You might also like
- Ethanol and IsopropanolDocument15 pagesEthanol and IsopropanolmsofiaemberNo ratings yet
- Synergistic Effects of Anionic Surfactants On Coronavirus (Sars-Cov-2) Virucidal Efficiency of Sanitizing Fluids To Fight Covid-19Document8 pagesSynergistic Effects of Anionic Surfactants On Coronavirus (Sars-Cov-2) Virucidal Efficiency of Sanitizing Fluids To Fight Covid-19Alicia PerezNo ratings yet
- JMV 25666Document5 pagesJMV 25666Nathalia LedesmaNo ratings yet
- Effects of Whole Cigarette Smoke On Human Beta Defensins Expression and Secretion by Oral Mucosal Epithelial CellsDocument10 pagesEffects of Whole Cigarette Smoke On Human Beta Defensins Expression and Secretion by Oral Mucosal Epithelial CellsMirela TomaNo ratings yet
- Lung Explant With Sars Cov 2Document10 pagesLung Explant With Sars Cov 2Ping LiuNo ratings yet
- Potential Role of Oral Rinses Targeting The Viral Lipid Zqaa002 COMPLETODocument12 pagesPotential Role of Oral Rinses Targeting The Viral Lipid Zqaa002 COMPLETODallas Juan Tarco SumireNo ratings yet
- The Ability of Two Chlorine Dioxide Chemistries To Inactivate Human Papillomavirus-Contaminated Endocavitary Ultrasound Probes and NasendoscopesDocument11 pagesThe Ability of Two Chlorine Dioxide Chemistries To Inactivate Human Papillomavirus-Contaminated Endocavitary Ultrasound Probes and NasendoscopesNathalia LedesmaNo ratings yet
- Analysis of The Anti-Viral Potential of Nasal Spray Constituents AgainstDocument16 pagesAnalysis of The Anti-Viral Potential of Nasal Spray Constituents AgainstLes BennettNo ratings yet
- Journal Pre-Proof: Trends in Plant ScienceDocument17 pagesJournal Pre-Proof: Trends in Plant ScienceMUGDHA MITTALNo ratings yet
- EnumerationandidentificationofentericandpseudomonadDocument15 pagesEnumerationandidentificationofentericandpseudomonadHafsaAliNo ratings yet
- Artigo PreditivaDocument5 pagesArtigo Preditivalarissamirellemm2No ratings yet
- Estudio Corona 1 Ropa41-7-E67Document5 pagesEstudio Corona 1 Ropa41-7-E67eudaldoNo ratings yet
- Biorxiv Infection of Human Lung Tissue SARSCoV2Document28 pagesBiorxiv Infection of Human Lung Tissue SARSCoV2Ping LiuNo ratings yet
- Candida Albicans Biofilm InhibitorsDocument7 pagesCandida Albicans Biofilm InhibitorsSenuke TestNo ratings yet
- Beneficial Effects of A Mouthwash Containing An Antiviral Phthalocyanine Derivative On The Length of Hospital Stay For COVID 19: Randomised TrialDocument10 pagesBeneficial Effects of A Mouthwash Containing An Antiviral Phthalocyanine Derivative On The Length of Hospital Stay For COVID 19: Randomised TrialtvinteNo ratings yet
- PESQUISA FIOCRUZ COVID - 2020.04.04.020925v2.fullDocument28 pagesPESQUISA FIOCRUZ COVID - 2020.04.04.020925v2.fullMaressa OmenaNo ratings yet
- Jwas 12589Document18 pagesJwas 12589WAPARAFOL100% (1)
- Disinfection Box Chamber Tunnel Booth Partition Gate To Reduce Transmision of COVID-19Document12 pagesDisinfection Box Chamber Tunnel Booth Partition Gate To Reduce Transmision of COVID-19kinzaNo ratings yet
- Development and Validation of A High-Throughput Screen For Inhibitors of Sars Cov and Its Application in Screening of A 100,000-Compound LibraryDocument8 pagesDevelopment and Validation of A High-Throughput Screen For Inhibitors of Sars Cov and Its Application in Screening of A 100,000-Compound LibraryRadenNo ratings yet
