You might also like
- Conjunctivitis UpToDateDocument21 pagesConjunctivitis UpToDateRosejane MagauayNo ratings yet
- Conjunctivitis - UpToDateDocument19 pagesConjunctivitis - UpToDateEddie Mondragon GomezNo ratings yet
- Conjunctivitis - StatPearls - NCBI BookshelfDocument6 pagesConjunctivitis - StatPearls - NCBI BookshelfAngel LimNo ratings yet
- EYE INFLAMMATION GUIDEDocument28 pagesEYE INFLAMMATION GUIDENrs Sani Sule MashiNo ratings yet
- Viral Infection On HumansDocument29 pagesViral Infection On HumansMashimallowNo ratings yet
- Conjunctivitis - AAFPDocument23 pagesConjunctivitis - AAFP21613284No ratings yet
- Viral Conjunctivitis: Daniel Solano Craig N. CzyzDocument6 pagesViral Conjunctivitis: Daniel Solano Craig N. CzyzJavier BarretoNo ratings yet
- Viral Conjunctivitis AlgorithmDocument8 pagesViral Conjunctivitis AlgorithmRobert Selvin MNo ratings yet
- Conjunctivitis - UpToDateDocument18 pagesConjunctivitis - UpToDateu201416371No ratings yet
- ConjunctivitisDocument52 pagesConjunctivitisFiona H.D.100% (2)
- Ocular Surgeries, Especially in Patients On AnticoagulationDocument6 pagesOcular Surgeries, Especially in Patients On AnticoagulationaryaNo ratings yet
- MICRO BIOLOGY ConjunctivitisDocument5 pagesMICRO BIOLOGY Conjunctivitisbabyko143444No ratings yet
- CASE STUDY - ConjunctivitisDocument9 pagesCASE STUDY - ConjunctivitisAngela CancinoNo ratings yet
- SIGNS SYMPTOMS BACTERIAL CONJUNCTIVITISDocument3 pagesSIGNS SYMPTOMS BACTERIAL CONJUNCTIVITISPamela Sidharta100% (1)
- Conjunctivitis - Diagnosis & DDXDocument7 pagesConjunctivitis - Diagnosis & DDXNabillaMerdikaPutriKusumaNo ratings yet
- Primary Care: HE ED YEDocument7 pagesPrimary Care: HE ED YEHani ChoirunnisaNo ratings yet
- Ojo RojoDocument7 pagesOjo Rojoapi-3696901No ratings yet
- Eye Infections: Common, Less Common, and Potentially DevastatingDocument14 pagesEye Infections: Common, Less Common, and Potentially DevastatingAbe MicuNo ratings yet
- Eye Emergency: DR Abdelmoniem SaeedDocument63 pagesEye Emergency: DR Abdelmoniem SaeedYousef Al-AmeenNo ratings yet
- Referat KonjungtivitisDocument21 pagesReferat KonjungtivitisWyendae CliquersNo ratings yet
- ConjunctivitisDocument3 pagesConjunctivitisFaye DacsNo ratings yet
- Conjunctivitis On The Rise - Causes, Symptoms, Prevention, and TreatmentDocument2 pagesConjunctivitis On The Rise - Causes, Symptoms, Prevention, and TreatmentKamatNo ratings yet
- Conjunctivitis (Inflammation of The Eye)Document3 pagesConjunctivitis (Inflammation of The Eye)Jzia DadieNo ratings yet
- Pediatric Conjunctivitis A Review of Clinical Manifestations, Diagnosis, and TreatmentDocument9 pagesPediatric Conjunctivitis A Review of Clinical Manifestations, Diagnosis, and TreatmentVisakha VidyadeviNo ratings yet
- Prep Id 2017 FainalDocument81 pagesPrep Id 2017 Fainala alrabiaahNo ratings yet
- Conjunctivitis - Dita LSDocument17 pagesConjunctivitis - Dita LSMeNo ratings yet
- Red eye guide for GPsDocument5 pagesRed eye guide for GPsakmar887No ratings yet
- Konjungtivitis Dan KeratitisDocument117 pagesKonjungtivitis Dan KeratitisResti Puteri ApriyuslimNo ratings yet
- Causes of Pink EyeDocument2 pagesCauses of Pink EyeJoy TignoNo ratings yet
- Conjunctivitis 1Document8 pagesConjunctivitis 1Opubo BrownNo ratings yet
- Welder Et Al (2012) - Herpes Simplex Keratitis. Available At: Accessed On: 20 Agustus 2015Document24 pagesWelder Et Al (2012) - Herpes Simplex Keratitis. Available At: Accessed On: 20 Agustus 2015Silvestri PurbaNo ratings yet
- Corneal Ulcer - StatPearls - NCBI BookshelfDocument5 pagesCorneal Ulcer - StatPearls - NCBI BookshelfAngel LimNo ratings yet
- InternisDocument8 pagesInternisOrang KalonganNo ratings yet
- Children 10 00808 With CoverDocument10 pagesChildren 10 00808 With CoverSilvia OktavianiNo ratings yet
- Herpes Simplex KeratitisDocument24 pagesHerpes Simplex KeratitisAdrianaIDCNo ratings yet
