You might also like
- Basic EKG Review: Identify Rhythms & InterventionsDocument31 pagesBasic EKG Review: Identify Rhythms & Interventionsmeb100% (1)
- EKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasFrom EverandEKG | ECG: An Ultimate Step-By-Step Guide to 12-Lead EKG | ECG Interpretation, Rhythms & Arrhythmias Including Basic Cardiac DysrhythmiasRating: 3 out of 5 stars3/5 (5)
- A. Cardiac Cycle: 1. Atrial Systole (Contraction of Atria) - 0.1sDocument6 pagesA. Cardiac Cycle: 1. Atrial Systole (Contraction of Atria) - 0.1sjasper haiNo ratings yet
- Airway Management TechniquesDocument48 pagesAirway Management TechniquesRea Dominique CabanillaNo ratings yet
- Cardiac Physiology MCQsDocument13 pagesCardiac Physiology MCQsالعراقي الصامد100% (2)
- Cardiac ElectrophysiologyDocument344 pagesCardiac Electrophysiologyiri_bal100% (4)
- Cardiovascular System - Electrical SystemDocument5 pagesCardiovascular System - Electrical SystemRashid DayaoNo ratings yet
- Cardio-Physiology Exam QuestionsDocument17 pagesCardio-Physiology Exam Questionsjimmy100% (1)
- CCN CardioDocument5 pagesCCN CardioSofia P. PanlilioNo ratings yet
- Estimulação Transcutânea Não InvasivaDocument10 pagesEstimulação Transcutânea Não InvasivaMarcos AcioliNo ratings yet
- HPP Lec Cvs2Document4 pagesHPP Lec Cvs2carlo baculiNo ratings yet
- Anti-Arrhythmic DrugsDocument15 pagesAnti-Arrhythmic DrugsYamin SanjuNo ratings yet
- Weekly Objectives PBL ThermoregulationDocument19 pagesWeekly Objectives PBL ThermoregulationKellyNo ratings yet
- HeartDocument4 pagesHeartArvin TaylorNo ratings yet
- N5sampleDocument12 pagesN5sampleshaikhbakhtiyar3669No ratings yet
- Antiarrhythmic DrugsDocument15 pagesAntiarrhythmic DrugsjaimeNo ratings yet
- The Heart: Gen PhysioDocument73 pagesThe Heart: Gen PhysioDawnie AlvarezNo ratings yet
- Cardiac Conduction System OverviewDocument32 pagesCardiac Conduction System OverviewNur FarinahNo ratings yet
- How the Heart Works as a Powerful PumpDocument12 pagesHow the Heart Works as a Powerful PumptohungthuyNo ratings yet
- Cardiovascular Physiology: Cardiac Muscle, Rhythm, Cycle & OutputDocument26 pagesCardiovascular Physiology: Cardiac Muscle, Rhythm, Cycle & OutputPhai KoemhienNo ratings yet
- CV 2 PHDocument22 pagesCV 2 PHaya najemNo ratings yet
- 1 7 Control of Heart RateDocument2 pages1 7 Control of Heart RateCalebNo ratings yet
- N5Document128 pagesN56qhx62pr42No ratings yet
- Blood Pressure Regulation HandoutDocument10 pagesBlood Pressure Regulation Handoutsac50900100% (2)
- Understanding Cardiac PhysiologyDocument31 pagesUnderstanding Cardiac PhysiologyTausif ChNo ratings yet
- Hemodynamics: Ncmb418 - Critical Care Nursing Rle Midterm LectureDocument7 pagesHemodynamics: Ncmb418 - Critical Care Nursing Rle Midterm LectureKyle Saberon100% (1)
- Lab08 Frog HeartDocument4 pagesLab08 Frog HeartAbie CaponponNo ratings yet
- Pacemaker learning essentialsDocument46 pagesPacemaker learning essentialsDeepak BhatNo ratings yet
- Electrocardiogram A5Document18 pagesElectrocardiogram A5FrancheskaNo ratings yet
- Manajemen Disritmia Kardiak IntraoperatifDocument53 pagesManajemen Disritmia Kardiak IntraoperatifAbi FaizNo ratings yet
- Anatomy & Physiology of The HeartDocument30 pagesAnatomy & Physiology of The HeartejarnmdNo ratings yet
- Normal Heart Rhythm: Mutiara Budi AzharDocument27 pagesNormal Heart Rhythm: Mutiara Budi AzharAditya Fresno Dwi WardhanaNo ratings yet
- CV ED Sem 2 2020 2021Document43 pagesCV ED Sem 2 2020 2021Sarhan AliNo ratings yet
