You might also like
- Acog Practice Bulletin: Antepartum Fetal SurveillanceDocument12 pagesAcog Practice Bulletin: Antepartum Fetal SurveillanceMariana Hernandez100% (10)
- Neurowerk Emg Manual en 20100104 enDocument144 pagesNeurowerk Emg Manual en 20100104 enamel kawaii100% (2)
- Bernard Le Méhauté (Auth.) - An Introduction To Hydrodynamics and Water Waves-Springer Berlin Heidelberg (1976)Document326 pagesBernard Le Méhauté (Auth.) - An Introduction To Hydrodynamics and Water Waves-Springer Berlin Heidelberg (1976)rafdi80% (5)
- Operating instructions for the Decomat 4656 dishwasherDocument16 pagesOperating instructions for the Decomat 4656 dishwasherLowayNo ratings yet
- Operating instructions for the Decomat 4656 dishwasherDocument16 pagesOperating instructions for the Decomat 4656 dishwasherLowayNo ratings yet
- Fine Sprays For Disinfection Within Healthcare: G.G.Nasr, A. Whitehead and A.J.YuleDocument18 pagesFine Sprays For Disinfection Within Healthcare: G.G.Nasr, A. Whitehead and A.J.YuledavidNo ratings yet
- Final ReportDocument18 pagesFinal ReportVijay VijiNo ratings yet
- Evaluation Study For Determination of Quantities of Disinfectant Solution Used For Fogging of Clean Rooms With Respect To Area VolumeDocument6 pagesEvaluation Study For Determination of Quantities of Disinfectant Solution Used For Fogging of Clean Rooms With Respect To Area VolumeSurjeet SamantaNo ratings yet
- SANITIZING TUNNEL PPT FinalDocument12 pagesSANITIZING TUNNEL PPT FinalSOUMYA HNo ratings yet
- pp45 47 CSJJun19Document3 pagespp45 47 CSJJun19Андрій КасійNo ratings yet
- What Is DisinfectionDocument22 pagesWhat Is DisinfectionAnn NavarroNo ratings yet
- Dissertação Traduzida-Juliana. (1)Document19 pagesDissertação Traduzida-Juliana. (1)Alessandro Sousa NascimentoNo ratings yet
- Eddy BMC ORAL HEALTHDocument9 pagesEddy BMC ORAL HEALTHSTEPHANY MENESES REYESNo ratings yet
- Sterilization of Air, Media and FermentersDocument39 pagesSterilization of Air, Media and FermentersDavion StewartNo ratings yet
- Kruger 02Document24 pagesKruger 02ab2653ncNo ratings yet
- Norm Compliant Hot Air SterilizationDocument6 pagesNorm Compliant Hot Air SterilizationAlvin IbañezNo ratings yet
- White Paper Fedegari - Decontamination by Hydrogen Peroxide Use and TechnicaldevelopmentsDocument3 pagesWhite Paper Fedegari - Decontamination by Hydrogen Peroxide Use and TechnicaldevelopmentsannunakipeNo ratings yet
- Sanitation of Pharmaceutical FacilitiesDocument6 pagesSanitation of Pharmaceutical FacilitiesJulie Ann JimenezNo ratings yet
- Microorganisms in Air SamplingDocument20 pagesMicroorganisms in Air SamplingerparixitpandeyNo ratings yet
- A Continuously Active Antimicrobial Coating Effective Against Human Coronavirus 229EDocument9 pagesA Continuously Active Antimicrobial Coating Effective Against Human Coronavirus 229ETARIK VNo ratings yet
- Sanitation of Pharmaceutical Facilities: August 2014Document6 pagesSanitation of Pharmaceutical Facilities: August 2014vitoNo ratings yet
- Aero BiologyDocument8 pagesAero BiologyFlavio ChipanaNo ratings yet