- Raposo 2014Document8 pagesRaposo 2014Anonymous Wcj4C3jNo ratings yet
- Food Microbiology: Alexander Rohde, Jens Andre Hammerl, Bernd Appel, Ralf Dieckmann, Sascha Al DahoukDocument13 pagesFood Microbiology: Alexander Rohde, Jens Andre Hammerl, Bernd Appel, Ralf Dieckmann, Sascha Al DahoukMihail AvramovNo ratings yet
- MainDocument7 pagesMainlps DiamondNo ratings yet
- Antibiotics in The EnvironmentDocument6 pagesAntibiotics in The Environmentjacksparrow7425No ratings yet
- Ultraviolet Disinfection With A Novel Microwave-Powered DeviceDocument9 pagesUltraviolet Disinfection With A Novel Microwave-Powered Devicebarby17_2005No ratings yet
- Virucidal Eficacia de Enjuagatorios Orales COMPLETO JOURNALDocument4 pagesVirucidal Eficacia de Enjuagatorios Orales COMPLETO JOURNALDallas Juan Tarco SumireNo ratings yet
- The Hyperlipidaemic Drug Fenofibrate SignificantlyDocument35 pagesThe Hyperlipidaemic Drug Fenofibrate SignificantlyJack NixonNo ratings yet
- The Effect of Temperature On Persistence of Sars-Cov-2 On Common SurfacesDocument7 pagesThe Effect of Temperature On Persistence of Sars-Cov-2 On Common SurfacesManglam GuptaNo ratings yet
- Bepridil Is Potent Against SARS-CoV-2 in VitroDocument28 pagesBepridil Is Potent Against SARS-CoV-2 in VitrosovalaxNo ratings yet
- 1 s2.0 S0168160523002593 MainDocument9 pages1 s2.0 S0168160523002593 MainsartikajuliaanugrahNo ratings yet
- Inhalation of A Fog of Hypochlorous Acid (Hocl) : Biochemical, Antimicrobial, and Pathological AssessmentDocument17 pagesInhalation of A Fog of Hypochlorous Acid (Hocl) : Biochemical, Antimicrobial, and Pathological AssessmentAngeles SuarezNo ratings yet
- Potential Antiviral Properties of Bioactive Constitents and Phytochemicals From Selected Plants Against SARSDocument118 pagesPotential Antiviral Properties of Bioactive Constitents and Phytochemicals From Selected Plants Against SARSRamil LucasNo ratings yet
- The Role of Chemistry in Sanitization and Personal Hygiene in Context of Covid-19Document8 pagesThe Role of Chemistry in Sanitization and Personal Hygiene in Context of Covid-19Central Asian StudiesNo ratings yet
- The Action of Three Antiseptics/disinfectants Against Enveloped and Non-Enveloped VirusesDocument13 pagesThe Action of Three Antiseptics/disinfectants Against Enveloped and Non-Enveloped VirusesTrần Minh TríNo ratings yet
- Ogorzaly Et Al 2013 - Two-Day Detection of Infectious Enteric and Non-Enteric Adenoviruses by Improved ICC-qPCRDocument9 pagesOgorzaly Et Al 2013 - Two-Day Detection of Infectious Enteric and Non-Enteric Adenoviruses by Improved ICC-qPCRYoNo ratings yet
- SporeDocument8 pagesSporepedroloxxxNo ratings yet
- Povidone-Iodine Use in Sinonasal and Oral CavitiesDocument8 pagesPovidone-Iodine Use in Sinonasal and Oral CavitiesTulio Reis HannasNo ratings yet
- Hypochlorous Acid COVID ReviewDocument6 pagesHypochlorous Acid COVID ReviewEnvirolyte Solutions InternationalNo ratings yet
- Pretreatment To Avoid Positive RT-PCR Results With Inactivated VirusesDocument9 pagesPretreatment To Avoid Positive RT-PCR Results With Inactivated VirusesNori PurnamaNo ratings yet
