You might also like
- To EDIT GRAPH CSPMAP - PIR Presentation (Rizal Medical Center) 2023Document29 pagesTo EDIT GRAPH CSPMAP - PIR Presentation (Rizal Medical Center) 2023Oncology PharmacyNo ratings yet
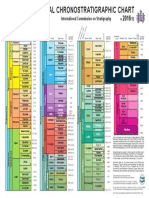
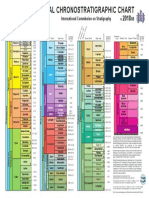
- ChronostratChart2017 02Document1 pageChronostratChart2017 02ross182No ratings yet
- Ilovepdf MergedDocument460 pagesIlovepdf MergedDoğukan ÖzbirinciNo ratings yet
- Graduation Thesis Strategizing A TransitDocument158 pagesGraduation Thesis Strategizing A TransitKurdeen KhairyNo ratings yet
- Endotracheal Tube Cuffs:: Design and FunctionDocument8 pagesEndotracheal Tube Cuffs:: Design and FunctionmochkurniawanNo ratings yet
- PhlebotomyDocument46 pagesPhlebotomyQaiser ZamanNo ratings yet
- HerniaDocument16 pagesHerniamuhammad akbarNo ratings yet
- ChronostratChart2016 12 PDFDocument1 pageChronostratChart2016 12 PDFgimenezNo ratings yet
- Erosao DIetschi 2011 n89aoR-ContentServer - AspDocument15 pagesErosao DIetschi 2011 n89aoR-ContentServer - AspPedroCruzNo ratings yet
- TimelineDocument1 pageTimelinemclaughaNo ratings yet
- PF - Kia - Polindes - Polindes 7Document213 pagesPF - Kia - Polindes - Polindes 7Nurdianty FauziahNo ratings yet
- Engaged Scholarship: A Guide For Organizational and Social ResearchDocument39 pagesEngaged Scholarship: A Guide For Organizational and Social ResearchImelda HotmariaNo ratings yet
- Mditi M Mediating Messages With Mediator ComponentsDocument36 pagesMditi M Mediating Messages With Mediator ComponentsghazouanikarimNo ratings yet
- International Chronostratigraphic Chart 2016Document1 pageInternational Chronostratigraphic Chart 2016Diego Ardila100% (1)
- TmeineDocument1 pageTmeinemclaughaNo ratings yet
- Extubation - Making Safer PDFDocument6 pagesExtubation - Making Safer PDFUlises Herrera SotoNo ratings yet
- International Chronosgraphic Trat Chart PDFDocument1 pageInternational Chronosgraphic Trat Chart PDFLara CitlalliNo ratings yet
- SeminaireIREENA 20180408Document49 pagesSeminaireIREENA 20180408sarraHouidiNo ratings yet
- Dashboard Penyel KIA PuskesmasDocument225 pagesDashboard Penyel KIA PuskesmasNurdianty FauziahNo ratings yet
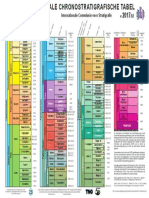
- ChronostratChart2017 02NLDutchDocument1 pageChronostratChart2017 02NLDutchDafne Ramírez MendozaNo ratings yet
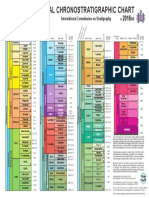
- ChronostratChart2018 07Document1 pageChronostratChart2018 07Gerardo GonzálezNo ratings yet
- PF - Kia - Kabbandung - PKM 12 SantosaDocument225 pagesPF - Kia - Kabbandung - PKM 12 SantosaNurdianty FauziahNo ratings yet
- Tema 2 - Ejed - 1 - 1 - Fradeani - 6Document8 pagesTema 2 - Ejed - 1 - 1 - Fradeani - 6tiberijNo ratings yet
- PF - Kia - Kabbandung - PKM 9 SukamanahDocument225 pagesPF - Kia - Kabbandung - PKM 9 SukamanahNurdianty FauziahNo ratings yet
- PF - Kia - Kabbandung - PKM 27 CikaroDocument225 pagesPF - Kia - Kabbandung - PKM 27 CikaroNurdianty FauziahNo ratings yet
- FOCUSED OBSERVATIONS Child's Name: - : Forms Committee 07/10Document41 pagesFOCUSED OBSERVATIONS Child's Name: - : Forms Committee 07/10sharpgypsyNo ratings yet
- 03 - Modified Grassline Technique For Orthodontic Space ClosureDocument22 pages03 - Modified Grassline Technique For Orthodontic Space ClosureAurelian DentistNo ratings yet
- PET 720 Reservoir Characterisation MethodsDocument32 pagesPET 720 Reservoir Characterisation MethodsMiguelNo ratings yet
