You might also like
- The COAT & Review Approach: How to recognise and manage unwell patientsFrom EverandThe COAT & Review Approach: How to recognise and manage unwell patientsRating: 5 out of 5 stars5/5 (1)
- Ethical Challenges Faced by Health Care Facilities and Their StaffDocument14 pagesEthical Challenges Faced by Health Care Facilities and Their StaffAbirahNo ratings yet
- Consumer Centered Mental Health EducationDocument6 pagesConsumer Centered Mental Health EducationfinazkyaloNo ratings yet
- Week 5 Ethical and Legal ImplicationsDocument5 pagesWeek 5 Ethical and Legal ImplicationsHugsNo ratings yet
- Order#1150365Document10 pagesOrder#1150365Gaddafi PhelixNo ratings yet
- AETCOM 2.4Document16 pagesAETCOM 2.4jerrykruger2003No ratings yet
- Sciences Basic To PsychiatryDocument2 pagesSciences Basic To Psychiatrynisha chauhanNo ratings yet
- Duties of A Doctor - UpdatedDocument25 pagesDuties of A Doctor - UpdatedlogaritmakosinusNo ratings yet
- Issue Brief - Patient Centered Team Based Health Care - 2016Document6 pagesIssue Brief - Patient Centered Team Based Health Care - 2016Nikka Fate MartinezNo ratings yet
- BERMAS Critical-ThinkingDocument4 pagesBERMAS Critical-ThinkingBenedict James Bermas0% (1)
- Nursing Leadership and ManagementDocument32 pagesNursing Leadership and ManagementWimer100% (2)
- Nursing Leadership and ManagementDocument32 pagesNursing Leadership and ManagementWimer100% (1)
- Do You Have To Write A Thesis For Physical TherapyDocument5 pagesDo You Have To Write A Thesis For Physical Therapyafbsyebpu100% (1)
- Professionalism: An Attempt To Measure Definition and UnderstandingDocument12 pagesProfessionalism: An Attempt To Measure Definition and UnderstandingFauzia AfrozaNo ratings yet
- Knowledge Management in ACOsDocument3 pagesKnowledge Management in ACOsRohit TungaNo ratings yet
- Professional Capstone and Practicum Reflective JournalDocument8 pagesProfessional Capstone and Practicum Reflective JournalBonnieNo ratings yet
- Cultivating Healthy Collegiality Among DoctorsDocument4 pagesCultivating Healthy Collegiality Among DoctorsFransiska Adriana LarasatiNo ratings yet
- Collaborative CareDocument16 pagesCollaborative CareArdhani IrfanNo ratings yet
- Williams 2015Document2 pagesWilliams 201556 Vignesh j 079No ratings yet
- Running Head: Evaluating Organizational Change 1Document11 pagesRunning Head: Evaluating Organizational Change 1klm klmNo ratings yet
- Jayson NovellesDocument38 pagesJayson Novellesaronara dalampasiganNo ratings yet
- Core Components-Competence NursingDocument2 pagesCore Components-Competence NursingitunuNo ratings yet
- Week 16Document6 pagesWeek 16Sal MiahNo ratings yet
- Chapter 5Document5 pagesChapter 5janasnsaiNo ratings yet
- CMA PuttDocument16 pagesCMA PuttShafffNo ratings yet
- Patient Centered CareDocument11 pagesPatient Centered Careapi-336270140No ratings yet
- Ra 2Document6 pagesRa 2api-334885239No ratings yet
- Arden University: BA (Hons) Health Care ManagementDocument10 pagesArden University: BA (Hons) Health Care ManagementArslan JoiyaNo ratings yet
- Possible Exam QuestionsDocument4 pagesPossible Exam QuestionsLihle Mirriam MdlaloseNo ratings yet
- Nursing: Student Name Affiliation Course Instructor Due DateDocument8 pagesNursing: Student Name Affiliation Course Instructor Due DateHAMMADHRNo ratings yet
- Three Ways To Empower Nurses For Engaged Patients: 0 Comments Christy Davidson Becker's Hospital Review ArticleDocument15 pagesThree Ways To Empower Nurses For Engaged Patients: 0 Comments Christy Davidson Becker's Hospital Review ArticleK Jayakumar KandasamyNo ratings yet
- Models of Physician-Led Team-Based CareDocument2 pagesModels of Physician-Led Team-Based CarefreteerNo ratings yet