- My Lecture13 - Cardiovascular PhysiologyDocument16 pagesMy Lecture13 - Cardiovascular PhysiologyVivek ChaudharyNo ratings yet
- HEART SimplifiedDocument94 pagesHEART Simplifiedcloud kumoishNo ratings yet
- Unknown EcgDocument22 pagesUnknown EcgKarthik SNo ratings yet
- Managing Cardiac Dysrhythmias and Conduction ProblemsDocument29 pagesManaging Cardiac Dysrhythmias and Conduction ProblemsYlanni Coritana100% (1)
- Understanding EKG's: Avant Healthcare ProfessionalsDocument20 pagesUnderstanding EKG's: Avant Healthcare ProfessionalsmarshaNo ratings yet
- Int9 ArrhythemiaDocument21 pagesInt9 ArrhythemiaOsama AlhumisiNo ratings yet
- Pacemaker Physics PaperDocument7 pagesPacemaker Physics PaperJose Rene BerliozNo ratings yet
- Regulation of BPDocument17 pagesRegulation of BPLemon CatbaganNo ratings yet
- First Question: Student's Name: Adel Sulaiman SectionDocument5 pagesFirst Question: Student's Name: Adel Sulaiman SectionDental LecturesMMQNo ratings yet
- Lecture 4 Properties of Myocardium and Cardiac Cycle 2020-2021Document43 pagesLecture 4 Properties of Myocardium and Cardiac Cycle 2020-2021badarbhai222No ratings yet
- Antiarrhythmic Agents Lecture NotesDocument6 pagesAntiarrhythmic Agents Lecture NotesErnest Patrick MatiasNo ratings yet
- CVS PhysiologyDocument43 pagesCVS Physiologyapi-3705050100% (1)
- Cardiac Physiology SDocument54 pagesCardiac Physiology Smutthineni.sushma28No ratings yet
- The Cardiovascular System2Document2 pagesThe Cardiovascular System2John ExcaliburNo ratings yet
- SEMIS 1 Circulatory Peripheral RespiratoryDocument21 pagesSEMIS 1 Circulatory Peripheral RespiratoryLorenz Jude CańeteNo ratings yet
- w2 Part 1Document30 pagesw2 Part 1farahafiqahNo ratings yet
- Aritmia PDFDocument114 pagesAritmia PDFRhahima SyafrilNo ratings yet
- Makalah Fisiologi VeterinerDocument8 pagesMakalah Fisiologi VeterinerZhaza AfilillaNo ratings yet
- Circulatory Response To ExerciseDocument31 pagesCirculatory Response To ExerciseFarhad GulNo ratings yet
- 12 - Cardiac Arrhythmias - 0Document12 pages12 - Cardiac Arrhythmias - 0Ehtiram HuseynovNo ratings yet
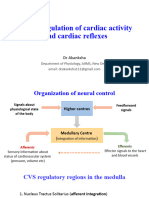
- Lecture 8 - Neural Regulation of Cardiac Activity and Cardiac ReflexesDocument35 pagesLecture 8 - Neural Regulation of Cardiac Activity and Cardiac ReflexesVishal BalamuruganNo ratings yet
- Kasus 6 (ADHF Grade II + NSTEMI + HHD + Dislipidemia) - Blok CVS - Tingkat 2 - NRP 1910211099 - REZA RAMADHANSYAHDocument34 pagesKasus 6 (ADHF Grade II + NSTEMI + HHD + Dislipidemia) - Blok CVS - Tingkat 2 - NRP 1910211099 - REZA RAMADHANSYAHReza RamadhansyahNo ratings yet
- Cardio NotesDocument15 pagesCardio NotesAngieNo ratings yet
- The Cardiovascular SystemDocument4 pagesThe Cardiovascular SystemSharie Mae MataumNo ratings yet
- Or Cardiac Physiology, Pathophysiology, and Some PharmacologyDocument58 pagesOr Cardiac Physiology, Pathophysiology, and Some PharmacologyJacob StoneNo ratings yet
- Overview of Anatomy & Physiology Assessment of CV Function: Cardiovascular SystemDocument60 pagesOverview of Anatomy & Physiology Assessment of CV Function: Cardiovascular SystemSaputra Tri NopiantoNo ratings yet
- Cardiovascular System: TH THDocument2 pagesCardiovascular System: TH THChristine Pialan SalimbagatNo ratings yet
- Nattel&Carlsson2006 Antiarrhythmic Drugs TaseDocument16 pagesNattel&Carlsson2006 Antiarrhythmic Drugs TaseGiulia AndreeaNo ratings yet
- 8C - Antiarrythmic DrugsDocument76 pages8C - Antiarrythmic DrugsShahpoor Ahmad ShirzadaNo ratings yet
