You might also like
- Insulin Protocols for Diabetic PatientsDocument16 pagesInsulin Protocols for Diabetic PatientsSitti Mardiya SariolNo ratings yet
- Self Monitoring Blood Glucose Recommendation ToolDocument2 pagesSelf Monitoring Blood Glucose Recommendation ToolADDC 0002 DeviNo ratings yet
- Animal RiddlerDocument3 pagesAnimal RiddlerCaro CaroNo ratings yet
- OMT Low Back Pain PDFDocument146 pagesOMT Low Back Pain PDFJavier Daza RamosNo ratings yet
- Tenses Positive Negative Introgative: I, You, We, They I, You, We, They I, You, We, TheyDocument2 pagesTenses Positive Negative Introgative: I, You, We, They I, You, We, They I, You, We, TheyRidwan baritoNo ratings yet
- Angol 3 (10) HÚZÓ KészDocument3 pagesAngol 3 (10) HÚZÓ KészAnita BaránszkyNo ratings yet
- Factors Influencing Insulin Biochemistry in UK Diabetic PatientsDocument8 pagesFactors Influencing Insulin Biochemistry in UK Diabetic PatientsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Angol 01 HÚZÓ KészDocument3 pagesAngol 01 HÚZÓ KészAnita BaránszkyNo ratings yet
- Writing PracticeDocument3 pagesWriting PracticelejozsefNo ratings yet
- Monash FODMAP Rip-Off v2.3.1Document34 pagesMonash FODMAP Rip-Off v2.3.1Calyve100% (1)
- The dyslexia debate: Key myths about identification and accommodationsDocument4 pagesThe dyslexia debate: Key myths about identification and accommodationsCatarina BarreirosNo ratings yet
- Revising Present Simple and ContinuousDocument3 pagesRevising Present Simple and ContinuousdenyNo ratings yet
- Angol Kereskedelmi Nyelvvizsga Irasbeli B2Document11 pagesAngol Kereskedelmi Nyelvvizsga Irasbeli B2Maya VeresNo ratings yet
- Angol B2 SzituációkDocument5 pagesAngol B2 SzituációkzsoieNo ratings yet
- Közlekedésinformatika: Dr. Zvikli Sándor Zvikli@sze - HuDocument243 pagesKözlekedésinformatika: Dr. Zvikli Sándor Zvikli@sze - HuBarnabás HegedűsNo ratings yet
- Színes Érettségi Feladatsorok Színes Érettségi FeladatsorokDocument4 pagesSzínes Érettségi Feladatsorok Színes Érettségi FeladatsorokSzabó ÁgnesNo ratings yet
- Insulin Start Formulas: Endocrinology & Metabolism Program, Calgary Zone, Alberta Health Services 2019Document3 pagesInsulin Start Formulas: Endocrinology & Metabolism Program, Calgary Zone, Alberta Health Services 2019DexterFrederickNo ratings yet
- FuturePumpFeatures 0809Document206 pagesFuturePumpFeatures 0809804390887No ratings yet
- 2011 - Practical Guide Insulin TherapyDocument6 pages2011 - Practical Guide Insulin Therapytheva_thy100% (1)
- Thera L15 PracticalDocument21 pagesThera L15 PracticalFatmaNo ratings yet
- DM OHA and InsulinDocument33 pagesDM OHA and InsulinPraba NanthanNo ratings yet
- EInsulin RegiemDocument18 pagesEInsulin RegiemzahrabokerNo ratings yet
- Insulin Initiation PPT - PPTX 2Document53 pagesInsulin Initiation PPT - PPTX 2Meno Ali100% (1)
- Correcting A High Blood Glucose LevelDocument5 pagesCorrecting A High Blood Glucose LevelAnnisa Fitri LidiaNo ratings yet
- Inpatient Management of Diabetes MellitusDocument38 pagesInpatient Management of Diabetes Mellitusmsala76No ratings yet
- 2022 Insulin Calculations Cheat Sheet ARDocument4 pages2022 Insulin Calculations Cheat Sheet ARGulsama BabarNo ratings yet
- CHAPTER 7 - Inpatient Management of Diabetes and HyperglycemiaDocument6 pagesCHAPTER 7 - Inpatient Management of Diabetes and HyperglycemiaenesNo ratings yet
