You might also like
- Citation XLS - Citation XLS Panel Poster - Revision 2 05-16 PDFDocument1 pageCitation XLS - Citation XLS Panel Poster - Revision 2 05-16 PDFAntonio Pegam100% (2)
- Family Planning Service Record Form IDocument4 pagesFamily Planning Service Record Form IBarangay Lam-anNo ratings yet
- ICIS-Petrochemicals Poster Online v7Document2 pagesICIS-Petrochemicals Poster Online v7remedali100% (1)
- FP Form ItrDocument2 pagesFP Form ItrAlibasher Macalnas100% (1)
- DGADocument1 pageDGAlapet busuk100% (1)
- Module 14 Group 1 Concept MapDocument1 pageModule 14 Group 1 Concept MapAubrey GadorNo ratings yet
- Master ChartDocument3 pagesMaster Chartsudhir74No ratings yet
- Nipt TRF MedgenomeDocument4 pagesNipt TRF MedgenomepathbiomedxNo ratings yet
- Ultimate Paeds Ref V2Document2 pagesUltimate Paeds Ref V2walkingthewardsNo ratings yet
- MATRIX VitaminsDocument1 pageMATRIX VitaminsfzattNo ratings yet
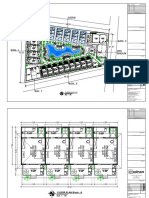
- For Construction: Legend of LandscapeDocument1 pageFor Construction: Legend of LandscapeNhan Phan ThanhNo ratings yet
- Daily Log Sheet OkDocument1 pageDaily Log Sheet OkMuzammil MirzaNo ratings yet
- DR ISRAA ADD-ModelDocument1 pageDR ISRAA ADD-ModelMohammad saidNo ratings yet
- For Construction: Doosan Heavy Industries VietnamDocument2 pagesFor Construction: Doosan Heavy Industries VietnamDoan Ngoc DucNo ratings yet
- For Construction: Doosan Heavy Industries VietnamDocument2 pagesFor Construction: Doosan Heavy Industries VietnamDoan Ngoc DucNo ratings yet
- Inoborn Errors of Metabolism Chart FINALDocument1 pageInoborn Errors of Metabolism Chart FINALfepc1966No ratings yet
- FP Form 1Document2 pagesFP Form 1hhhirangNo ratings yet
- M-02 - Ac - Vent Layout PDFDocument1 pageM-02 - Ac - Vent Layout PDFArjay 123No ratings yet
- Biochimie MetabolismDocument2 pagesBiochimie MetabolismSaca AnastasiaNo ratings yet
- Blodbank Kjoleskap FrysereDocument14 pagesBlodbank Kjoleskap FrysereRaden Mas MaulanaNo ratings yet
- Pierhead P.24.SDocument7 pagesPierhead P.24.SFella SupazaeinNo ratings yet
- Telford Test HouseDocument1 pageTelford Test HouseUmesh MishraNo ratings yet
- KPD West Side SubstationDocument2 pagesKPD West Side SubstationDigraj SinghNo ratings yet
- e C7330 - 1FDocument4 pagese C7330 - 1Fmina fawzyNo ratings yet
- Pt-Overview en PDFDocument1 pagePt-Overview en PDFimrakesh8014No ratings yet
- e C7328 - 1F PDFDocument6 pagese C7328 - 1F PDFmina fawzyNo ratings yet
- Input NilaiDocument33 pagesInput Nilaimuhrisal41No ratings yet
- For Construction: Beachfront Beachfront Softscape-Shrub-Enlarged 09Document1 pageFor Construction: Beachfront Beachfront Softscape-Shrub-Enlarged 09Nhan Phan ThanhNo ratings yet
- Dimero-D ACL-TOP 3800-6476 R1Document3 pagesDimero-D ACL-TOP 3800-6476 R1Germà JuliàNo ratings yet
- Multi-Speciality Hospital: Rajnish Anand B.I.T Mesra, Patna B.ARCH/15031/14Document1 pageMulti-Speciality Hospital: Rajnish Anand B.I.T Mesra, Patna B.ARCH/15031/14Rajnish AnandNo ratings yet
- Product Research Product 2Document2 pagesProduct Research Product 2Christian AngalotNo ratings yet
- Kuk G 0724 03 Voyage Log AbstractDocument3 pagesKuk G 0724 03 Voyage Log Abstractbarış KalkanNo ratings yet
- Input Output SummaryDocument8 pagesInput Output SummaryThinh TranNo ratings yet
- SIMPUS Laporan Register Januari 2024 LANSIA. FixDocument1 pageSIMPUS Laporan Register Januari 2024 LANSIA. FixAnik RosyidahNo ratings yet
- En El Interior de Api Coatzacoalcos Estación de Carga de Fulles de EtanoDocument1 pageEn El Interior de Api Coatzacoalcos Estación de Carga de Fulles de EtanoGustavo SánchezNo ratings yet
- JKT1 DRG CTR 3 ZZ ZZ 2503 CS01 - 002Document1 pageJKT1 DRG CTR 3 ZZ ZZ 2503 CS01 - 002Entah DimanaNo ratings yet