- Detection of Viruses in Used Ventilation Filters From Two Large Public BuildingsDocument9 pagesDetection of Viruses in Used Ventilation Filters From Two Large Public BuildingsbaridinoNo ratings yet
- Health Hazards of Mosquito Repellents and Safe AlternativesDocument3 pagesHealth Hazards of Mosquito Repellents and Safe AlternativesIshan RathoreNo ratings yet
- CovidDocument8 pagesCovidYamil Sacin ReydeCastroNo ratings yet
- Acetic Acid Disinfection As A Potential Adjunctive Therapy For Non Severe COVID 19Document4 pagesAcetic Acid Disinfection As A Potential Adjunctive Therapy For Non Severe COVID 19Intan AyuNo ratings yet
- Vacuum Aerosol 6Document7 pagesVacuum Aerosol 6khamilatusyNo ratings yet
- Rasberries FreshDocument9 pagesRasberries FreshKarla GNo ratings yet
- Animal AnalogDocument10 pagesAnimal Analograhul392410No ratings yet
- 2020 JAPR Hernández YcolsDocument15 pages2020 JAPR Hernández YcolsJavier RamirezNo ratings yet
- 2015 The Authors. Food Science & Nutrition Published by Wiley Periodicals, Inc.Document12 pages2015 The Authors. Food Science & Nutrition Published by Wiley Periodicals, Inc.ТатьянаNo ratings yet
- Study of The Efficacy and Safety of Topical Ivermectin + Iota-Carrageenan in The Prophylaxis Against COVID-19 in Health PersonnelDocument6 pagesStudy of The Efficacy and Safety of Topical Ivermectin + Iota-Carrageenan in The Prophylaxis Against COVID-19 in Health PersonnelKaroline MarxNo ratings yet
- Executive Summary: Exposure To DEHPDocument6 pagesExecutive Summary: Exposure To DEHPsinglethienNo ratings yet
- A Pragmatic Multicenter, Randomized, Double-Blind, Placebo-Controlled TrialDocument21 pagesA Pragmatic Multicenter, Randomized, Double-Blind, Placebo-Controlled TrialHidalgo Primo InmobiliariaNo ratings yet
- Penicillium 8 Pag.Document11 pagesPenicillium 8 Pag.Jorge Raul VilcaNo ratings yet
- Wang 2015Document7 pagesWang 2015Sebastian MilesNo ratings yet
- Chlorine Inactivation of Highly Pathogenic Avian Infl Uenza Virus (H5N1)Document3 pagesChlorine Inactivation of Highly Pathogenic Avian Infl Uenza Virus (H5N1)Rahul SahuNo ratings yet
- Jam 13361Document6 pagesJam 13361Melissa SchulthessNo ratings yet
- Lesiones Orales Covid19Document7 pagesLesiones Orales Covid19Diana PerezNo ratings yet
- 2020 Troeltzschbrothers Covid-19 EngDocument6 pages2020 Troeltzschbrothers Covid-19 Engdamsia-1No ratings yet
- 10 1016@j Ijantimicag 2020 105923Document6 pages10 1016@j Ijantimicag 2020 105923Basilio Papuico RomeroNo ratings yet
- Kusum D.V., Bhosale U.V. - Formulation and Optimization of Polymeric Nano Drug Delivery System of Acyclovir Using 3 (2) Full Factorial DesignDocument10 pagesKusum D.V., Bhosale U.V. - Formulation and Optimization of Polymeric Nano Drug Delivery System of Acyclovir Using 3 (2) Full Factorial DesignJordy CanalesNo ratings yet
- Original Research: COVID-19 Global Pandemic Planning: Decontamination and Reuse Processes For N95 RespiratorsDocument7 pagesOriginal Research: COVID-19 Global Pandemic Planning: Decontamination and Reuse Processes For N95 RespiratorscrisNo ratings yet
- Jurnal Nonylphenol EthoxylateDocument13 pagesJurnal Nonylphenol EthoxylateWerstant Adhityananda RNo ratings yet