- Insulin Therapy: Prof. Khalifa AbdallahDocument33 pagesInsulin Therapy: Prof. Khalifa AbdallahAhmed Adel MostafaNo ratings yet
- Insulin GNTDocument41 pagesInsulin GNTV Narayan Rao TummalaNo ratings yet
- Module 1 Case Study Worksheet: Name: Vasundhara Dambal InstructionsDocument4 pagesModule 1 Case Study Worksheet: Name: Vasundhara Dambal InstructionsvasuNo ratings yet
- Diabetes Insulin InitiationDocument12 pagesDiabetes Insulin InitiationSatinder BhallaNo ratings yet
- Insulin Initiation and Intensification in Type 2 DiabetesDocument54 pagesInsulin Initiation and Intensification in Type 2 DiabetesAshraf Shaaban MahfouzNo ratings yet
- Adjusting Your Insulin DoseDocument3 pagesAdjusting Your Insulin DoseLib AsNo ratings yet
- Dr.Rihab Pediatrics 02.Pediatric DM Part TwoDocument7 pagesDr.Rihab Pediatrics 02.Pediatric DM Part TwoMujtaba JawadNo ratings yet
- Practical Guidance On The Use of Premix Insulin - FinalDocument14 pagesPractical Guidance On The Use of Premix Insulin - FinalJonesius Eden ManoppoNo ratings yet
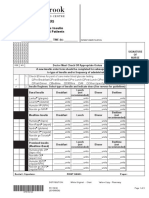
- Sunnybrook Insulin OrdersDocument5 pagesSunnybrook Insulin OrderskaybeeNo ratings yet
- Inpatient DM MX in Twenty First CenturyDocument65 pagesInpatient DM MX in Twenty First CenturyTRP TSYONo ratings yet
- Insulin Adjustment Workbook CompleteDocument53 pagesInsulin Adjustment Workbook CompletetskumarphdNo ratings yet
- Insulin Adjustment Workbook CompleteDocument53 pagesInsulin Adjustment Workbook CompleteDiabestes-stuff100% (1)
- Inpatient Guideline JoslinDocument8 pagesInpatient Guideline Joslinospinu6780No ratings yet
- Insulin Therapy: by Dr. Adithya PolavarapuDocument18 pagesInsulin Therapy: by Dr. Adithya Polavarapuadithya polavarapuNo ratings yet
- Glycemic ManagementDocument39 pagesGlycemic ManagementZayar HmunNo ratings yet
- Slentrol Treatment Plan: A Medically Appropriate Approach To Weight Management For Obese DogsDocument8 pagesSlentrol Treatment Plan: A Medically Appropriate Approach To Weight Management For Obese DogsZoran ŠušakNo ratings yet
- Calculating Insulin DoseDocument5 pagesCalculating Insulin DoseMąhmóúd SąmíNo ratings yet
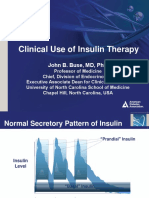
- Slide Clinical Use of Insulin Therapy (ADA)Document36 pagesSlide Clinical Use of Insulin Therapy (ADA)Dian SobaNo ratings yet
- RTD NovoMix 2017Document56 pagesRTD NovoMix 2017bayu permasuthaNo ratings yet
- DiabetesMellitisChap09 SpecialPopulationsDocument12 pagesDiabetesMellitisChap09 SpecialPopulationsarmandoNo ratings yet
- 6403 Advanced Insulin Management FinalDocument3 pages6403 Advanced Insulin Management FinalAmada Flores RubioNo ratings yet
- Fit-Diploma 3-2-2024Document57 pagesFit-Diploma 3-2-2024light tweenNo ratings yet
- Standards of Care 2021 Figure 9.2Document2 pagesStandards of Care 2021 Figure 9.2Ariel GutierrezNo ratings yet
- Comprehensive assessment and management plan for type 1 diabetesDocument37 pagesComprehensive assessment and management plan for type 1 diabetesironNo ratings yet
- Basal Bolus Insulin Concept GuideDocument1 pageBasal Bolus Insulin Concept Guideocean329No ratings yet
- Diabetes Mellitus in Pediatric: Dr. Wasnaa Hadi AbdullahDocument30 pagesDiabetes Mellitus in Pediatric: Dr. Wasnaa Hadi AbdullahLily AddamsNo ratings yet