- CONJUNCTIVITISDocument67 pagesCONJUNCTIVITISNauli Panjaitan86% (7)
- Eye Infection and Blepharitis by MHSNDocument18 pagesEye Infection and Blepharitis by MHSNMhsn0% (1)
- ConjuntivitisDocument21 pagesConjuntivitisjoal510No ratings yet
- Group 4: Trapago Trebucias Trinidad Umiten Vega Ventura Villalon YabresDocument86 pagesGroup 4: Trapago Trebucias Trinidad Umiten Vega Ventura Villalon YabresHunterDrimsumNo ratings yet
- Chapter 7Document6 pagesChapter 7Umarul HaziqNo ratings yet
- Tuberculosis and The EyeDocument16 pagesTuberculosis and The EyeSaid Plazola MercadoNo ratings yet
- Periorbital and Orbital Cellulitis Definitions:: Created by Carrie Rassbach, MD LPCH Pediatric Hospitalist May, 2011Document3 pagesPeriorbital and Orbital Cellulitis Definitions:: Created by Carrie Rassbach, MD LPCH Pediatric Hospitalist May, 2011Muhd Idris Aizat AdamNo ratings yet
- ConjunctivitisDocument19 pagesConjunctivitiskatrina_velasco_1No ratings yet
- Jurnal 2Document3 pagesJurnal 2danna aflahNo ratings yet
- DR Vishali's PaperDocument9 pagesDR Vishali's PaperpoojasharmachdNo ratings yet
- Right Eye Conjunctivitis Suspected ViralDocument6 pagesRight Eye Conjunctivitis Suspected ViralNia FitriyaniNo ratings yet
- 09conjunctival Infections 13-12-07Document55 pages09conjunctival Infections 13-12-07ari rujatiNo ratings yet
- Bacteria PowerpointDocument21 pagesBacteria PowerpointOpubo BrownNo ratings yet
- Conjunctivitis 09Document28 pagesConjunctivitis 09somebody_ma100% (1)
- Conjunctivitis 03Document4 pagesConjunctivitis 03Carmii CastorNo ratings yet
- James B &bron A. Lecture Notes: Ophthalmology. Ed 11. John Wiley & Sons. 2011Document9 pagesJames B &bron A. Lecture Notes: Ophthalmology. Ed 11. John Wiley & Sons. 2011qisthiNo ratings yet
- Sarra F 1996Document4 pagesSarra F 1996karinarakhmaNo ratings yet
- Journal Reading: Update On The Management of Infectious KeratitisDocument35 pagesJournal Reading: Update On The Management of Infectious KeratitisninataniaaaNo ratings yet
- ChorioretinitisDocument19 pagesChorioretinitisilmansyahandiNo ratings yet
- Pedi conjunctivitisDocument7 pagesPedi conjunctivitisfikerteadelleNo ratings yet
- Conjunctivitis: Susana A. Alfonso,, Jonie D. Fawley,, Xiaoqin Alexa LuDocument21 pagesConjunctivitis: Susana A. Alfonso,, Jonie D. Fawley,, Xiaoqin Alexa LuMichi TristeNo ratings yet
- Types of ConjunctivitisDocument20 pagesTypes of ConjunctivitisAnonymous 9lmlWQoDm8No ratings yet
- Perioperative Medication Management - UpToDateDocument46 pagesPerioperative Medication Management - UpToDateEvy Alvionita YurnaNo ratings yet
- Dampak Putusan Mahkamah Agung Nomor 365 K/PID 2012 Terhadap Kinerja Dokter Di Wilayah III CirebonDocument9 pagesDampak Putusan Mahkamah Agung Nomor 365 K/PID 2012 Terhadap Kinerja Dokter Di Wilayah III CirebonNandaa AyuuNo ratings yet
- WHO 2019 NCoV Therapeutics 2021.3 EngDocument71 pagesWHO 2019 NCoV Therapeutics 2021.3 Engnina purnamasariNo ratings yet
- Genetic Disease Is A Common Cause of Bilateral Childhood Cataract in DenmarkDocument10 pagesGenetic Disease Is A Common Cause of Bilateral Childhood Cataract in DenmarkEvy Alvionita YurnaNo ratings yet
- Congenital Cataracts 2019Document22 pagesCongenital Cataracts 2019Evy Alvionita YurnaNo ratings yet
- 10 1111@aos 14081Document6 pages10 1111@aos 14081Evy Alvionita YurnaNo ratings yet
- ASD Diagnosis Tools - UpToDateDocument3 pagesASD Diagnosis Tools - UpToDateEvy Alvionita Yurna100% (1)
- Jurnal Hukum Kesehatan 2020Document14 pagesJurnal Hukum Kesehatan 2020mona marhamahNo ratings yet
- MCQs Gynaec 2 - ObGynDocument10 pagesMCQs Gynaec 2 - ObGynbmhsh100% (3)
- Elbow Joint ConditionsDocument3 pagesElbow Joint ConditionsMarilia FarensenaNo ratings yet
- 2022 Book BreastCancerDocument601 pages2022 Book BreastCancerVera Gabor100% (1)
- The Side Effects of SmokingDocument5 pagesThe Side Effects of SmokingCentral Asian StudiesNo ratings yet