- Oxygen Ontents - Reading - ExcerptDocument23 pagesOxygen Ontents - Reading - ExcerptBabli Lovely Nicky100% (1)
- Colorful Lamp Strategy Model Mind Map BrainstormDocument1 pageColorful Lamp Strategy Model Mind Map BrainstormmarcusluismacusiNo ratings yet
- Kemahiran Proses SainsDocument4 pagesKemahiran Proses SainsNOREDAWATI BINTI MAHFUDZ KPM-GuruNo ratings yet
- International Chronostratigraphic Chart: International Commission On Stratigraphy V /08Document1 pageInternational Chronostratigraphic Chart: International Commission On Stratigraphy V /08Leonardo Xavier DornelasNo ratings yet
- International Chronostratigraphic Chart: International Commission On Stratigraphy V /08Document1 pageInternational Chronostratigraphic Chart: International Commission On Stratigraphy V /08Inngry GutiéérrezNo ratings yet
- Clear Mutual Expectations RefresherDocument10 pagesClear Mutual Expectations RefresherInstalasi RehabilitasiNo ratings yet
- Describing Bar Chart Practice 3Document7 pagesDescribing Bar Chart Practice 3Irfan HasifNo ratings yet
- Lip SupportDocument9 pagesLip SupportFrancisco Antonio Vargas GuevaraNo ratings yet
- Optimizing Smile Composition and Esthetics With Resin Composites and Other Conservative Esthetic ProceduresDocument16 pagesOptimizing Smile Composition and Esthetics With Resin Composites and Other Conservative Esthetic ProceduresTiagoNo ratings yet
- 30th Sept Protest - PosterDocument1 page30th Sept Protest - PosteredenmorecdpNo ratings yet
- 2022 11 16 RCC Enhanced Brochure FINAL V6Document21 pages2022 11 16 RCC Enhanced Brochure FINAL V6Darren ChenNo ratings yet
- Women Rights 2018Document49 pagesWomen Rights 2018Saba JaianiNo ratings yet
- Full-Mouth Adhesive Rehabilitation of A Severely Eroded Dentition: The Three-Step Technique. Part 2Document17 pagesFull-Mouth Adhesive Rehabilitation of A Severely Eroded Dentition: The Three-Step Technique. Part 2Karina OjedaNo ratings yet
- WMC 2016 Prospectus June 2016 PDFDocument87 pagesWMC 2016 Prospectus June 2016 PDFAnonymous 0gfzLMYYfXNo ratings yet
- Next Generation CR and Sustainability Jobs - 2017Document10 pagesNext Generation CR and Sustainability Jobs - 2017Ghadeer MohammedNo ratings yet
- El Amal Hospital Manpower ServicesDocument1 pageEl Amal Hospital Manpower Servicesإبرآهيم محمدNo ratings yet
- Exercise 1: Looking For Information at SpeedDocument17 pagesExercise 1: Looking For Information at SpeedtruongthikhaNo ratings yet
- Biomimcry KitesDocument1 pageBiomimcry Kitesvibha bNo ratings yet
- Prathapraj UX - Consultant Design PortfolioDocument25 pagesPrathapraj UX - Consultant Design PortfolioprathaprajNo ratings yet
- 1 NI IntroductionDocument23 pages1 NI IntroductionbunsokoyNo ratings yet
- 09 - Jacoby, Alison - Adolescent GynecologyDocument60 pages09 - Jacoby, Alison - Adolescent GynecologyscotNo ratings yet
- Final Ideal Clinic Framework - Version 17 On 3 Aug 2017Document92 pagesFinal Ideal Clinic Framework - Version 17 On 3 Aug 2017Finger TladiNo ratings yet
- Orgl 3321 Dddmi ArtifactDocument5 pagesOrgl 3321 Dddmi Artifactapi-673975467No ratings yet
- Palatal and Facial Veneers To Treat Severe DentalDocument12 pagesPalatal and Facial Veneers To Treat Severe DentalBrenda Patricia Ruiz GodinezNo ratings yet
- Summary I - Fraud Circulator TotalsDocument1 pageSummary I - Fraud Circulator Totalsaaronc2484No ratings yet