- A GDM ProformaDocument3 pagesA GDM Proformarasnamj009No ratings yet
- A Practical Guide To Insulin TherapyDocument42 pagesA Practical Guide To Insulin Therapyseun williams100% (2)
- Calculating Insulin DoseDocument8 pagesCalculating Insulin DoseJYL academy100% (1)
- Sick Day Rules New GuidelineDocument4 pagesSick Day Rules New Guidelinerahmatullahmandozai789No ratings yet
- Insulin CorretionDocument5 pagesInsulin CorretionArshad SyahaliNo ratings yet
- Clinical Guidance On Diabetes Management at COVID-19 Patient Management FacilityDocument14 pagesClinical Guidance On Diabetes Management at COVID-19 Patient Management FacilitynrhmhealthNo ratings yet
- COVID-19 Positive Patient - Dexamethasone GuidanceDocument2 pagesCOVID-19 Positive Patient - Dexamethasone GuidanceLe Hoang TuanNo ratings yet
- Management of Perioperative Client: Unit 5Document62 pagesManagement of Perioperative Client: Unit 5Ann A.No ratings yet
- Unit 3 - OxygenationDocument53 pagesUnit 3 - OxygenationAnn A.No ratings yet
- Fluid Therapy Form Intravenous And/or HypodermoclysisDocument1 pageFluid Therapy Form Intravenous And/or HypodermoclysisAnn A.No ratings yet
- Unit 3 - OxygenationDocument53 pagesUnit 3 - OxygenationAnn A.No ratings yet
- Elimination - Urinary and BowelDocument58 pagesElimination - Urinary and BowelAnn A.No ratings yet
- Neurovascular Assessment V1.16Document1 pageNeurovascular Assessment V1.16Ann A.No ratings yet
- Allergies Adverse Reaction RecordDocument1 pageAllergies Adverse Reaction RecordAnn A.No ratings yet
- This Study Resource Was: Health Promotion, Restoration, and Preservation Through Patient EducationDocument9 pagesThis Study Resource Was: Health Promotion, Restoration, and Preservation Through Patient EducationAnn A.No ratings yet
- NorQuest Professional Portfolio Focusing on CLPNA CompetenciesDocument2 pagesNorQuest Professional Portfolio Focusing on CLPNA CompetenciesAnn A.No ratings yet
- NorQuest Professional Portfolio Focusing on CLPNA CompetenciesDocument2 pagesNorQuest Professional Portfolio Focusing on CLPNA CompetenciesAnn A.No ratings yet
- NURS 1503-M4-Patient MAR 3Document3 pagesNURS 1503-M4-Patient MAR 3Ann A.No ratings yet
- Elimination-Urinary and BowelDocument71 pagesElimination-Urinary and BowelAnn A.No ratings yet
- Medication LabelsDocument1 pageMedication LabelsAnn A.No ratings yet
- CPS Info Dimenhydrinate (Gravol)Document5 pagesCPS Info Dimenhydrinate (Gravol)Ann A.No ratings yet
- HyperHypo HandoutDocument2 pagesHyperHypo HandoutAnn A.No ratings yet
- NFDN 1002 Org Plan Practice Scenario #15 OxygenationDocument1 pageNFDN 1002 Org Plan Practice Scenario #15 OxygenationAnn A.No ratings yet
- NFDN 1002 Org Plan Practice Scenario #14 SC AnticoagulantDocument1 pageNFDN 1002 Org Plan Practice Scenario #14 SC AnticoagulantAnn A.No ratings yet
- Assignment Professional Portfolio-Marking Guide: NameDocument1 pageAssignment Professional Portfolio-Marking Guide: NameAnn A.No ratings yet
- Nutrition and HydrationDocument9 pagesNutrition and HydrationAnn A.No ratings yet
- Injection guidelines summaryDocument1 pageInjection guidelines summaryAnn A.No ratings yet
- Clean Vs Sterile TechniqueDocument5 pagesClean Vs Sterile TechniqueAda EzeNo ratings yet
- Grade 5 Teacher's Guide: Week 1 Day 1 ActivityDocument11 pagesGrade 5 Teacher's Guide: Week 1 Day 1 ActivityMemon RaFNo ratings yet