- Tikrit Journal of Pure Science: Increasing Sterilization Efficiency of Medical Waste DeviceDocument7 pagesTikrit Journal of Pure Science: Increasing Sterilization Efficiency of Medical Waste DeviceTheJokerNo ratings yet
- Sanitization of Pharmaceutical FacilitiesDocument14 pagesSanitization of Pharmaceutical FacilitiesTim Sandle100% (1)
- Sterilization and DisinfectionDocument78 pagesSterilization and DisinfectionMuhammad Shoaib50% (2)
- Sterile Products 2023 Part EDocument76 pagesSterile Products 2023 Part ESHAHIQNo ratings yet
- Pidsr Manual On Infection ControlDocument4 pagesPidsr Manual On Infection ControlKristine EstrellaNo ratings yet
- pulsFOG Aerosoldisinfection in Public Health HygieneDocument16 pagespulsFOG Aerosoldisinfection in Public Health Hygienecoralmoise64No ratings yet
- Cleaning and Disinfection of Cleanrooms PDFDocument11 pagesCleaning and Disinfection of Cleanrooms PDFnguyen ngoc HieuNo ratings yet
- Application Guide: Solution Air-Handling Units Uv-C Light OptionsDocument12 pagesApplication Guide: Solution Air-Handling Units Uv-C Light OptionsBruno GuedesNo ratings yet
- Disinfection GatewayDocument6 pagesDisinfection GatewaylynnNo ratings yet
- Hospital Textiles, Are They A Possible Vehicle For Healthcare-Associated Infections?Document14 pagesHospital Textiles, Are They A Possible Vehicle For Healthcare-Associated Infections?Muhammad Nadeem RazaNo ratings yet
- ASPIRO TechnologyDocument19 pagesASPIRO Technologysehyong0419No ratings yet
- Infection Control in Restorative DentistryDocument32 pagesInfection Control in Restorative Dentistryjamaica faith ramonNo ratings yet
- Gerpac 2014 ReviewDocument3 pagesGerpac 2014 ReviewTim SandleNo ratings yet
- Sterilization and Surveillance of Operation Theatres in Developing WorldDocument5 pagesSterilization and Surveillance of Operation Theatres in Developing Worldtummalapalli venkateswara raoNo ratings yet
- A? A? A? A? A?: Nosocomial Epidemiology Public HealthDocument8 pagesA? A? A? A? A?: Nosocomial Epidemiology Public HealthAbhijeet TambeNo ratings yet
- Automatic Fogging Disinfection Unit Effectively Cleans Operating RoomsDocument5 pagesAutomatic Fogging Disinfection Unit Effectively Cleans Operating RoomsDavid Adolfo Paez MolinaNo ratings yet
- Extraction Processes Assisted by UltrasoundDocument18 pagesExtraction Processes Assisted by UltrasoundDr. YUSHINTA ARISTINA SANJAYA, SPi., MP. DTP-Dosen Teknologi PanganNo ratings yet
- Ultraviolet Disinfection Robots To Improve Hospital Cleaning: Real Promise or Just A Gimmick?Document3 pagesUltraviolet Disinfection Robots To Improve Hospital Cleaning: Real Promise or Just A Gimmick?RopareNo ratings yet
- Cleaning and Disinfection of Pharmaceutical CleanroomsDocument11 pagesCleaning and Disinfection of Pharmaceutical Cleanroomss.sotomayorNo ratings yet
- McQuay UV News LetterDocument4 pagesMcQuay UV News LetterVipul JainNo ratings yet
- MED. Dental Services (Infectionn Control 1) .003docDocument7 pagesMED. Dental Services (Infectionn Control 1) .003docKenny JosefNo ratings yet
- Fumigation in Operation TheatresDocument22 pagesFumigation in Operation TheatresUtkarsh RaiNo ratings yet
