You might also like
- Posterior Circulation Stroke: Advances in Understanding and ManagementFrom EverandPosterior Circulation Stroke: Advances in Understanding and ManagementJong S. KimNo ratings yet
- Brain Aneurysm Thesis StatementDocument7 pagesBrain Aneurysm Thesis Statementchristinewhitebillings100% (2)
- Interventional NeuroradiologyDocument8 pagesInterventional NeuroradiologyAbhinav GuptaNo ratings yet
- Aneurysm: TypesDocument12 pagesAneurysm: TypesSofia Isabelle GarciaNo ratings yet
- Their Treatments: Brain AneurysmsDocument9 pagesTheir Treatments: Brain AneurysmsArdiansyah P PratamaNo ratings yet
- BRAIN AneurysmDocument14 pagesBRAIN AneurysmRikizu HobbiesNo ratings yet
- Carotid Artery Disease FlyerDocument2 pagesCarotid Artery Disease Flyerdinh son myNo ratings yet
- A Stroke RecoveryDocument2 pagesA Stroke Recoverymanjukumard2007No ratings yet
- Cerebral AneurysmDocument6 pagesCerebral AneurysmNavjot BrarNo ratings yet
- Brain AneurysmDocument2 pagesBrain Aneurysmmactrina100% (1)
- Neurovascular Conditions Treated at PennDocument7 pagesNeurovascular Conditions Treated at PennFatrawati BahuaNo ratings yet
- Cerebral AneurysmsDocument45 pagesCerebral AneurysmsJerinNo ratings yet
- Interventional Procedure in NeurosurgeryDocument2 pagesInterventional Procedure in NeurosurgeryAbhinav GuptaNo ratings yet
- Treatment of Ischemic StrokeDocument9 pagesTreatment of Ischemic Strokeka 66No ratings yet
- Abdominal Aortic AneurysmDocument2 pagesAbdominal Aortic AneurysmSuhailah Mohd JamilNo ratings yet
- Cerebral Aneurysms: Aneurysms Posterior Circulation Basilar Artery Vertebral Arteries Posterior Communicating ArteryDocument10 pagesCerebral Aneurysms: Aneurysms Posterior Circulation Basilar Artery Vertebral Arteries Posterior Communicating ArteryRani SujithNo ratings yet
- Consent Carotid StentingDocument13 pagesConsent Carotid StentingAbhinav GuptaNo ratings yet
- Ischemic Stroke Research PaperDocument4 pagesIschemic Stroke Research Paperwihefik1t0j3100% (1)
- Brain AneurysmDocument8 pagesBrain Aneurysmzairajoy07100% (1)
- Coarctation of The AortaDocument7 pagesCoarctation of The Aortamharz_astillo100% (1)
- Case AnalysisDocument1 pageCase AnalysisCris Anne BautistaNo ratings yet
- STROKEDocument3 pagesSTROKEAddy IletoNo ratings yet
- Cardiac Stent GuideDocument6 pagesCardiac Stent GuideAbrar KhafagaNo ratings yet
- Neurovascular Conditions: Stroke and Transient Ischemic AttackDocument7 pagesNeurovascular Conditions: Stroke and Transient Ischemic AttackGinNo ratings yet
- Endovascular Coiling_UCNIDocument6 pagesEndovascular Coiling_UCNIKasturi SriramNo ratings yet
- Rle RequirementDocument101 pagesRle RequirementJe KirsteneNo ratings yet
- Health Publications: Cerebral Aneurysm Treatment and Perioperative Nursing CareDocument9 pagesHealth Publications: Cerebral Aneurysm Treatment and Perioperative Nursing CareElmer San JoseNo ratings yet
- Cerebrovascular DiseaseDocument29 pagesCerebrovascular DiseaseKamsha UyNo ratings yet
- Surgery To Remove Blood ClotsDocument16 pagesSurgery To Remove Blood ClotsGopi KrishnanNo ratings yet
- Intracranial Berry Aneurysm - Wikipedia, The Free EncyclopediaDocument3 pagesIntracranial Berry Aneurysm - Wikipedia, The Free EncyclopediaAniket MittalNo ratings yet
- pe-aneurruptDocument4 pagespe-aneurruptrungthanaporn4No ratings yet
- Stroke PhilhealthDocument5 pagesStroke PhilhealthErwin BrionesNo ratings yet