- Arietta 65Document7 pagesArietta 65Juan VillamizarNo ratings yet
- Data Presentation and InterpretationDocument9 pagesData Presentation and InterpretationClarisse PlatonNo ratings yet
- SEM05 - Montero - Mind MapDocument1 pageSEM05 - Montero - Mind MapReysel MonteroNo ratings yet
- wachtel2006 19655501Document12 pageswachtel2006 19655501André Pinheiro de AraújoNo ratings yet
- It's So Easy Going Green: An Interactive, Scientific Look at Protecting Our EnvironmentFrom EverandIt's So Easy Going Green: An Interactive, Scientific Look at Protecting Our EnvironmentNo ratings yet
- From the Midwife's Bag to the Patient's File: Public Health in Eastern and Southeastern EuropeFrom EverandFrom the Midwife's Bag to the Patient's File: Public Health in Eastern and Southeastern EuropeNo ratings yet
- Cervical Cancer Prevention & Management of Pre-Malignant LesionsDocument41 pagesCervical Cancer Prevention & Management of Pre-Malignant LesionsMichaelNo ratings yet
- ICI Course - Prostate Cancer EpidemiologyDocument19 pagesICI Course - Prostate Cancer EpidemiologyMichaelNo ratings yet
- Gu MDT: Virtual Tumour Board PresentationDocument12 pagesGu MDT: Virtual Tumour Board PresentationMichaelNo ratings yet
- Concept and PSS - ILCCDocument34 pagesConcept and PSS - ILCCMichaelNo ratings yet
- Supportive, Palliative Care & Survivorship in Prostate Cancer ICI April 2022 ZADocument39 pagesSupportive, Palliative Care & Survivorship in Prostate Cancer ICI April 2022 ZAMichaelNo ratings yet
- Results Framework and Logframe - 13th - October 2020Document37 pagesResults Framework and Logframe - 13th - October 2020MichaelNo ratings yet
- Presented By: Musyoki David: Kenya Hospices and Palliative Care AssociationDocument34 pagesPresented By: Musyoki David: Kenya Hospices and Palliative Care AssociationMichaelNo ratings yet
- Locaaly Advanced Cervical CancerDocument50 pagesLocaaly Advanced Cervical CancerMichaelNo ratings yet
- Antineoplastics: CCC100: Administration Competency CourseDocument48 pagesAntineoplastics: CCC100: Administration Competency CourseMichaelNo ratings yet
- NK/T Cell Lymphoma Case PresentationDocument14 pagesNK/T Cell Lymphoma Case PresentationMichaelNo ratings yet
- Role of Pet-Ct in Management of LymphomaDocument45 pagesRole of Pet-Ct in Management of LymphomaMichaelNo ratings yet
- Queries in EmergenciesDocument1 pageQueries in EmergenciesMichaelNo ratings yet
- Effective Communication Styles - ICI August 2020Document37 pagesEffective Communication Styles - ICI August 2020Michael100% (1)
- Queries in EmergenciesDocument1 pageQueries in EmergenciesMichaelNo ratings yet
- Palliative Care (PC) EmergenciesDocument31 pagesPalliative Care (PC) EmergenciesMichaelNo ratings yet
- Palliative Care (PC) EmergenciesDocument31 pagesPalliative Care (PC) EmergenciesMichaelNo ratings yet
- Nutrition and Diet Therapy: Classification of Essential NutrientsDocument66 pagesNutrition and Diet Therapy: Classification of Essential NutrientsChristine Joy Molina100% (1)
- Pediatric Nursing 300 With RationaleDocument65 pagesPediatric Nursing 300 With RationaleXer AlliuqNo ratings yet
- Gynecological Oncology PDFDocument226 pagesGynecological Oncology PDFlula gestiana taufanNo ratings yet
- Celiac DiseaseDocument35 pagesCeliac DiseaseRye HanaNo ratings yet