- Song: Introducing Me - Nick Jonas Parody Digestive SystemDocument2 pagesSong: Introducing Me - Nick Jonas Parody Digestive SystemCymer Romeo DizonNo ratings yet
- Assignment Food CreationDocument44 pagesAssignment Food CreationafnanNo ratings yet
- Final Thesis Nutan (2011HS07D)Document186 pagesFinal Thesis Nutan (2011HS07D)Varsha RaniNo ratings yet
- 18gym Fitness Club Nutritie 1200kcal Varianta 4Document3 pages18gym Fitness Club Nutritie 1200kcal Varianta 4Dudila MariusNo ratings yet
- Project B Amara Dietary AnalysisDocument6 pagesProject B Amara Dietary Analysisjot7799No ratings yet
- Unit-1 Infancy: S.Dharaneeshwari. 1MSC - Home Science-Food &nutritionDocument16 pagesUnit-1 Infancy: S.Dharaneeshwari. 1MSC - Home Science-Food &nutritionDharaneeshwari Siva-F&NNo ratings yet
- Document 621 8476Document61 pagesDocument 621 8476dennis.roberson462No ratings yet
- 4434 12963 1 PBDocument13 pages4434 12963 1 PBfadilababyonggo99No ratings yet
- 2014ActiveSupervisorPromotion Us ENDocument2 pages2014ActiveSupervisorPromotion Us ENflorinbroqiNo ratings yet
- Case Budica John H. Jackson Moot Court Competition 19th EditionDocument26 pagesCase Budica John H. Jackson Moot Court Competition 19th EditionNawress Ben AissaNo ratings yet
- Bonus Get LeanDocument39 pagesBonus Get LeanLeticia BarretoNo ratings yet
- Food and Nutrition: What Is Feeding?Document26 pagesFood and Nutrition: What Is Feeding?Lawrence KasambaNo ratings yet
- Primal Blueprint DietDocument10 pagesPrimal Blueprint Dietcornel100% (1)
- Week 5 Tutorial - Lab ActivityDocument4 pagesWeek 5 Tutorial - Lab Activityamisha kumarNo ratings yet
- San Miguel Products ReportDocument20 pagesSan Miguel Products Reporttricia mae GranilNo ratings yet
- Fast Food Impacts on StudentsDocument14 pagesFast Food Impacts on StudentsJonela LazaroNo ratings yet
- MSC Food and Nutrition Dissertation TopicsDocument6 pagesMSC Food and Nutrition Dissertation TopicsPayToWritePapersUK100% (1)
- Study - Id102831 - Dietary Supplements and Functional Foods WorldwideDocument78 pagesStudy - Id102831 - Dietary Supplements and Functional Foods WorldwidemustafakemalkesimNo ratings yet
- Making Cupcake Ala ShellDocument24 pagesMaking Cupcake Ala ShellSherlita Gumabon TuringanNo ratings yet
- For Protein !: Say C HeeseDocument4 pagesFor Protein !: Say C HeeseJuan Sebastian CeleitaNo ratings yet
- Class 7 Science Chapter 2 Revision NotesDocument4 pagesClass 7 Science Chapter 2 Revision NotesKanta AroraNo ratings yet
- Healthy Food Shopping ListDocument3 pagesHealthy Food Shopping ListMaite Flores Plaza100% (1)
- Dietplan Type2B Balanceddiet PDFDocument5 pagesDietplan Type2B Balanceddiet PDFMario The Coach100% (1)
- Your Supplements For Health - 1Document11 pagesYour Supplements For Health - 1Parth BhattNo ratings yet
- Rotation 4 Roleplay ScriptDocument2 pagesRotation 4 Roleplay ScriptDwynwen Aleaume GumapacNo ratings yet
- CLC 12 - Capstone Project Draft ProposalDocument5 pagesCLC 12 - Capstone Project Draft Proposalapi-573803296No ratings yet
- Nutrition in AnimalsDocument7 pagesNutrition in AnimalsDEVMONo ratings yet
- Duplichecker Plagiarism ReportDocument2 pagesDuplichecker Plagiarism ReportGAKNo ratings yet
- Child Nutrition 2021Document38 pagesChild Nutrition 2021kaltham almalkiNo ratings yet