- Whole Room DisinfectionDocument68 pagesWhole Room Disinfectionkfujiwar100% (1)
- Tristar Uvc Disinfecting CabinetDocument9 pagesTristar Uvc Disinfecting CabinetshobhitmahawarNo ratings yet
- Corelation Between Machines Assisted EndodonticDocument7 pagesCorelation Between Machines Assisted EndodonticdinaNo ratings yet
- Ijerph 16 03572Document10 pagesIjerph 16 03572Cassie AbernathNo ratings yet
- Safe Use of Microbubbles For Removal of Ro Membrane FoulingDocument18 pagesSafe Use of Microbubbles For Removal of Ro Membrane Foulingashraf refaatNo ratings yet
- Journal of Dentistry: M.A. Boyle, M.J. O 'Donnell, R.J. Russell, N. Galvin, J. Swan, D.C. ColemanDocument12 pagesJournal of Dentistry: M.A. Boyle, M.J. O 'Donnell, R.J. Russell, N. Galvin, J. Swan, D.C. ColemanAlexandru Codrin-IonutNo ratings yet
- Nuclear Engineering and TechnologyDocument8 pagesNuclear Engineering and TechnologyBharat MahajanNo ratings yet
- Review - Spray DryerDocument4 pagesReview - Spray DryerGusmannNo ratings yet
- New Guidelines for Infection Control and SterilizationDocument43 pagesNew Guidelines for Infection Control and SterilizationLama AhmadNo ratings yet
- How SterilAir PRO Effectively Prevents Airborne InfectionsDocument12 pagesHow SterilAir PRO Effectively Prevents Airborne InfectionssayedNo ratings yet
- Ventilation Performance in The Operating Theatre Against Airborne Infection Numerical Study On An Ultra-Clean SystemDocument10 pagesVentilation Performance in The Operating Theatre Against Airborne Infection Numerical Study On An Ultra-Clean SystemVL KohNo ratings yet
- Disinfection of Impression Materials II-1-4Document4 pagesDisinfection of Impression Materials II-1-4ananthNo ratings yet
- Environment Monitoring, Result Evaluation and Common Contaminants Study of Vaccine Manufacturing FacilityDocument12 pagesEnvironment Monitoring, Result Evaluation and Common Contaminants Study of Vaccine Manufacturing FacilityIJRASETPublicationsNo ratings yet
- ASEPTIC FILL CLEANING VALIDATIONDocument9 pagesASEPTIC FILL CLEANING VALIDATIONangel vencesNo ratings yet
- ABC VW24A CatsalogueDocument2 pagesABC VW24A CatsalogueKeith Ivan Ong MeridoresNo ratings yet
- Sabnis 2014Document8 pagesSabnis 2014Lobo CalupohNo ratings yet
- IVT Network - Sanitization of Pharmaceutical Facilities - 2014-08-29Document7 pagesIVT Network - Sanitization of Pharmaceutical Facilities - 2014-08-29Bhagath VikasNo ratings yet
- Cleanroom Technology: Fundamentals of Design, Testing and OperationFrom EverandCleanroom Technology: Fundamentals of Design, Testing and OperationNo ratings yet
- Basic Guide to Infection Prevention and Control in DentistryFrom EverandBasic Guide to Infection Prevention and Control in DentistryNo ratings yet
- Self-Cleaning Materials and Surfaces: A Nanotechnology ApproachFrom EverandSelf-Cleaning Materials and Surfaces: A Nanotechnology ApproachWalid A. DaoudRating: 5 out of 5 stars5/5 (1)
- Exposure Assessment and Safety Considerations for Working with Engineered NanoparticlesFrom EverandExposure Assessment and Safety Considerations for Working with Engineered NanoparticlesNo ratings yet