- Unit - 3 Level of PreventionDocument26 pagesUnit - 3 Level of Preventionmoges lakeNo ratings yet
- Calorie Burn and Weight Loss Guidelines from ExerciseDocument4 pagesCalorie Burn and Weight Loss Guidelines from ExerciseHansen LouistherNo ratings yet
- General Appraisal Overview (GAO) For All Studies : British Journal of Occupational Therapy, 74 (11), 517-524Document3 pagesGeneral Appraisal Overview (GAO) For All Studies : British Journal of Occupational Therapy, 74 (11), 517-524Heather CunninghamNo ratings yet
- NCP MeningitisDocument4 pagesNCP MeningitisMa. Gina DerlaNo ratings yet
- Medicine - BhanuDocument469 pagesMedicine - BhanuHIMAVARADHAN UNo ratings yet
- Art Therapy and Neuroscience Blend: Working With Patients Who Have DementiaDocument8 pagesArt Therapy and Neuroscience Blend: Working With Patients Who Have DementiaLiliana Duarte PedrozaNo ratings yet
- Complete Blood Count (CBC) Test: WBC DifferentialDocument4 pagesComplete Blood Count (CBC) Test: WBC Differentialchang02No ratings yet
- Black Death in AsiaDocument3 pagesBlack Death in Asiaapi-286657372No ratings yet
- University of Health and Allied Sciences School of Public HealthDocument12 pagesUniversity of Health and Allied Sciences School of Public HealthWillis ITNo ratings yet
- Sources of Epidemiological Data BoazDocument4 pagesSources of Epidemiological Data Boazgeorgeloto1288% (8)
- Asparaginase / Erwinia AsparaginaseDocument10 pagesAsparaginase / Erwinia AsparaginaseMohammed HaiderNo ratings yet
- PNHIS - Treatment - Hospital List - 20210430143954 - 71540Document115 pagesPNHIS - Treatment - Hospital List - 20210430143954 - 71540sugunec2013No ratings yet
- Lung Ca Case Presentation PDFDocument28 pagesLung Ca Case Presentation PDFapi-276417422100% (2)
- ThyrotoxicosissumiDocument24 pagesThyrotoxicosissumidrcumee0% (1)
- Concept of disease MCQs فراسDocument5 pagesConcept of disease MCQs فراسHisokagenNo ratings yet
- Science Year 5: MicroorganismsDocument8 pagesScience Year 5: MicroorganismscthanifahNo ratings yet
- Emotional DisturbanceDocument37 pagesEmotional DisturbanceAngelo MirabelNo ratings yet
- Pediatric Infectious Diseases. Vaccination ProgramsDocument44 pagesPediatric Infectious Diseases. Vaccination ProgramsShubhra PaulNo ratings yet
- Group 2 - Vitamins LaboratoryDocument6 pagesGroup 2 - Vitamins LaboratorySophia BiacoNo ratings yet
- Nursing Health History /nursing Process/Physical AsessmentDocument2 pagesNursing Health History /nursing Process/Physical AsessmentKaye CorNo ratings yet
- Malaria ProjectDocument45 pagesMalaria ProjectNikhilNo ratings yet
- Passage 1-Acquired Immune Deficiency SyndromeDocument3 pagesPassage 1-Acquired Immune Deficiency SyndromeWasik ShaheerNo ratings yet
- Here are the answers to the exercises:1. a. Ridwan visits his grandfather every month.2. The students always play card in the living room every eveningDocument37 pagesHere are the answers to the exercises:1. a. Ridwan visits his grandfather every month.2. The students always play card in the living room every eveningAjeng Afriliana75% (4)
- Gut and Psychology Syndrome (GAPS) - Weston A Price Foundation"Document13 pagesGut and Psychology Syndrome (GAPS) - Weston A Price Foundation"shadhilidarqawi75% (4)
- Postural DrainageDocument7 pagesPostural DrainagemohtishimNo ratings yet
- DNB Gen Surgery Old Question Papers 1Document28 pagesDNB Gen Surgery Old Question Papers 1sidorai100% (1)