You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
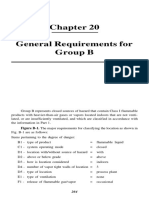
- General Requirements For Group B: Figure B-1. The Major Requirements For Classifying The Location As Shown inDocument14 pagesGeneral Requirements For Group B: Figure B-1. The Major Requirements For Classifying The Location As Shown intawfikNo ratings yet
- First Edition, Last Update January 18, 2006Document376 pagesFirst Edition, Last Update January 18, 2006tawfikNo ratings yet
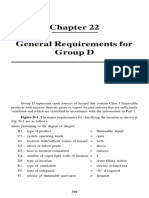
- General Requirements For Group D: Figure D-1. The Major Requirements For Classifying The Location As Shown inDocument6 pagesGeneral Requirements For Group D: Figure D-1. The Major Requirements For Classifying The Location As Shown intawfikNo ratings yet
- Energy Consumption During Extrusion-Cooking of Precooked PastaDocument8 pagesEnergy Consumption During Extrusion-Cooking of Precooked PastatawfikNo ratings yet
- Project Profile ON Banana Ripening: This Publication Is Supported byDocument33 pagesProject Profile ON Banana Ripening: This Publication Is Supported bytawfikNo ratings yet
- GTR Ne201Document146 pagesGTR Ne201tawfikNo ratings yet
- Effect of Process Variables On Spaghetti Quality': Durum Wheat and PastaDocument5 pagesEffect of Process Variables On Spaghetti Quality': Durum Wheat and PastatawfikNo ratings yet
- 45W Triple Output Medical Type: SeriesDocument2 pages45W Triple Output Medical Type: SeriestawfikNo ratings yet
- CNC Mill Calibration Procedure: 1.0 Standards and EquipmentDocument5 pagesCNC Mill Calibration Procedure: 1.0 Standards and EquipmenttawfikNo ratings yet
- ALMiG G V DRIVE 30 37 Instruction Manual 195.04032REV04 - GBDocument80 pagesALMiG G V DRIVE 30 37 Instruction Manual 195.04032REV04 - GBtawfik100% (1)
- Installation Manual: Medical Switching Power SupplyDocument4 pagesInstallation Manual: Medical Switching Power SupplytawfikNo ratings yet
- Installation Manual: Open Frame (PCB) Type Switching Power SupplyDocument3 pagesInstallation Manual: Open Frame (PCB) Type Switching Power SupplytawfikNo ratings yet
- 3Urıoh0Dfklqlqj&Hqwhuv: Revised October 2014Document26 pages3Urıoh0Dfklqlqj&Hqwhuv: Revised October 2014tawfikNo ratings yet
- Technical Explanation For Power Supplies: What Is A Power Supply?Document17 pagesTechnical Explanation For Power Supplies: What Is A Power Supply?tawfikNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- What Rewards Child PreferDocument3 pagesWhat Rewards Child PreferSudeep M. ChoudharyNo ratings yet
- Learners' Orientation For Limited Face-To-face ClassesDocument15 pagesLearners' Orientation For Limited Face-To-face ClassesVicente VicenteNo ratings yet
- CounsellingDocument6 pagesCounsellingNiharika savitaNo ratings yet
- Paper Emotional IntelligenceDocument17 pagesPaper Emotional IntelligenceCorona, Nur Shafiqah M.No ratings yet
- Blood TransfusionDocument6 pagesBlood TransfusionSophia Mae RoseteNo ratings yet
- IR 1Q2020 Prev-Min PDFDocument24 pagesIR 1Q2020 Prev-Min PDFSirc ElocinNo ratings yet
- The National Academies Press: Risk Assessment of Proposed ARFF Standards (2011)Document105 pagesThe National Academies Press: Risk Assessment of Proposed ARFF Standards (2011)Marius BuysNo ratings yet
- Vol7No1 PDFDocument56 pagesVol7No1 PDFStereo PodNo ratings yet
- Nurs 452 Community Windshield PaperDocument9 pagesNurs 452 Community Windshield Paperapi-338133673No ratings yet
- Gingival Phenotype and Its Relationship With Different Clinical Parameters: A Study in A Dominican Adult SampleDocument7 pagesGingival Phenotype and Its Relationship With Different Clinical Parameters: A Study in A Dominican Adult SampleHarish ShahNo ratings yet
- Greg Ott - Late Show Writer Packet 2020Document7 pagesGreg Ott - Late Show Writer Packet 2020Greg OttNo ratings yet
- UreaDocument1 pageUreaDesiNo ratings yet
- WFT SOW - For Wellbore Clean Up Tools (WBCU) - Sept 30th.Document1 pageWFT SOW - For Wellbore Clean Up Tools (WBCU) - Sept 30th.EduardNo ratings yet
- COVID-19 Liability Shield LawDocument13 pagesCOVID-19 Liability Shield LawGary DetmanNo ratings yet
- Hospital Readiness Checklist For Covid 19Document8 pagesHospital Readiness Checklist For Covid 19staffdev jprizalNo ratings yet
- Aesthetic Facial Anatomy Essentials For Injections-CRC Press (2020)Document259 pagesAesthetic Facial Anatomy Essentials For Injections-CRC Press (2020)stella95% (22)
- SEARO Proposal For Demonstration Project On R&D For Diabetes MellitusDocument17 pagesSEARO Proposal For Demonstration Project On R&D For Diabetes Mellitussubramanyam62No ratings yet
- 4.method Statement - Installation of FRP Lining For Steel Tank Rev02Document4 pages4.method Statement - Installation of FRP Lining For Steel Tank Rev02Sripathi SeetharamanNo ratings yet
- DLL Science 8-4thQ-2Document4 pagesDLL Science 8-4thQ-2anon_298904132100% (3)
- Patient SafetyDocument25 pagesPatient Safetyfbasudan2No ratings yet
- Allianz Care Individual BrochureDocument10 pagesAllianz Care Individual BrochureYang lai liatNo ratings yet
- Case On TrachomaDocument20 pagesCase On Trachomadimple alluriNo ratings yet
- Ginny An Analysis of Knowledge Attitude and Practices Regarding Standard Precautions of Infection Control and Impact of Knowledge and Attitude of ICU Nurses On Self-Reported Practices of InfDocument7 pagesGinny An Analysis of Knowledge Attitude and Practices Regarding Standard Precautions of Infection Control and Impact of Knowledge and Attitude of ICU Nurses On Self-Reported Practices of InfMANISHA FMSNo ratings yet
- Trauma-Informed Practice GuideDocument64 pagesTrauma-Informed Practice Guideapi-546034011100% (1)
- School Policies and Their FunctionDocument11 pagesSchool Policies and Their FunctionJessa Mae PerfiñanNo ratings yet
- Society Achievers August 2023Document104 pagesSociety Achievers August 2023magnatepublishingpvtltdNo ratings yet
- Mindfulness and Mental HealthDocument4 pagesMindfulness and Mental Healthkelvin waweruNo ratings yet
- Clinical Teaching Report - PAD &DYNAHDocument5 pagesClinical Teaching Report - PAD &DYNAHpampamaosNo ratings yet
- The Bad Weather, He Still Chooses To Go: Soal UASBN Lintas Minat Bahasa InggrisDocument7 pagesThe Bad Weather, He Still Chooses To Go: Soal UASBN Lintas Minat Bahasa InggrisHilwa FitriNo ratings yet
- Rhu Nutrition ProgramDocument12 pagesRhu Nutrition ProgrampapayNo ratings yet