- Clinical Boundaries: What Parameters Determine A Midwife'S Scope of Practice?Document3 pagesClinical Boundaries: What Parameters Determine A Midwife'S Scope of Practice?Lidia AuzalikaNo ratings yet
- Patient-Practtitioner Collaborative ModelDocument20 pagesPatient-Practtitioner Collaborative ModelNestor BalboaNo ratings yet
- SAMPLE 2 GIBBSDocument5 pagesSAMPLE 2 GIBBSAhmed YusufNo ratings yet
- QDMGDocument4 pagesQDMGDan NgugiNo ratings yet
- The Philosophy of Professionalism and Professional Ethics: Cmep - 15Th AnniversaryDocument2 pagesThe Philosophy of Professionalism and Professional Ethics: Cmep - 15Th AnniversaryPramukti WibowoNo ratings yet
- Implementing a Successful Nursing Unit ReorganizationDocument5 pagesImplementing a Successful Nursing Unit ReorganizationJan Lianne BernalesNo ratings yet
- Module 1.9. Ncm119 LecDocument33 pagesModule 1.9. Ncm119 LecGailNo ratings yet
- SSDocument44 pagesSSquennieNo ratings yet
- ACTIVITY-Create-your-theory. BuendiaMikaelaMaeDocument5 pagesACTIVITY-Create-your-theory. BuendiaMikaelaMaemikaelamaebuendiaNo ratings yet
- Syndicated Seminar ProposalDocument44 pagesSyndicated Seminar ProposalBeanncaAngelesNo ratings yet
- Standards of Nursing PracticeDocument15 pagesStandards of Nursing Practiceapi-253732526No ratings yet
- Nurse's Role as Part of an Interprofessional Healthcare TeamDocument11 pagesNurse's Role as Part of an Interprofessional Healthcare TeamOmi EdNo ratings yet
- Seminar 4 Discussion 3Document7 pagesSeminar 4 Discussion 3api-643881078No ratings yet
- Nursing Practice FrameworkDocument70 pagesNursing Practice FrameworkRoselineTigga100% (1)
- Qsen Research PaperDocument5 pagesQsen Research Paperzijkchbkf100% (1)
- Nursing Code of Ethics guidelinesDocument3 pagesNursing Code of Ethics guidelinesrosita d. ramosNo ratings yet
- Hunter2012 The Integrative Medicine Team-Is Biomedical Dominance InevitableDocument6 pagesHunter2012 The Integrative Medicine Team-Is Biomedical Dominance InevitableSiu KiuNo ratings yet
- nsg-436 Ethical Decision MakingDocument6 pagesnsg-436 Ethical Decision Makingapi-491461037100% (1)
- Interview and Interdisciplinary Issue IdentificationDocument6 pagesInterview and Interdisciplinary Issue Identificationotienocliff7No ratings yet
- A Maternal and Child's Nurses Quest Towards ExcellenceDocument78 pagesA Maternal and Child's Nurses Quest Towards Excellencedecsag06No ratings yet
- Implications in Practice and Conclusions - EditedDocument11 pagesImplications in Practice and Conclusions - EditedAtanas WamukoyaNo ratings yet
- Nursing Assessment Theory by Marilynn E. DoengesDocument26 pagesNursing Assessment Theory by Marilynn E. DoengesMuhammad PanduNo ratings yet
- Working As A Team To Improve Patient CareDocument8 pagesWorking As A Team To Improve Patient CarefreteerNo ratings yet
- Decision-Making in Healthcare As A Complex Adaptive System: Craig KuziemskyDocument4 pagesDecision-Making in Healthcare As A Complex Adaptive System: Craig KuziemskyChofi SaezNo ratings yet
- PA Final Report Jan 09 Version 5Document47 pagesPA Final Report Jan 09 Version 5Sean HalliganNo ratings yet
- Sept 13 Journalreview 2 DocxDocument3 pagesSept 13 Journalreview 2 DocxHarold Mantaring LoNo ratings yet
- Case Study Theory Guided Practice Evidence Based Practice Nursing EssayDocument4 pagesCase Study Theory Guided Practice Evidence Based Practice Nursing EssayJoe AdehshinaNo ratings yet
- Principles of Medical Ethics TODAYSDocument22 pagesPrinciples of Medical Ethics TODAYSOmarNo ratings yet
- HIT EARLY HIT HARD - CF OtienoDocument22 pagesHIT EARLY HIT HARD - CF OtienoOmarNo ratings yet
- Informed Consent ExplainedDocument9 pagesInformed Consent ExplainedOmarNo ratings yet
- Human Values & Proffessional EthicsDocument67 pagesHuman Values & Proffessional EthicsOmarNo ratings yet
- Headache PAINDocument1 pageHeadache PAINOmarNo ratings yet