- Muhammad Zakwan, S.PDDocument14 pagesMuhammad Zakwan, S.PDMuhammad ZakwanNo ratings yet
- Abbot Istat 1241.2 - CartridgeMenu - Poc - Abbott PDFDocument1 pageAbbot Istat 1241.2 - CartridgeMenu - Poc - Abbott PDFmiteshshahcollegeNo ratings yet
- IPAL Cap. 22 M PDDocument2 pagesIPAL Cap. 22 M PDRomly Van PersieNo ratings yet
- Master Lower Ground: Drawing TitleDocument1 pageMaster Lower Ground: Drawing TitleFaisal Al-QurachiNo ratings yet
- SBSPDocument15 pagesSBSPzacklaws100% (1)
- A Bberi VationDocument54 pagesA Bberi Vationmistry mehulNo ratings yet
- Option 1 - Critical Equipments SupplyDocument6 pagesOption 1 - Critical Equipments Supplybrat.jose2023No ratings yet
- Grafic Asistenti Septembrie 2022-1Document1 pageGrafic Asistenti Septembrie 2022-1Romeo-Marian MihaiNo ratings yet
- Ground. (On Site) ModelDocument1 pageGround. (On Site) ModelFathima NazrinNo ratings yet
- Organism: Percentage of Susceptible Organisms Isolated From All Specimen, 83 Hospitals, Jan - Dec 2020Document2 pagesOrganism: Percentage of Susceptible Organisms Isolated From All Specimen, 83 Hospitals, Jan - Dec 2020BaronKornNo ratings yet
- Condensed ADULT DIABETIC KETOACIDOSIS (DKA) MANAGEMENT CHART Aug 2017Document2 pagesCondensed ADULT DIABETIC KETOACIDOSIS (DKA) MANAGEMENT CHART Aug 2017Zubair Mahmood KamalNo ratings yet
- Iwk KM LayoutDocument1 pageIwk KM LayoutArman ManNo ratings yet
- Floor Plan 1St: Kitchen BedroomDocument17 pagesFloor Plan 1St: Kitchen Bedroomzuldesignyahoo.comNo ratings yet
- Pemantauan Status AprilDocument2 pagesPemantauan Status AprilBendahara rutinNo ratings yet
- Tugas 7 - Pik - Pefd Pabrik Nitrobenzena - Yohanes Nico Prabowo - Kelas A - 8Document1 pageTugas 7 - Pik - Pefd Pabrik Nitrobenzena - Yohanes Nico Prabowo - Kelas A - 8Nico MarpaungNo ratings yet
- Usaid An Icn Hemocue Population 2022Document1 pageUsaid An Icn Hemocue Population 2022Samson DesieNo ratings yet
- Serveron Posterdga 160728164659Document1 pageServeron Posterdga 160728164659jycortesNo ratings yet
- Pencatatan Hasil Kegiatan Kesehatan Lanjut Usia Puskesmas Bukoposo Bulan: AprilDocument1 pagePencatatan Hasil Kegiatan Kesehatan Lanjut Usia Puskesmas Bukoposo Bulan: AprilAlta ShoopNo ratings yet
- 1D71-001-722-3209070 - Rev J - FW Cool SystDocument1 page1D71-001-722-3209070 - Rev J - FW Cool SystcontatodoerrideNo ratings yet
- Halal Certification FlowchartDocument1 pageHalal Certification FlowchartAbe Li HamzahNo ratings yet
- (PULMO) 2012 ARDS - The New Berlin DefinitionDocument4 pages(PULMO) 2012 ARDS - The New Berlin DefinitionerikaNo ratings yet
- Acute Kidney Injury: Erika Phillie T. Chua Internal Medicine ResidentDocument48 pagesAcute Kidney Injury: Erika Phillie T. Chua Internal Medicine ResidenterikaNo ratings yet
- HyperglycemiaDocument11 pagesHyperglycemiaerikaNo ratings yet
- 3/2 CBC - Na - K - Crea - TPAG - CXR Post Intubation - ABG - Eta GscsDocument2 pages3/2 CBC - Na - K - Crea - TPAG - CXR Post Intubation - ABG - Eta GscserikaNo ratings yet
- Antibiotics - Chua EDocument29 pagesAntibiotics - Chua EerikaNo ratings yet
- Adhesive Capsulitis (Frozen Shoulder)Document5 pagesAdhesive Capsulitis (Frozen Shoulder)erikaNo ratings yet
- I School - DiaCareDocument1 pageI School - DiaCareWarun KumarNo ratings yet
- Pregestational Diabetes Mellitus: Group 2Document24 pagesPregestational Diabetes Mellitus: Group 2Jellie An TalattagNo ratings yet
- Korelasi Lingkar Pinggang Dan Rasio Lingkar Pinggang-Panggul Terhadap Kadar Glukosa Plasma Menggunakan Tes Toleransi Glukosa OralDocument8 pagesKorelasi Lingkar Pinggang Dan Rasio Lingkar Pinggang-Panggul Terhadap Kadar Glukosa Plasma Menggunakan Tes Toleransi Glukosa OralFernaldi NugrahaNo ratings yet