- Ncm117 Psychiatric Nursing Communication&Therapeutic Relationship Module2&3 TransDocument8 pagesNcm117 Psychiatric Nursing Communication&Therapeutic Relationship Module2&3 TransGlizzel Jade GumadeNo ratings yet
- ARDS Concept MapDocument1 pageARDS Concept Mapadro100% (2)
- The Transmission of Epidemic Influenza by R. Edgar Hope-Simpson (1992) (257pp) PDFDocument257 pagesThe Transmission of Epidemic Influenza by R. Edgar Hope-Simpson (1992) (257pp) PDFSlim Jim100% (2)
- All About NailsDocument16 pagesAll About NailsJoel MarasiganNo ratings yet
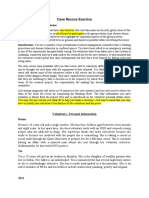
- Cave Rescue ExerciseDocument3 pagesCave Rescue ExerciserajeshNo ratings yet
- Imaging Thoracic Aortic AneurysmDocument11 pagesImaging Thoracic Aortic AneurysmHector Hernandez-SoriaNo ratings yet
- Type 2 Diabetes MellitusDocument1 pageType 2 Diabetes MellitusJúlia MeixnerNo ratings yet
- Thyroid DisordersDocument34 pagesThyroid DisordersAbdulhameed Mohamed100% (1)
- High Yield Step 1 ImagesDocument65 pagesHigh Yield Step 1 Imagesaditya mishraNo ratings yet
- Essay feedback and marks sheetDocument37 pagesEssay feedback and marks sheetParth KumarNo ratings yet
- Ped A Internship 1517300917 PDF 2Document13 pagesPed A Internship 1517300917 PDF 2dariasuslowaNo ratings yet
- A Review On The Diseases and Treatments That Affect The Bone Physiology and StrengthDocument17 pagesA Review On The Diseases and Treatments That Affect The Bone Physiology and StrengthErnest Gabriel Cruz AdvinculaNo ratings yet
- Gautam PHD Dissertation 2013Document129 pagesGautam PHD Dissertation 2013sorinaNo ratings yet
- Skin Rash Station Worksheet and HandoutDocument5 pagesSkin Rash Station Worksheet and HandoutLou EscobarNo ratings yet
- MCQ ParasitologyDocument7 pagesMCQ ParasitologyMontassar Dridi100% (1)
- Parent HandbookDocument7 pagesParent Handbookapi-238446737No ratings yet
- Data Collection in EpidemiologyDocument32 pagesData Collection in EpidemiologyOlivier MakengoNo ratings yet
- Evaluación Diagnóstica Inglés - 5 QuintoDocument6 pagesEvaluación Diagnóstica Inglés - 5 Quintonadia cespedes cruzNo ratings yet
- AVILA, Decision Making For Tooth Extraction or ConservationDocument17 pagesAVILA, Decision Making For Tooth Extraction or ConservationKathe LeyvaNo ratings yet
- Financial Markets and Institutions Mishkin 8th Edition Solutions ManualDocument34 pagesFinancial Markets and Institutions Mishkin 8th Edition Solutions Manualverrugassterrink.08ywf6100% (42)
- English-10 Q2-Module 5Document18 pagesEnglish-10 Q2-Module 5janeNo ratings yet
- Physical-Education-And-Health-11-Module 2&3Document8 pagesPhysical-Education-And-Health-11-Module 2&3Rea Mariz JordanNo ratings yet
- HydrocephalusDocument25 pagesHydrocephalusعمارہ عمرNo ratings yet
- Cardio Exercise Testing in Children and AdolecentsDocument288 pagesCardio Exercise Testing in Children and AdolecentsTeoNo ratings yet
- Research Menopause DepressionDocument5 pagesResearch Menopause DepressionVinitha JobyNo ratings yet
- Community Health Nursing: Unit Title/SDocument4 pagesCommunity Health Nursing: Unit Title/SNicole LantinNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (15)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 5 out of 5 stars5/5 (4)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 3.5 out of 5 stars3.5/5 (33)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisFrom EverandSummary: It Didn't Start with You: How Inherited Family Trauma Shapes Who We Are and How to End the Cycle By Mark Wolynn: Key Takeaways, Summary & AnalysisRating: 5 out of 5 stars5/5 (3)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- The Tennis Partner: A Doctor's Story of Friendship and LossFrom EverandThe Tennis Partner: A Doctor's Story of Friendship and LossRating: 4.5 out of 5 stars4.5/5 (4)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingFrom EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingRating: 5 out of 5 stars5/5 (5)