- What Is an Arteriovenous Malformation (AVM)? Symptoms, Types, Diagnosis and TreatmentDocument4 pagesWhat Is an Arteriovenous Malformation (AVM)? Symptoms, Types, Diagnosis and TreatmentRafika MonalisaNo ratings yet
- Dissertation Abdominal Aortic AneurysmDocument6 pagesDissertation Abdominal Aortic AneurysmBuyThesisPaperCanada100% (1)
- What Is A Brain Aneurysm?Document2 pagesWhat Is A Brain Aneurysm?shinNo ratings yet
- Clinical Pathway of Acute Stroke: Renz Darwin C. CastañadayDocument32 pagesClinical Pathway of Acute Stroke: Renz Darwin C. CastañadayRenz CastañadayNo ratings yet
- Britz, An Overview of Neurovascular Disease ManagementDocument2 pagesBritz, An Overview of Neurovascular Disease Managementlaila forestaNo ratings yet
- Brain Aneurysm SummaryDocument3 pagesBrain Aneurysm SummaryEvaNo ratings yet
- PTCADocument51 pagesPTCAJasmin Jacob100% (1)
- Subarachnoid Hemorrhage (SAH) : (A Type of Hemorrhagic Stroke)Document14 pagesSubarachnoid Hemorrhage (SAH) : (A Type of Hemorrhagic Stroke)calvincalebNo ratings yet
- CVDDocument67 pagesCVDRachel PerandoNo ratings yet
- Treatment: Ischemic StrokeDocument4 pagesTreatment: Ischemic StrokeGopi KrishnanNo ratings yet
- Imaging in Subarachnoid Hemorrhage - Overview, Radiography, Computed TomographyDocument13 pagesImaging in Subarachnoid Hemorrhage - Overview, Radiography, Computed TomographySaraNo ratings yet
- Cran Surg AnDocument30 pagesCran Surg AnGioGio2020No ratings yet
- Stroke in Young ThesisDocument7 pagesStroke in Young Thesisafloihzesdawig100% (1)
- Intracerebral Hemorrhage: Merck Manual Consumer VersionDocument3 pagesIntracerebral Hemorrhage: Merck Manual Consumer VersionAlamul HudaNo ratings yet
- Coronary Artery DiseaseDocument9 pagesCoronary Artery DiseaseMariquita Buenafe100% (1)
- Stroke ThesisDocument7 pagesStroke Thesisnavysavchenkobellevue100% (1)
- Cerebral Aneurysm: By: Cristi Ne Reyes Al-Sundal, RN, MN NCM 118 InstuctorDocument21 pagesCerebral Aneurysm: By: Cristi Ne Reyes Al-Sundal, RN, MN NCM 118 InstuctorVhince Norben PiscoNo ratings yet
- Stent Procedure: What Is A Stent and How Is One Used?Document18 pagesStent Procedure: What Is A Stent and How Is One Used?royflo2009No ratings yet
- AngioplastyDocument10 pagesAngioplastyВлада ХоружийNo ratings yet
- What Are Angioplasty and Vascular Stenting?Document5 pagesWhat Are Angioplasty and Vascular Stenting?mcewenpNo ratings yet
- CraniectomyDocument5 pagesCraniectomytabanaoNo ratings yet
- Dust inDocument7 pagesDust inlarkspor31No ratings yet
- Coronary Artery DiseaseDocument3 pagesCoronary Artery DiseaseMarta Luquez RNo ratings yet
- Aortic Aneurysm Info From Mass GeneralDocument8 pagesAortic Aneurysm Info From Mass Generalclubsingr28No ratings yet
- Renal Artery AneurysmDocument2 pagesRenal Artery AneurysmPete Cobra CobraitiNo ratings yet
- DR NzooloDocument21 pagesDR NzooloJohn chrisant Mwansa the future presdoNo ratings yet
- Smart Stent Detects Narrowing of ArteriesDocument3 pagesSmart Stent Detects Narrowing of ArteriesRebelandarrowNo ratings yet
- What Is A Brain AVMDocument5 pagesWhat Is A Brain AVMCj UritaNo ratings yet
- Scenario 1 Block 12: Tutor 5Document14 pagesScenario 1 Block 12: Tutor 5Syerin AudiaNo ratings yet
- SURGERY Lecture 1 - Small Intestine (Dr. Mendoza)Document16 pagesSURGERY Lecture 1 - Small Intestine (Dr. Mendoza)Medisina101100% (1)