- دراسة إحصائية لعوامل خطر الإصابة بداء السكري من النوع الثاني - دار مرضى السكري بولاية جيجل أنموذجDocument26 pagesدراسة إحصائية لعوامل خطر الإصابة بداء السكري من النوع الثاني - دار مرضى السكري بولاية جيجل أنموذجFa TeneNo ratings yet
- 2022 Insulin Calculations Cheat Sheet ARDocument4 pages2022 Insulin Calculations Cheat Sheet ARGulsama BabarNo ratings yet
- NURS FPX 5003 Assessment 1 Identifying Community Health NeedsDocument5 pagesNURS FPX 5003 Assessment 1 Identifying Community Health Needsjoohnsmith070No ratings yet
- Group 5 - English - A14-A KeperawatanDocument11 pagesGroup 5 - English - A14-A KeperawatanNi luh ade dwi AntariNo ratings yet
- Endocrine System Csec HSBDocument20 pagesEndocrine System Csec HSBNicketa AndersonNo ratings yet
- Diabetes MellitusDocument2 pagesDiabetes MellitusElyas MehdarNo ratings yet
- Diabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiDocument23 pagesDiabetic Emergencies by DR Gireesh Kumar K P, Department of Emergency Medicine, Amrita Institute of Medical Sciences, KochiSreekrishnan Trikkur100% (2)
- D-10 Dual Program Hba /F/A: Diabetes and Hemoglobinopathy Testing in One KitDocument2 pagesD-10 Dual Program Hba /F/A: Diabetes and Hemoglobinopathy Testing in One Kittawfiq bouyahiaNo ratings yet
- Scientific Research For DiabtiesDocument18 pagesScientific Research For DiabtiesSubhana HashmiNo ratings yet
- Case Study PresentationDocument35 pagesCase Study PresentationblairNo ratings yet
- Diabetic ChefDocument3 pagesDiabetic ChefVishalNo ratings yet
- NCM 118 - Lesson 13 (DKA and HHNS)Document3 pagesNCM 118 - Lesson 13 (DKA and HHNS)Bobby Christian DuronNo ratings yet
- Blood Sugar 455 MG - DL (25.25mmol - L) and What It Means - BloodSugarEasy PDFDocument4 pagesBlood Sugar 455 MG - DL (25.25mmol - L) and What It Means - BloodSugarEasy PDFSalman KhanNo ratings yet
- Glucose Measurements: Mustafa Adalgadir Khandgawi 2016Document22 pagesGlucose Measurements: Mustafa Adalgadir Khandgawi 2016Mustafa KhandgawiNo ratings yet
- Plan of Care PaperDocument5 pagesPlan of Care Paperapi-548969267No ratings yet
- ReviewDocument200 pagesReview0860833No ratings yet
- Su Hba1cDocument1 pageSu Hba1cMaherNo ratings yet
- All About Insulin: Jill E. Vollbrecht, MDDocument41 pagesAll About Insulin: Jill E. Vollbrecht, MDkeylapireNo ratings yet
- Uji Aktivitas Antidiabetes Dari Ekstrak Daun SESEWANUA (Clerodendron Squamatum Vahl.) TERHADAP Tikus Putih Jantan Galur Wistar (Rattus Norvegicus L.)Document7 pagesUji Aktivitas Antidiabetes Dari Ekstrak Daun SESEWANUA (Clerodendron Squamatum Vahl.) TERHADAP Tikus Putih Jantan Galur Wistar (Rattus Norvegicus L.)Margareta PratiwiNo ratings yet
- Select All That Apply Question Study TipsDocument2 pagesSelect All That Apply Question Study TipsjodymahmoudNo ratings yet
- AntidiabeticDrugsPJMR 20153p96 98Document4 pagesAntidiabeticDrugsPJMR 20153p96 98Tayyaba RahatNo ratings yet
- Bedah Trabekulektomi 5 Fluorourasil Dengan Antivascular Endothelial Growth Factor Pada Glaukoma Neovaskular - Nikho Melga ShalimDocument12 pagesBedah Trabekulektomi 5 Fluorourasil Dengan Antivascular Endothelial Growth Factor Pada Glaukoma Neovaskular - Nikho Melga ShalimMohammed GhalumNo ratings yet
- Bionica PumpDocument19 pagesBionica Pumpdr9348345000No ratings yet
- WCO17 AbstractBook PDFDocument674 pagesWCO17 AbstractBook PDFMihai GabrielaNo ratings yet
- Jurnal Kepatuhan Pola Asuh Pasien DiabetesDocument10 pagesJurnal Kepatuhan Pola Asuh Pasien DiabetesAuliatur RohmahNo ratings yet
- Antidiabetic Drugs: Raymund N. Tapaoan, RPHDocument23 pagesAntidiabetic Drugs: Raymund N. Tapaoan, RPHNicole EncinaresNo ratings yet
- Proceeding + Cover + Daftar Isi EditDocument346 pagesProceeding + Cover + Daftar Isi EditAndri UnairNo ratings yet