- Arcomed Syramed uSP6000 - Manual Mantencion PDFDocument43 pagesArcomed Syramed uSP6000 - Manual Mantencion PDFpirihuey1234No ratings yet
- Heat Sealer Repair and Maintenance Kit IFU 2019-02-06Document27 pagesHeat Sealer Repair and Maintenance Kit IFU 2019-02-06LowayNo ratings yet
- instrukcija СО 7Document23 pagesinstrukcija СО 7LowayNo ratings yet
- SE 1200 Operators ManualDocument103 pagesSE 1200 Operators ManualNikolay PenevNo ratings yet
- Hemocue WBC Diff: Operating ManualDocument84 pagesHemocue WBC Diff: Operating ManualLowayNo ratings yet
- Polaris 600Document96 pagesPolaris 600LowayNo ratings yet
- Hiperfet Power Mosfets: Ixfh14N80 Ixfh15N80Document6 pagesHiperfet Power Mosfets: Ixfh14N80 Ixfh15N80LowayNo ratings yet
- lm2595 PDFDocument42 pageslm2595 PDFMartin SaraviaNo ratings yet
- Low Voltage Generator Thesis Provides Insight into Charging Storage BatteriesDocument38 pagesLow Voltage Generator Thesis Provides Insight into Charging Storage BatteriesLowayNo ratings yet
- SkupDocument95 pagesSkupLowayNo ratings yet
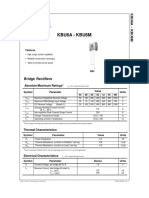
- PDF KBU6A-KBU6M FairchildDocument3 pagesPDF KBU6A-KBU6M FairchildLowayNo ratings yet
- Ds - Tlsr8261-E - Datasheet For Telink Ble Soc Tlsr8261Document106 pagesDs - Tlsr8261-E - Datasheet For Telink Ble Soc Tlsr8261LowayNo ratings yet
- FSN Monitor - FS-P2601D-User-GuideDocument48 pagesFSN Monitor - FS-P2601D-User-GuideLowayNo ratings yet
- IMT Bellavista 1000 Ventilator - Service Manual PDFDocument94 pagesIMT Bellavista 1000 Ventilator - Service Manual PDFecarrera1975No ratings yet
- Aun Perfusor Space - Service ManualDocument132 pagesAun Perfusor Space - Service ManualMursal MursalzadeNo ratings yet
- Sensors: Design of An Oximeter Based On LED-LED Configuration and FPGA TechnologyDocument13 pagesSensors: Design of An Oximeter Based On LED-LED Configuration and FPGA TechnologyShanny SantosNo ratings yet
- Acculan 3ti Ga677Document146 pagesAcculan 3ti Ga677LowayNo ratings yet
- Real Time Joint Resistance Monitoring During Solder Re FlowDocument10 pagesReal Time Joint Resistance Monitoring During Solder Re FlowLowayNo ratings yet
- GE Eagle 4000 - Service ManualDocument226 pagesGE Eagle 4000 - Service ManualFernando AlonsoNo ratings yet
- Central data management for EMG and EEGDocument10 pagesCentral data management for EMG and EEGLowayNo ratings yet
- Piezoelectric Properties Dry Human SkinDocument7 pagesPiezoelectric Properties Dry Human SkinLowayNo ratings yet
- Aun Perfusor FM - Service ManualDocument88 pagesAun Perfusor FM - Service ManualBruno Gonçalves Lima GomesNo ratings yet
- Aun Perfusor Space - Service ManualDocument132 pagesAun Perfusor Space - Service ManualMursal MursalzadeNo ratings yet
- Bioimpedance Measurement System For Smart ClothingDocument10 pagesBioimpedance Measurement System For Smart ClothingLowayNo ratings yet
- Marquette Eagle1000 - Service ManualDocument148 pagesMarquette Eagle1000 - Service ManualfpanciNo ratings yet
- Nellcor N395 User ManualDocument110 pagesNellcor N395 User ManualLowayNo ratings yet
- Biel 006 PDFDocument3 pagesBiel 006 PDFrohanNo ratings yet
- Bally 5500 SetUpandOperationDocument34 pagesBally 5500 SetUpandOperationFreder AngelNo ratings yet