- Immediate Life Support for healthcare Practitioners: A Step-By-Step GuideFrom EverandImmediate Life Support for healthcare Practitioners: A Step-By-Step GuideNo ratings yet
- #1 VASCULAR DISEASES Revised 20211029 Minus VideosDocument61 pages#1 VASCULAR DISEASES Revised 20211029 Minus VideosRea Dominique CabanillaNo ratings yet
- #2B CNS Tumors RCE Revised 20211029 2of2 Minus SpinalDocument30 pages#2B CNS Tumors RCE Revised 20211029 2of2 Minus SpinalRea Dominique CabanillaNo ratings yet
- Acc Aha Ventricular Aritmia SCD 2017 PDFDocument130 pagesAcc Aha Ventricular Aritmia SCD 2017 PDFJuwita PratiwiNo ratings yet
- CNS Tumors: Types, Symptoms and DiagnosisDocument36 pagesCNS Tumors: Types, Symptoms and DiagnosisRea Dominique CabanillaNo ratings yet
- CP3 Assignment1Document2 pagesCP3 Assignment1Rea Dominique CabanillaNo ratings yet
- One Hundred Thousand People End Up in The Hospital Every YearDocument4 pagesOne Hundred Thousand People End Up in The Hospital Every YearRea Dominique CabanillaNo ratings yet
- Aplastic Anemia, Megaloblastic Anemia & ITP TreatmentsDocument21 pagesAplastic Anemia, Megaloblastic Anemia & ITP TreatmentsRea Dominique CabanillaNo ratings yet
- Conduct of Normal Labor and DeliveryDocument141 pagesConduct of Normal Labor and DeliveryRea Dominique CabanillaNo ratings yet
- How To Critically Appraise A Paper Caroline SabinDocument38 pagesHow To Critically Appraise A Paper Caroline SabinciptaNo ratings yet
- CP3 Assignment1Document2 pagesCP3 Assignment1Rea Dominique CabanillaNo ratings yet
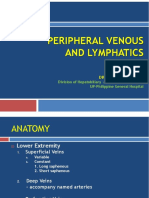
- Peripheral Venous and LymphaticsDocument34 pagesPeripheral Venous and LymphaticsRea Dominique CabanillaNo ratings yet
- Surgery II: Congenital Heart DiseaseDocument10 pagesSurgery II: Congenital Heart DiseaseRea Dominique CabanillaNo ratings yet
- Respiratory Disorders & TB in Children (Part I and Ii) - Dr. MendozaDocument17 pagesRespiratory Disorders & TB in Children (Part I and Ii) - Dr. MendozaRea Dominique CabanillaNo ratings yet
- CLINICAL DIAGNOSTIC TEST PART 2 Without KeyDocument22 pagesCLINICAL DIAGNOSTIC TEST PART 2 Without KeyRea Dominique CabanillaNo ratings yet
- Basic Diagnostic Test Part 1Document13 pagesBasic Diagnostic Test Part 1Rea Dominique CabanillaNo ratings yet
- CLINICAL DIAGNOSTIC TEST PART 2 Without KeyDocument22 pagesCLINICAL DIAGNOSTIC TEST PART 2 Without KeyRea Dominique CabanillaNo ratings yet
- Obstetric History and ExamDocument22 pagesObstetric History and ExamRea Dominique CabanillaNo ratings yet
- Genitourinary System TopicsDocument3 pagesGenitourinary System TopicsRea Dominique CabanillaNo ratings yet
- How Much Reduction in PercentDocument3 pagesHow Much Reduction in PercentRea Dominique CabanillaNo ratings yet
- Cranial Nerve AsxDocument3 pagesCranial Nerve AsxRea Dominique CabanillaNo ratings yet
- Im Cluster 2 Master Table UpdatedDocument246 pagesIm Cluster 2 Master Table UpdatedRea Dominique CabanillaNo ratings yet
- Understand Acute Hepatitis Causes and TypesDocument29 pagesUnderstand Acute Hepatitis Causes and TypesRea Dominique CabanillaNo ratings yet
- OB Normal Labor and Delivery 1Document6 pagesOB Normal Labor and Delivery 1Rea Dominique CabanillaNo ratings yet
- Surgery II: Congenital Heart DiseaseDocument10 pagesSurgery II: Congenital Heart DiseaseRea Dominique CabanillaNo ratings yet
- Pharma Case MoDocument2 pagesPharma Case MoRea Dominique CabanillaNo ratings yet
- OB Normal Labor and DeliveryDocument5 pagesOB Normal Labor and DeliveryRea Dominique CabanillaNo ratings yet