- Principles of Medical Ethics NewDocument8 pagesPrinciples of Medical Ethics NewOmarNo ratings yet
- Designing Ethical Research StudiesDocument11 pagesDesigning Ethical Research StudiesOmarNo ratings yet
- Introduction To Medical EthicsDocument23 pagesIntroduction To Medical EthicsOmarNo ratings yet
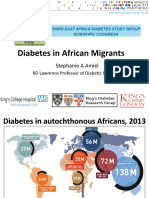
- Impact of African Ancestry on Type 2 Diabetes Progression and PathophysiologyDocument22 pagesImpact of African Ancestry on Type 2 Diabetes Progression and PathophysiologyOmarNo ratings yet
- CVD in Diabetes - EADSG 2016Document57 pagesCVD in Diabetes - EADSG 2016OmarNo ratings yet
- DR - Professionalism & EthicsDocument167 pagesDR - Professionalism & EthicsOmarNo ratings yet
- Overview of ethical issues in organ transplantationDocument16 pagesOverview of ethical issues in organ transplantationOmarNo ratings yet
- Fifty Years of Diabetes Research and CareDocument58 pagesFifty Years of Diabetes Research and CareOmarNo ratings yet
- Doctor Patient RelationshipDocument7 pagesDoctor Patient RelationshipOmarNo ratings yet
- Currently Medical Ethics For PhysiciansDocument16 pagesCurrently Medical Ethics For PhysiciansOmarNo ratings yet
- 300+ TOP NURSING Objective Questions and Answers MCQsDocument43 pages300+ TOP NURSING Objective Questions and Answers MCQsOmar50% (2)
- MBBS Physiology Exam Questions on Digestion, Absorption, HematopoiesisDocument2 pagesMBBS Physiology Exam Questions on Digestion, Absorption, HematopoiesisOmarNo ratings yet
- Syllabus For Paper I & Ii For M.B.B.S Course Subject - AnatomyDocument10 pagesSyllabus For Paper I & Ii For M.B.B.S Course Subject - AnatomyPreetam PaulNo ratings yet
- Overview of ethical issues in organ transplantationDocument16 pagesOverview of ethical issues in organ transplantationOmarNo ratings yet
- The Implications of Medical Ethics: A To ResortDocument9 pagesThe Implications of Medical Ethics: A To ResortOmarNo ratings yet
- AMA Journal of EthicsDocument83 pagesAMA Journal of EthicsOmarNo ratings yet
- Cases in Medical EthicsDocument8 pagesCases in Medical EthicsOmarNo ratings yet
- AMA Journal of EthicsDocument83 pagesAMA Journal of EthicsOmarNo ratings yet
- PDFDocument16 pagesPDFTiago CunhaNo ratings yet
- MBBS Physiology Exam Questions on Digestion, Absorption, HematopoiesisDocument2 pagesMBBS Physiology Exam Questions on Digestion, Absorption, HematopoiesisOmarNo ratings yet
- (MBBS 0221) February 2021 Sub - Code:6054 M.B.B.S. Degree Examination First Year Paper Ii - PhysiologyDocument2 pages(MBBS 0221) February 2021 Sub - Code:6054 M.B.B.S. Degree Examination First Year Paper Ii - PhysiologyOmarNo ratings yet
- Provided by Digital Library of Open University of TanzaniaDocument78 pagesProvided by Digital Library of Open University of TanzaniaOmarNo ratings yet
- The Implications of Medical Ethics: A To ResortDocument9 pagesThe Implications of Medical Ethics: A To ResortOmarNo ratings yet
- Assessment of 4th year medical student ethicsDocument5 pagesAssessment of 4th year medical student ethicsOmarNo ratings yet
- Legal Ethics Canon 14Document12 pagesLegal Ethics Canon 14prince pacasum100% (1)
- Suntay Vs SuntayDocument5 pagesSuntay Vs SuntayNikki Joanne Armecin LimNo ratings yet
- Business Ethics Policy ChecklistDocument2 pagesBusiness Ethics Policy Checklistnarasi64No ratings yet
- Subject: Appointment/ Employment Letter For Post of Executive EngineerDocument4 pagesSubject: Appointment/ Employment Letter For Post of Executive EngineerYash K. JasaniNo ratings yet
- Philips Ultrasound, Inc: See PDM For ApprovalsDocument10 pagesPhilips Ultrasound, Inc: See PDM For Approvalsboobesh kumar dNo ratings yet
- Alberta Health Services ContractDocument3 pagesAlberta Health Services ContractArjun Singh ChoudharyNo ratings yet