- Exocytosis and Endocytosis: © 2012 Pearson Education, IncDocument49 pagesExocytosis and Endocytosis: © 2012 Pearson Education, IncGlein CenizaNo ratings yet
- YSCA Brochure22 York Pared Con SEER 10Document2 pagesYSCA Brochure22 York Pared Con SEER 10san cadejoNo ratings yet
- INMATEH-Agricultural Engineering Vol.42 - 2014Document175 pagesINMATEH-Agricultural Engineering Vol.42 - 2014Popa LucretiaNo ratings yet
- GHDL Latest PDFDocument111 pagesGHDL Latest PDFArpanNo ratings yet
- Oracle OLTP (Transactional) Load Testing: Quick Start TutorialDocument68 pagesOracle OLTP (Transactional) Load Testing: Quick Start TutorialVenki ReddyNo ratings yet
- Good Practice Guide For Form and Diameter Measurements For Large ShaftsDocument14 pagesGood Practice Guide For Form and Diameter Measurements For Large ShaftsNg Wei LihNo ratings yet
- AGE Site Core Cutting DataDocument1 pageAGE Site Core Cutting Dataaashish patidarNo ratings yet
- Rectangular Tank Calculation Roarks FormulasDocument39 pagesRectangular Tank Calculation Roarks FormulasInamullah Khan100% (3)
- SC-9790AV SX-9790: Service ManualDocument80 pagesSC-9790AV SX-9790: Service ManualBRAULIO GARCIA SANTIAGONo ratings yet
- MAS TEST With AnswerDocument10 pagesMAS TEST With Answerjoneth.duenasNo ratings yet
- Overview of Algorithms For Swarm Intelligence PDFDocument14 pagesOverview of Algorithms For Swarm Intelligence PDFmenguemengueNo ratings yet
- EED 5 Unit 8Document45 pagesEED 5 Unit 8Reinaliza FerraroNo ratings yet
- Instrument Note RangesDocument11 pagesInstrument Note RangesWalter Macasiano GravadorNo ratings yet
- Mathematical Conversations To Transform Algebra ClassDocument9 pagesMathematical Conversations To Transform Algebra ClassSyamil AlliyusNo ratings yet
- Date ValidationDocument9 pagesDate ValidationAnonymous 9B0VdTWiNo ratings yet
- S - 1.3 E A Big "O" Truncation Error: O (H) Order of ApproximationDocument5 pagesS - 1.3 E A Big "O" Truncation Error: O (H) Order of ApproximationMohammed SalahNo ratings yet
- SE1Document5 pagesSE1AlexisNo ratings yet
- 1st Q Math 10Document2 pages1st Q Math 10Mari Zechnas Osnola100% (1)
- Getting Started with Python for Data ScienceDocument5 pagesGetting Started with Python for Data ScienceAkhi DanuNo ratings yet
- Instruction Sheet 579 163: Simulation ABS/Ti, STE 2/50Document1 pageInstruction Sheet 579 163: Simulation ABS/Ti, STE 2/50Billel TalbiNo ratings yet
- BS499 PDFDocument36 pagesBS499 PDFnisha_khanNo ratings yet
- Readme LADSPA Plugins-WinDocument2 pagesReadme LADSPA Plugins-WineduhideoNo ratings yet
- Oil Families in Canadian Williston Basin (Southwestern Saskatchewan) - Osadetz, Snowdon, Brooks - (42, 155-177) - (1994) - PAPERDocument24 pagesOil Families in Canadian Williston Basin (Southwestern Saskatchewan) - Osadetz, Snowdon, Brooks - (42, 155-177) - (1994) - PAPERVitor8AzevedoNo ratings yet
- TriGem CognacDocument29 pagesTriGem CognacfostechNo ratings yet
- Chapter 4-Piezoelectric CeramicsDocument33 pagesChapter 4-Piezoelectric Ceramicssantsex111No ratings yet
- ADU451816 V 01Document2 pagesADU451816 V 01Daniel Manole67% (3)