- What Is Phlegm 1192127Document3 pagesWhat Is Phlegm 1192127xz wyNo ratings yet
- Old Canalicular Laceration Repair A Retrospective Study ofDocument6 pagesOld Canalicular Laceration Repair A Retrospective Study ofMuh Syarifullah ANo ratings yet
- EDRA Reading List v2Document3 pagesEDRA Reading List v2MubeenRahmanNo ratings yet
- Pembahasan Kuis 7 Ppu - Bahasa Inggris: B.Inggris Persiapan Utbk 2021Document8 pagesPembahasan Kuis 7 Ppu - Bahasa Inggris: B.Inggris Persiapan Utbk 202154 Hilmi Nur PersadaNo ratings yet
- CFTsDocument92 pagesCFTsSreya SanilNo ratings yet
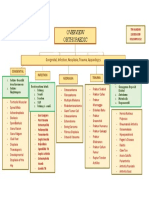
- Orthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesDocument1 pageOrthopaedic: Congenital, Infection, Neoplasia, Trauma, AppandegesdinsNo ratings yet
- Psikologi KodingDocument141 pagesPsikologi KodingAntonSusantoNo ratings yet
- Causes and Treatment of SplenomegalyDocument4 pagesCauses and Treatment of SplenomegalydoctorimrankabirNo ratings yet
- Side Effects of Aloe Vera JuiceDocument2 pagesSide Effects of Aloe Vera JuiceSumit SharmaNo ratings yet
- CancerDocument4 pagesCancerJan Jamison ZuluetaNo ratings yet
- Sexually Transmitted DiseasesDocument45 pagesSexually Transmitted DiseasesLarr SumalpongNo ratings yet
- Diagnostic Cytopathology Board Review and Self-AssessmentDocument755 pagesDiagnostic Cytopathology Board Review and Self-AssessmentJiro ManawariNo ratings yet
- Drug index for Risperdal, Diumide, Amlodipine, Linagliptin and other medicationsDocument103 pagesDrug index for Risperdal, Diumide, Amlodipine, Linagliptin and other medicationsvalencia222No ratings yet
- Castro Et Al. ProtocoloDocument10 pagesCastro Et Al. ProtocoloFrancisco Alfonso Burgos JuliánNo ratings yet
- Respiratory Part 2Document23 pagesRespiratory Part 2api-26938624No ratings yet
- ? Emergency Surgery Step-1 MCQ FinalDocument50 pages? Emergency Surgery Step-1 MCQ Finalp69b24hy8pNo ratings yet
- Causes and Types of Common Sports InjuriesDocument5 pagesCauses and Types of Common Sports InjuriesPedro HampaslupaNo ratings yet
- Opening: (EN-ES-EI-AI-DI) (EN-ES-EI-AI-DI)Document4 pagesOpening: (EN-ES-EI-AI-DI) (EN-ES-EI-AI-DI)Trisna meyanaNo ratings yet
- Corosive PoisoningDocument16 pagesCorosive Poisoninglitan dasNo ratings yet
- Top 5 Acupressure Points To Treat Cold, Flu and FeverDocument16 pagesTop 5 Acupressure Points To Treat Cold, Flu and Feverdlpurpos0% (1)
- Congenital Scoliosis Case Study: Ashley (6-7 YearsDocument20 pagesCongenital Scoliosis Case Study: Ashley (6-7 YearsIulia Dulgheru100% (1)
- Flu Report Current WeekDocument6 pagesFlu Report Current WeekNews10NBCNo ratings yet
- Pediatrics CLINICAL QUESTIONDocument14 pagesPediatrics CLINICAL QUESTIONAyesha KhatunNo ratings yet
- Fly Detox KitDocument2 pagesFly Detox Kitapi-203993890No ratings yet
- Mandatory Infants and Children Health Immunization Act of 2011 Compulsory ImmunizationDocument3 pagesMandatory Infants and Children Health Immunization Act of 2011 Compulsory Immunizationbunso padilla100% (2)
- Cervical BiopsyDocument17 pagesCervical BiopsyNestley TiongsonNo ratings yet
- A Diagnostic Dilemma in A Child With Macroscopic Hematuria, Nephrotic Syndrome and Hypocomplementemia: AnswersDocument4 pagesA Diagnostic Dilemma in A Child With Macroscopic Hematuria, Nephrotic Syndrome and Hypocomplementemia: AnswersRiszki_03No ratings yet
- Srac 0260Document4 pagesSrac 0260Wahyu SatriojatiNo ratings yet