- IMU Studios iPlayMore Participation AgreementDocument7 pagesIMU Studios iPlayMore Participation AgreementIMU StudiosNo ratings yet
- International Distribution Agreement - Long Form - 11!22!11Document17 pagesInternational Distribution Agreement - Long Form - 11!22!11Paul Shustak100% (1)
- Sample - 2 - Consulting AgreementDocument10 pagesSample - 2 - Consulting AgreementUdeptaChoudhuryNo ratings yet
- Epson Eut432tm m192bDocument126 pagesEpson Eut432tm m192bAnonymous 1ZPqwOBHrCNo ratings yet
- Undervalued Sabah PlantersDocument9 pagesUndervalued Sabah PlantersNorazmi Abdul RahmanNo ratings yet
- Concept of Translation EthicsDocument3 pagesConcept of Translation EthicsKhrystynaNo ratings yet
- Completion Bonus: Iqor Employees Who Are Offered The Iqor Completion Incentive PlanDocument6 pagesCompletion Bonus: Iqor Employees Who Are Offered The Iqor Completion Incentive PlanNestor Del PilarNo ratings yet
- Driver ContractDocument2 pagesDriver ContractMarvin Bautista100% (1)
- Chapter 19 Professional EthicsDocument26 pagesChapter 19 Professional EthicsSavya SachiNo ratings yet
- Contract of Employment PDFDocument13 pagesContract of Employment PDFHUE HUENo ratings yet
- Informed Consent Document Format GuideDocument4 pagesInformed Consent Document Format Guidegalih cahya pratamiNo ratings yet
- Local Government of Laoac/Urdaneta City University School of Law Re: Legal Aid Extension ProgramDocument7 pagesLocal Government of Laoac/Urdaneta City University School of Law Re: Legal Aid Extension ProgramOffice AcadNo ratings yet
- Conflict of Interest FormDocument5 pagesConflict of Interest FormKelly YoungNo ratings yet
- Network Installation and Maintenance AgreementDocument2 pagesNetwork Installation and Maintenance AgreementMukesh KrishnaMurthy100% (1)
- 5 BA Privacy AgreementDocument3 pages5 BA Privacy AgreementNeil Mhartin NapolesNo ratings yet
- Test - PSW Chapter 1 Role of A Support Worker - QuizletDocument5 pagesTest - PSW Chapter 1 Role of A Support Worker - Quizletkateba Yahya0% (1)
- Assessment Task Instructions and Feedback Form: (Non-Graded)Document14 pagesAssessment Task Instructions and Feedback Form: (Non-Graded)Hà Phương100% (1)
- At-Will Employment, Confidentiality & Invention AgreementDocument17 pagesAt-Will Employment, Confidentiality & Invention Agreementeswar100% (1)
- Client CounsellingDocument19 pagesClient Counsellingparveensara18119233% (6)
- Fraud Response Plan SummaryDocument17 pagesFraud Response Plan SummaryRebbapragadaNo ratings yet
- Globe Telecom Inc.: Mutual Confidentiality and Non-Disclosure AgreementDocument3 pagesGlobe Telecom Inc.: Mutual Confidentiality and Non-Disclosure AgreementJaypee PimentelNo ratings yet
- Protecting Confidential Information and Trade SecretDocument2 pagesProtecting Confidential Information and Trade SecretRajesureshNo ratings yet
- 7.5.2016 IBHRE CCDS Physician 17 - FINAL PDFDocument8 pages7.5.2016 IBHRE CCDS Physician 17 - FINAL PDFAlexander Edo TondasNo ratings yet
- PICU-KIDS Consultant Job in BirminghamDocument10 pagesPICU-KIDS Consultant Job in BirminghamramdasNo ratings yet
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisFrom EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (9)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsFrom EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsRating: 4.5 out of 5 stars4.5/5 (38)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeFrom EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeRating: 4.5 out of 5 stars4.5/5 (140)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryFrom EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryRating: 4.5 out of 5 stars4.5/5 (157)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- An Autobiography of Trauma: A Healing JourneyFrom EverandAn Autobiography of Trauma: A Healing JourneyRating: 5 out of 5 stars5/5 (2)
