaDocument20 pagesHyperthermiaShereen AlobinayNo ratings yet
- The Evaluation and Management of Heat Injuries inDocument5 pagesThe Evaluation and Management of Heat Injuries inDasa HotNo ratings yet
- 4 9 Heat Stroke PDFDocument6 pages4 9 Heat Stroke PDFmia nurjanahNo ratings yet
- Altered Body Temperature: Presented By: Navjeet Kaur M.SC (NSG) 1 YRDocument68 pagesAltered Body Temperature: Presented By: Navjeet Kaur M.SC (NSG) 1 YRNithu NithuNo ratings yet
- Heat Stroke in Dogs Literature ReviewDocument11 pagesHeat Stroke in Dogs Literature ReviewGuillermo MuzasNo ratings yet
- Fever - Pathogenesis, Pathophysiology, and PurposeDocument10 pagesFever - Pathogenesis, Pathophysiology, and PurposeTiago RiosNo ratings yet
- Presented By:: Lisa Chadha M.SC (NSG) 1 YR BvconDocument69 pagesPresented By:: Lisa Chadha M.SC (NSG) 1 YR BvconHardeep KaurNo ratings yet
- 2013-143 Heat StressDocument4 pages2013-143 Heat StressArun PrakashNo ratings yet
- Fever in The Neurointensive Care UnitDocument9 pagesFever in The Neurointensive Care UnitDiayanti TentiNo ratings yet
- Exertional Heatstroke, Asesmen Cepat Dan Penatalaksanaan Tepat: Laporan KasusDocument18 pagesExertional Heatstroke, Asesmen Cepat Dan Penatalaksanaan Tepat: Laporan KasusGreen HanauNo ratings yet
- Group 4 - Bacani - 220000002117Document3 pagesGroup 4 - Bacani - 220000002117Ana Paula Bacani-SacloloNo ratings yet
- 1.TBL 1 - Acute FeverDocument8 pages1.TBL 1 - Acute FeverJeffrey FNo ratings yet
- Exertional Heatstroke, Asesmen Cepat Dan Penatalaksanaan:: Laporan KasusDocument17 pagesExertional Heatstroke, Asesmen Cepat Dan Penatalaksanaan:: Laporan KasusAndhika RcmNo ratings yet
- Inflam 2Document7 pagesInflam 2Abraham TheodoreNo ratings yet
- Heat Stroke: Early Recognition and Cooling TechniquesDocument13 pagesHeat Stroke: Early Recognition and Cooling TechniquesAniNo ratings yet
- Review Mechanism of FeverDocument8 pagesReview Mechanism of FeverYanna RizkiaNo ratings yet
- Historical Perspectives On Medical Care For Heat Stroke, Part 1: Ancient Times Through The Nineteenth CenturyDocument7 pagesHistorical Perspectives On Medical Care For Heat Stroke, Part 1: Ancient Times Through The Nineteenth CenturyAhmad Yar SukheraNo ratings yet
- Fev Mech PDFDocument7 pagesFev Mech PDFMitzu AlparisNo ratings yet
- Chapter 49 Heat InjuriesDocument8 pagesChapter 49 Heat Injuriessmith.kevin1420344No ratings yet
- Heatstroke.4Document7 pagesHeatstroke.4Ester DuwitNo ratings yet
- Chapter 5 - Fever: Pathogenesis and Treatment: Normal Body TemperatureDocument5 pagesChapter 5 - Fever: Pathogenesis and Treatment: Normal Body TemperatureGio MirandaNo ratings yet
- E-Therapeutics+ - Minor Ailments - Therapeutics - Central Nervous System Conditions - Heat-Related DisordersDocument7 pagesE-Therapeutics+ - Minor Ailments - Therapeutics - Central Nervous System Conditions - Heat-Related DisordersSamMansuriNo ratings yet
- Fever During AnesthesiaDocument19 pagesFever During AnesthesiaWindy SuryaNo ratings yet
- Term o RegulationDocument10 pagesTerm o Regulationfinna kartikaNo ratings yet
- Treatment and Prevention of Heat-Related Illness1Document10 pagesTreatment and Prevention of Heat-Related Illness1Karyn AlbaNo ratings yet
- Golpe de Calor NEJMDocument11 pagesGolpe de Calor NEJMJair Alexander Quintero PanucoNo ratings yet
- Becker 2010 FeverDocument10 pagesBecker 2010 Fever211097salNo ratings yet