- Journal Pre-Proof: Journal of Hospital InfectionDocument14 pagesJournal Pre-Proof: Journal of Hospital InfectionWerstant Adhityananda RNo ratings yet
- 594 1901 5 PB PDFDocument6 pages594 1901 5 PB PDFAlmarchiano SandiNo ratings yet
- Russell 2002Document4 pagesRussell 2002Werstant Adhityananda RNo ratings yet
- MJM-18-0035 FinalisedDocument7 pagesMJM-18-0035 FinalisedWerstant Adhityananda RNo ratings yet
- Journal Pre-Proofs: Food Research InternationalDocument38 pagesJournal Pre-Proofs: Food Research InternationalWerstant Adhityananda RNo ratings yet
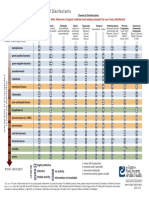
- The Antimicrobial Spectrum of Disinfectants: Most SusceptibleDocument1 pageThe Antimicrobial Spectrum of Disinfectants: Most SusceptibleWerstant Adhityananda RNo ratings yet
- The Scientific Basis of Lactobacillus AcidophilusDocument13 pagesThe Scientific Basis of Lactobacillus AcidophilussrihastutiNo ratings yet
- The Vitamin B Complex: Chemists and Chemistry That Transformed Our LivesDocument4 pagesThe Vitamin B Complex: Chemists and Chemistry That Transformed Our LivesWerstant Adhityananda RNo ratings yet
- Seleksi Dan Identifikasi Lactobacillus Kandidat Probiotik Penurun Kolesterol Berdasarkan Analisis Sekuen 16s RnaDocument6 pagesSeleksi Dan Identifikasi Lactobacillus Kandidat Probiotik Penurun Kolesterol Berdasarkan Analisis Sekuen 16s RnaWerstant Adhityananda RNo ratings yet
- Investigation of Acute Toxicity of Deltamethrin On Guppies (Poecilia Reticulata)Document4 pagesInvestigation of Acute Toxicity of Deltamethrin On Guppies (Poecilia Reticulata)Werstant Adhityananda RNo ratings yet
- Deltamethrin 3Document8 pagesDeltamethrin 3Werstant Adhityananda RNo ratings yet
- Toxicokinetics of Deltamethrin and Its 4'-HO-Metabolite in The RatDocument9 pagesToxicokinetics of Deltamethrin and Its 4'-HO-Metabolite in The RatWerstant Adhityananda RNo ratings yet
- Solubilities of Magnesium Sulfite: J. NývltDocument4 pagesSolubilities of Magnesium Sulfite: J. NývltWerstant Adhityananda RNo ratings yet
- Ecosterile Plus LiteratureDocument4 pagesEcosterile Plus LiteratureChetan GajjarNo ratings yet
- Lynal: Tissue Conditioner & Temporary RelinerDocument2 pagesLynal: Tissue Conditioner & Temporary RelinerGonzalo Urrutia ElsoNo ratings yet
- The Testing of DisinfectantsDocument4 pagesThe Testing of DisinfectantsalejandraNo ratings yet
- FOLDER Gesamt Hospital ENG 2105 SCREEN LOW Brosch PDFDocument74 pagesFOLDER Gesamt Hospital ENG 2105 SCREEN LOW Brosch PDFCristina EnculescuNo ratings yet
- Watanabe 1989 Inactivation of Laboratory Animal RNA Viruses by Physicochemical TreatmentDocument7 pagesWatanabe 1989 Inactivation of Laboratory Animal RNA Viruses by Physicochemical Treatmentalejzamora9No ratings yet
- Germagic™ Thyme Disinfectant Spray For Coronavirus (Update) : Mahtas Covid-19 Rapid Evidence UpdatesDocument4 pagesGermagic™ Thyme Disinfectant Spray For Coronavirus (Update) : Mahtas Covid-19 Rapid Evidence UpdatesEuky Bear FgbNo ratings yet
- Test Bank For Microbiology An Introduction 12th Edition Tortora Funke Case DownloadDocument23 pagesTest Bank For Microbiology An Introduction 12th Edition Tortora Funke Case Downloadchristinemays21121993bgw100% (22)
- BSI Standards PublicationDocument46 pagesBSI Standards Publicationيحي عامرNo ratings yet