- Heal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaFrom EverandHeal the Body, Heal the Mind: A Somatic Approach to Moving Beyond TraumaRating: 4.5 out of 5 stars4.5/5 (56)
- My Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesFrom EverandMy Grandmother's Hands: Racialized Trauma and the Pathway to Mending Our Hearts and BodiesRating: 5 out of 5 stars5/5 (70)
- The Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeFrom EverandThe Complex PTSD Workbook: A Mind-Body Approach to Regaining Emotional Control & Becoming WholeRating: 4.5 out of 5 stars4.5/5 (49)
- BORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONFrom EverandBORDERLINE PERSONALITY DISORDER: Help Yourself and Help Others. Articulate Guide to BPD. Tools and Techniques to Control Emotions, Anger, and Mood Swings. Save All Your Relationships and Yourself. NEW VERSIONRating: 4.5 out of 5 stars4.5/5 (24)
- Somatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionFrom EverandSomatic Therapy Workbook: A Step-by-Step Guide to Experiencing Greater Mind-Body ConnectionNo ratings yet
- Overcoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsFrom EverandOvercoming Unwanted Intrusive Thoughts: A CBT-Based Guide to Getting Over Frightening, Obsessive, or Disturbing ThoughtsRating: 4.5 out of 5 stars4.5/5 (48)
- When Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionFrom EverandWhen Religion Hurts You: Healing from Religious Trauma and the Impact of High-Control ReligionRating: 4 out of 5 stars4/5 (11)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDFrom EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDRating: 4.5 out of 5 stars4.5/5 (167)
- Don't Panic: Taking Control of Anxiety AttacksFrom EverandDon't Panic: Taking Control of Anxiety AttacksRating: 4 out of 5 stars4/5 (12)
- Embrace Your Weird: Face Your Fears and Unleash CreativityFrom EverandEmbrace Your Weird: Face Your Fears and Unleash CreativityRating: 4.5 out of 5 stars4.5/5 (124)
- Summary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisFrom EverandSummary: No Bad Parts: Healing Trauma and Restoring Wholeness with the Internal Family Systems Model by Richard C. Schwartz PhD & Alanis Morissette: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (5)
- Feel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveFrom EverandFeel the Fear… and Do It Anyway: Dynamic Techniques for Turning Fear, Indecision, and Anger into Power, Action, and LoveRating: 4 out of 5 stars4/5 (249)
- Summary: Psycho-Cybernetics: by Maxwell Maltz: Key Takeaways, Summary & AnalysisFrom EverandSummary: Psycho-Cybernetics: by Maxwell Maltz: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (2)
- Vagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerFrom EverandVagus Nerve: A Complete Self Help Guide to Stimulate and Activate Vagal Tone — A Self Healing Exercises to Reduce Chronic Illness, PTSD, Anxiety, Inflammation, Depression, Trauma, and AngerRating: 4.5 out of 5 stars4.5/5 (16)
- The Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.From EverandThe Secrets of Vagus Nerve Stimulation: 18 Proven, Science-Backed Exercises and Methods to Activate Your Vagal Tone and Heal from Inflammation, Chronic Stress, Anxiety, Epilepsy, and Depression.Rating: 5 out of 5 stars5/5 (14)
- Triggers: How We Can Stop Reacting and Start HealingFrom EverandTriggers: How We Can Stop Reacting and Start HealingRating: 5 out of 5 stars5/5 (58)
- Anxious for Nothing: Finding Calm in a Chaotic WorldFrom EverandAnxious for Nothing: Finding Calm in a Chaotic WorldRating: 4.5 out of 5 stars4.5/5 (1244)
- The Anatomy of Loneliness: How to Find Your Way Back to ConnectionFrom EverandThe Anatomy of Loneliness: How to Find Your Way Back to ConnectionRating: 4.5 out of 5 stars4.5/5 (162)