- 20230923-21444-50guzkDocument6 pages20230923-21444-50guzkEster DuwitNo ratings yet
- Enfermedades Relacionadas Al CalorDocument12 pagesEnfermedades Relacionadas Al CalorJennifer Gonzalez NajeraNo ratings yet
- Thermoregulation Disorders of Central Origin - How To Diagnose and TreatDocument8 pagesThermoregulation Disorders of Central Origin - How To Diagnose and TreatCatalina GonzalezNo ratings yet
- Recent Advances in ThermoregulationDocument11 pagesRecent Advances in ThermoregulationlutfianaNo ratings yet
- Fiebre Patofisiologia WordDocument9 pagesFiebre Patofisiologia WordMatt Mathy Chang PariapazaNo ratings yet
- Ch11 HumanPhysiologicalResponsestoColdStressandHypotDocument32 pagesCh11 HumanPhysiologicalResponsestoColdStressandHypotLee SmithNo ratings yet
- Physiology of ThermoregulationDocument18 pagesPhysiology of Thermoregulationsanti sidabalokNo ratings yet
- The Effects of Heat: Climate Change and HealthDocument2 pagesThe Effects of Heat: Climate Change and HealthChantelle De GraciaNo ratings yet
- Fever TransliteDocument23 pagesFever TransliteeenNo ratings yet
- Heat StrokeDocument15 pagesHeat Strokevague_darklordNo ratings yet
- Environmental Emergencies ParamedicDocument90 pagesEnvironmental Emergencies ParamedicPaulhotvw67100% (2)
- FeverDocument5 pagesFeverdonalpampamNo ratings yet
- Stroke and Heat StrokeDocument12 pagesStroke and Heat StrokeAkinsoun MotunrayoNo ratings yet
- Thermal Regulation: Mary Frances D. PateDocument17 pagesThermal Regulation: Mary Frances D. PateWinny Shiru MachiraNo ratings yet
- Diagnosis of Pyrexia of Unknown Origin - in PracticeDocument10 pagesDiagnosis of Pyrexia of Unknown Origin - in PracticeVioletNo ratings yet
- Heat Stroke NejmDocument11 pagesHeat Stroke NejmYovita LimiawanNo ratings yet
- Temperature Regulation and Monitoring-Samar TahaDocument57 pagesTemperature Regulation and Monitoring-Samar TahapaulaNo ratings yet
- Fever of Unknown OriginDocument33 pagesFever of Unknown OriginRanjit Kumar ShahNo ratings yet
- Hyperthermia Case StudyDocument28 pagesHyperthermia Case StudyJanelle GimenezNo ratings yet
- Fever: in Children: ShouldDocument4 pagesFever: in Children: ShouldTran Trang AnhNo ratings yet
- Acut FeverDocument11 pagesAcut FeverAndreas Adrianto HandokoNo ratings yet
- Garispanduan Pengurusan Kes-Kes Yang Berkaitan Dengan Cuaca PanasDocument21 pagesGarispanduan Pengurusan Kes-Kes Yang Berkaitan Dengan Cuaca PanasHong Wei LungNo ratings yet
- Targeted Temperature Management in Brain Injured  Patients PDFDocument23 pagesTargeted Temperature Management in Brain Injured  Patients PDFCamilo Benavides BurbanoNo ratings yet
- The Healing Power of Fever: Your Body's Natural Defense against DiseaseFrom EverandThe Healing Power of Fever: Your Body's Natural Defense against DiseaseNo ratings yet
- The Ice Bath Path To Enhanced Sperm Health And Fertility - Based On The Teachings Of Dr. Andrew Huberman: Ice Baths And Male Reproductive HealthFrom EverandThe Ice Bath Path To Enhanced Sperm Health And Fertility - Based On The Teachings Of Dr. Andrew Huberman: Ice Baths And Male Reproductive HealthNo ratings yet
- Anatomy and Physiology NCSDocument2 pagesAnatomy and Physiology NCSVianah Eve EscobidoNo ratings yet
- FtytytDocument1 pageFtytytVianah Eve EscobidoNo ratings yet
- UuyyuyDocument3 pagesUuyyuyVianah Eve EscobidoNo ratings yet