- Neodisher Septo DN: Disinfectant For The Automated Reprocessing of Flexible Endoscopes and Thermolabile InstrumentsDocument2 pagesNeodisher Septo DN: Disinfectant For The Automated Reprocessing of Flexible Endoscopes and Thermolabile InstrumentsArsyadNo ratings yet
- Carrier Tests To Assess Microbicidal Activities of Chemical Disinfectants For Use On Medical Devices and Environmental SurfacesDocument20 pagesCarrier Tests To Assess Microbicidal Activities of Chemical Disinfectants For Use On Medical Devices and Environmental Surfacesabd el rhman gamalNo ratings yet
- Aquazix Plus Ag 2022 09 30 b03Document4 pagesAquazix Plus Ag 2022 09 30 b03KerdraonNo ratings yet
- Disinfection GatewayDocument6 pagesDisinfection GatewaylynnNo ratings yet
- Sanitizing Agents For Virus Inactivation and DisinfectionDocument26 pagesSanitizing Agents For Virus Inactivation and DisinfectionhhNo ratings yet
- IMAEC Disinfectant Product Catalogue - DigitalCopy - April - 2023Document32 pagesIMAEC Disinfectant Product Catalogue - DigitalCopy - April - 2023ToureNo ratings yet
- Product Information Orotol Plus Disinfection of Suction SystemsDocument2 pagesProduct Information Orotol Plus Disinfection of Suction SystemsAwdan MailNo ratings yet
- En 14885 - 2022Document72 pagesEn 14885 - 2022rixalopesNo ratings yet
- Surfasafe Disinfectant Detergent For Surfaces and Equipment Fqy PDFDocument2 pagesSurfasafe Disinfectant Detergent For Surfaces and Equipment Fqy PDFAlaa FasialNo ratings yet
- 100% Automated: Bio-Disinfection and Disinfestation TreatmentsDocument16 pages100% Automated: Bio-Disinfection and Disinfestation TreatmentsUlprsudCiamisNo ratings yet
- Efficacy of Ethanol Against Viruses in Hand DisinfectionDocument9 pagesEfficacy of Ethanol Against Viruses in Hand DisinfectionImaec LimitedNo ratings yet
- CUM-02-E (CYW-201 User Manual) (Rev.2)Document30 pagesCUM-02-E (CYW-201 User Manual) (Rev.2)Miguel DiazNo ratings yet
- Bardac 208M - APIC CSPA PosterDocument1 pageBardac 208M - APIC CSPA PosterDyaniNo ratings yet
- ANTONIO - Short TalkDocument42 pagesANTONIO - Short TalkJazMine AntonioNo ratings yet
- Nisus DSV LabelDocument24 pagesNisus DSV LabelwilliamNo ratings yet
- Clifton UltrasonicDocument19 pagesClifton UltrasonicSami Al SamowNo ratings yet
- Condensed Guidance On Disinfection Solutions (UNHCR 2020) - v1.2Document4 pagesCondensed Guidance On Disinfection Solutions (UNHCR 2020) - v1.2Joel OchiengNo ratings yet
- Ga Wash-Master Eco en 2015-11-04Document69 pagesGa Wash-Master Eco en 2015-11-04Moas GabrounNo ratings yet
- Hydris Hydris™: Disinfectant CleanerDocument1 pageHydris Hydris™: Disinfectant Cleanernikors65No ratings yet
- Can Ethnopharmacology Contribute To The Dev of Antiviral Drug - Vlietinck1991Document13 pagesCan Ethnopharmacology Contribute To The Dev of Antiviral Drug - Vlietinck1991Tyasmeita14No ratings yet
- Disinfection Water: A Superior & Safe Environmental Solution in The Biological & Deodorization ofDocument8 pagesDisinfection Water: A Superior & Safe Environmental Solution in The Biological & Deodorization ofedwin fernandezNo ratings yet
- Infectious Diseases 2022 Virtual Abstract BookDocument53 pagesInfectious Diseases 2022 Virtual Abstract BookSriNo ratings yet