- Post-Operative Superior Mesenteric Artery Syndrome Following Retroperitoneal Sarcoma ResectionDocument6 pagesPost-Operative Superior Mesenteric Artery Syndrome Following Retroperitoneal Sarcoma ResectionRea Dominique CabanillaNo ratings yet
- IM: Gastroenterology: Approach To Patients With Liver DisordersDocument15 pagesIM: Gastroenterology: Approach To Patients With Liver DisordersRea Dominique CabanillaNo ratings yet
- Quiz On Peripheral Venous Lymphatic DiseaseDocument5 pagesQuiz On Peripheral Venous Lymphatic DiseaseRea Dominique CabanillaNo ratings yet
- Guillian-Barr e Syndrome - A Case StudyDocument11 pagesGuillian-Barr e Syndrome - A Case StudyHecan ComeNo ratings yet
- Berne & Levy Physiology 7th - Emedicodiary-325-335Document11 pagesBerne & Levy Physiology 7th - Emedicodiary-325-335eb364a0319No ratings yet
- Cardiovascular System Anatomy and Physiology - Study Guide For NursesDocument34 pagesCardiovascular System Anatomy and Physiology - Study Guide For NursesMarie ParksNo ratings yet
- Conducting System of The HeartDocument27 pagesConducting System of The HeartMuhammadNo ratings yet
- Test PhysioDocument22 pagesTest PhysioruskirururuNo ratings yet
- Learning Objectives: Chapter 4: Electrophysiology of The HeartDocument28 pagesLearning Objectives: Chapter 4: Electrophysiology of The HeartLaura PucheNo ratings yet
- EkgppDocument93 pagesEkgppLindsay WishmierNo ratings yet
- ECG WorkbookDocument0 pagesECG WorkbookJim ThorntonNo ratings yet
- EcgDocument29 pagesEcgSouvikDattaNo ratings yet
- PCOL CV - Lecture Notes 3 PCOL CV - Lecture Notes 3: Pharmacy (San Pedro College) Pharmacy (San Pedro College)Document9 pagesPCOL CV - Lecture Notes 3 PCOL CV - Lecture Notes 3: Pharmacy (San Pedro College) Pharmacy (San Pedro College)Mhiel Bhon RamzNo ratings yet
- The Heart, Part 1 - Under Pressure: Crash Course A&P # 25Document5 pagesThe Heart, Part 1 - Under Pressure: Crash Course A&P # 25Jordan TorresNo ratings yet
- Smooth & Cardiac Muscles: DR Marlini Muhamad FPSK, Usim Nov 2012Document34 pagesSmooth & Cardiac Muscles: DR Marlini Muhamad FPSK, Usim Nov 2012Harleyquinn96 DrNo ratings yet
- HeartDocument38 pagesHeartanuzNo ratings yet
- Ecg Essentials 2021 PDF by Osmosis 9d8 DR NotesDocument61 pagesEcg Essentials 2021 PDF by Osmosis 9d8 DR NotesiimjokerssNo ratings yet
- ImplantsDocument18 pagesImplantsmukeshNo ratings yet
- Permanent PacemakerDocument24 pagesPermanent PacemakerAwais PanhwarNo ratings yet
- Properties of Cardiac MuscleDocument60 pagesProperties of Cardiac MuscleBukhari Husain0% (1)
- Basic and Bedside ElectrocardiographyDocument464 pagesBasic and Bedside ElectrocardiographyBimo Panji Kumoro100% (2)
- ECG Learning ModulesDocument150 pagesECG Learning ModulesdodiNo ratings yet
- 309 Lab ReportDocument8 pages309 Lab ReportZorina Bi0% (1)
- ECG LecturesDocument144 pagesECG Lecturesİlayda KavascıkNo ratings yet
- PacemakersDocument8 pagesPacemakersVIVEK Kumar Prajapati 72No ratings yet
- Smooth and Cardiac MuscleDocument19 pagesSmooth and Cardiac Musclezahra nabilaNo ratings yet
- DocxDocument18 pagesDocxmutindaNo ratings yet
- Basics ECGpediaDocument6 pagesBasics ECGpediaCarina SuarezNo ratings yet
- Physiology of Heart in DetailDocument101 pagesPhysiology of Heart in Detailakanksha sharmaNo ratings yet
- Santa Monica Institute of Technology: Science 1: Teaching Science in Elementary Grade (Biology and Chemistry)Document8 pagesSanta Monica Institute of Technology: Science 1: Teaching Science in Elementary Grade (Biology and Chemistry)Chapz PaczNo ratings yet
- Cardiovascular SystemDocument32 pagesCardiovascular SystemAugustus Alejandro ZenitNo ratings yet