- Emergency NursingDocument1 pageEmergency NursingVianah Eve EscobidoNo ratings yet
- XFRGFXGDocument1 pageXFRGFXGVianah Eve EscobidoNo ratings yet
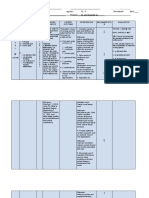
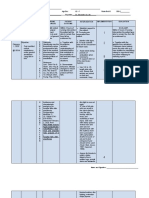
- Date/ Time Cues Need Nursing Diagnosis Patient Outcome Planning of Interventions Imple Ment Ation EvaluationDocument4 pagesDate/ Time Cues Need Nursing Diagnosis Patient Outcome Planning of Interventions Imple Ment Ation EvaluationVianah Eve EscobidoNo ratings yet
- Drug Study Diazepam and ValiumDocument4 pagesDrug Study Diazepam and ValiumVianah Eve EscobidoNo ratings yet
- Simon SaysDocument1 pageSimon SaysVianah Eve EscobidoNo ratings yet
- Acute PainDocument9 pagesAcute PainVianah Eve EscobidoNo ratings yet
- Anti MalarialDocument6 pagesAnti MalariallablikwenNo ratings yet
- Impaired Skin IntegrityDocument4 pagesImpaired Skin IntegrityVianah Eve EscobidoNo ratings yet
- Risk For InfectionDocument5 pagesRisk For InfectionVianah Eve EscobidoNo ratings yet
- Breast Mass Patient Nursing InterventionsDocument8 pagesBreast Mass Patient Nursing InterventionsVianah Eve EscobidoNo ratings yet
- Readiness For Enhance CopingDocument6 pagesReadiness For Enhance CopingVianah Eve EscobidoNo ratings yet
- Impaired Physical MobilityDocument7 pagesImpaired Physical MobilityVianah Eve EscobidoNo ratings yet
- Ineffective Tissue Perfusion - NCPDocument7 pagesIneffective Tissue Perfusion - NCPVianah Eve EscobidoNo ratings yet
- Ineffective Tissue Perfusion - NCPDocument7 pagesIneffective Tissue Perfusion - NCPVianah Eve EscobidoNo ratings yet
- Cervical Cancer - Second-Most Common Cancer Among Women - BusinessMirrorDocument4 pagesCervical Cancer - Second-Most Common Cancer Among Women - BusinessMirrorVianah Eve EscobidoNo ratings yet
- Cervical Cancer - Second-Most Common Cancer Among Women - BusinessMirrorDocument4 pagesCervical Cancer - Second-Most Common Cancer Among Women - BusinessMirrorVianah Eve EscobidoNo ratings yet
- Letters Bsn2i ObgyneDocument4 pagesLetters Bsn2i ObgyneVianah Eve EscobidoNo ratings yet
- Antihpn 2Document23 pagesAntihpn 2Vianah Eve EscobidoNo ratings yet
- Biography ST Therese of Lisieux - Biography OnlineDocument3 pagesBiography ST Therese of Lisieux - Biography OnlineVianah Eve EscobidoNo ratings yet
- Apostle Peter Biography - Timeline, Life, and DeathDocument16 pagesApostle Peter Biography - Timeline, Life, and DeathVianah Eve EscobidoNo ratings yet
- Final Research Proposal 2017 FullDocument52 pagesFinal Research Proposal 2017 FullVianah Eve EscobidoNo ratings yet
- Pregnancy Loss Can Lead To Posttraumatic StressDocument2 pagesPregnancy Loss Can Lead To Posttraumatic StressVianah Eve EscobidoNo ratings yet
- Final Research Proposal 2017Document39 pagesFinal Research Proposal 2017Vianah Eve EscobidoNo ratings yet
- Short StoryDocument6 pagesShort StoryVianah Eve EscobidoNo ratings yet
- Timeline of The Life of St. Dominic - Dominican Friars Province of St. JosephDocument10 pagesTimeline of The Life of St. Dominic - Dominican Friars Province of St. JosephVianah Eve EscobidoNo ratings yet
- Paper Transcription & Translation: Proteins: MlelrlvqgsllkkvleairDocument5 pagesPaper Transcription & Translation: Proteins: MlelrlvqgsllkkvleairXimena QuenguanNo ratings yet
- HEMOLYTIC DISEASE OF THE NEWBORN - Docx PrintDocument6 pagesHEMOLYTIC DISEASE OF THE NEWBORN - Docx PrintJudy HandlyNo ratings yet
- MeaslesDocument14 pagesMeaslesCHALIE MEQUNo ratings yet
- M.F.SC & PHD Programs in - Syllabus: Fish BiotechnologyDocument24 pagesM.F.SC & PHD Programs in - Syllabus: Fish BiotechnologyRinku AroraNo ratings yet
- Bacterial spectrum and antibiotic sensitivity patterns in bile culturesDocument127 pagesBacterial spectrum and antibiotic sensitivity patterns in bile culturesChawki MokademNo ratings yet
- DR Sangeeta T. Amladi: Professor of Dermatology G.S.M.C.& K.E.M. H, Parel, MumbaiDocument24 pagesDR Sangeeta T. Amladi: Professor of Dermatology G.S.M.C.& K.E.M. H, Parel, MumbaidoeneckeNo ratings yet
- TETANUSDocument41 pagesTETANUSruchikakaushal1910No ratings yet
- Histology SlidesDocument47 pagesHistology SlidesHaJoRaNo ratings yet
- Acute Erythroid Leukemia: Review ArticleDocument10 pagesAcute Erythroid Leukemia: Review Articlemita potabugaNo ratings yet
- Skema Modul Skor A+ Bab 5Document8 pagesSkema Modul Skor A+ Bab 5Siti MuslihahNo ratings yet
- Quality Assurance of Selective Culture Media. Método Ecometrico Mossel Et Al 1983Document15 pagesQuality Assurance of Selective Culture Media. Método Ecometrico Mossel Et Al 1983catabacteymicrobioloNo ratings yet
- Emergencia Del Virus Ebola en El Zaire y GuineaDocument8 pagesEmergencia Del Virus Ebola en El Zaire y GuineaColombiologo CaquetensisNo ratings yet
- Anti-MUM1 Antibody Ab104803: 1 Abreviews 2 ImagesDocument3 pagesAnti-MUM1 Antibody Ab104803: 1 Abreviews 2 Imageshorace35No ratings yet
- Activity No. 5 - I Scream For Ice CreamDocument5 pagesActivity No. 5 - I Scream For Ice CreamReynalyn AbaoNo ratings yet
- Whooping CoughDocument22 pagesWhooping CoughAqeel AhmadNo ratings yet
- AP Biology Unit 6 Student NotesDocument57 pagesAP Biology Unit 6 Student Notesmohammadi2No ratings yet
- Case Report: Rapport de CasDocument3 pagesCase Report: Rapport de CasfadillahidsyamNo ratings yet
- Antibacterial Activity of Medicinal Plants Against ESKAPE An Up - 2021 - HeliyoDocument12 pagesAntibacterial Activity of Medicinal Plants Against ESKAPE An Up - 2021 - HeliyoTONY VILCHEZ YARIHUAMANNo ratings yet
- Microbes Worksheet GuideDocument11 pagesMicrobes Worksheet GuideAsma MerchantNo ratings yet
- Notice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsDocument2 pagesNotice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsJustia.comNo ratings yet
- Description of Prototype Modes-of-Action Related To Repeated Dose ToxicityDocument49 pagesDescription of Prototype Modes-of-Action Related To Repeated Dose ToxicityRoy MarechaNo ratings yet
- Hematology I Intensive Rationale - Louise MDocument20 pagesHematology I Intensive Rationale - Louise MKai YoungNo ratings yet
- Core CH 27 Molecular GeneticsDocument6 pagesCore CH 27 Molecular GeneticsTSZ YAN CHEUNGNo ratings yet
- Concept of Gene and Protein SynthesisDocument39 pagesConcept of Gene and Protein SynthesisTabada NickyNo ratings yet
- Antibiotic Use in Food Animals Worldwide, With A Focus On Africa - Pluses and MinusesDocument8 pagesAntibiotic Use in Food Animals Worldwide, With A Focus On Africa - Pluses and MinusesxubicctNo ratings yet
- Jason Call's Letter To ParentsDocument2 pagesJason Call's Letter To Parentsaingram@morningjournalNo ratings yet
- 1.3 - Defense MechanismsDocument7 pages1.3 - Defense MechanismsJEMIMA RUTH MARANo ratings yet
- Understanding MicroorganismsDocument6 pagesUnderstanding MicroorganismsDanica CervantesNo ratings yet