You might also like
- Impact of Stress on EmployeesDocument10 pagesImpact of Stress on EmployeesTulika singhNo ratings yet
- Cohen 1999Document14 pagesCohen 1999Devasish KNo ratings yet
- Occupational Neuroplasticity BrainDocument15 pagesOccupational Neuroplasticity BrainGabriiella ChaviraNo ratings yet
- Lu 2016Document13 pagesLu 2016Diana WijayaNo ratings yet
- Boubekri Et Al - 2014 - Impact of Windows and Daylight Exposure On Overall Health and Sleep Quality ofDocument9 pagesBoubekri Et Al - 2014 - Impact of Windows and Daylight Exposure On Overall Health and Sleep Quality ofDr.QiuNo ratings yet
- 1 s2.0 S0169814111000151 MainDocument6 pages1 s2.0 S0169814111000151 MainQNE INTERNALNo ratings yet
- Reciprocal Effects of Work Stressors and Counterproductive Work Behavior: A Five-Wave Longitudinal StudyDocument11 pagesReciprocal Effects of Work Stressors and Counterproductive Work Behavior: A Five-Wave Longitudinal StudyMădălina SimionNo ratings yet
- A Personal Projects Analysis: Examining Adaptation To Low Back PainDocument11 pagesA Personal Projects Analysis: Examining Adaptation To Low Back PainamdtzNo ratings yet
- Sage Publications, Inc., Johnson Graduate School of Management, Cornell University Administrative Science QuarterlyDocument25 pagesSage Publications, Inc., Johnson Graduate School of Management, Cornell University Administrative Science QuarterlyAlejandro GarcíaNo ratings yet
- Karasek1979 Job DemandsDocument25 pagesKarasek1979 Job DemandsCorina S. R. MaschioNo ratings yet
- Artigo 5Document2 pagesArtigo 5Gabriel RodriguesNo ratings yet
- The (In) Significance of Executive Functions For The Trait of Self-ControlDocument12 pagesThe (In) Significance of Executive Functions For The Trait of Self-ControlMiguel Ángel DominguezNo ratings yet
- Jurnal WorkLoadDocument12 pagesJurnal WorkLoadAufa NabilahNo ratings yet
- Workplace Stressors and Employee Performance: A Conceptual ReviewDocument10 pagesWorkplace Stressors and Employee Performance: A Conceptual ReviewDhanunjayaNo ratings yet
- Improvisation For Prefrontal RehabilitationDocument28 pagesImprovisation For Prefrontal RehabilitationB Carvalheiro100% (1)
- NIH Public Access: Author ManuscriptDocument32 pagesNIH Public Access: Author ManuscriptJorgeBarriosMurielNo ratings yet
- Physiological Stress During Simultaneous Interpreting: A Comparison of Experts and NovicesDocument17 pagesPhysiological Stress During Simultaneous Interpreting: A Comparison of Experts and NovicesBé SâuNo ratings yet
- Park, 2019Document10 pagesPark, 2019Fatimah EkaNo ratings yet
- Factors contributing to work-ability for injured workersDocument12 pagesFactors contributing to work-ability for injured workersRashmi SheelvantNo ratings yet
- Brain InjuriesDocument15 pagesBrain Injuriesprabhakar_n1No ratings yet
- Editorial Effect of Neurophysiological ConditionsDocument3 pagesEditorial Effect of Neurophysiological ConditionsHeloiana FaroNo ratings yet
- Basics of NeuropsychologyDocument7 pagesBasics of NeuropsychologyJasroop MahalNo ratings yet
- Social Science 6 A 1155 1160 Full PaperDocument6 pagesSocial Science 6 A 1155 1160 Full PaperMeraj HasanNo ratings yet
- The Effects of Self-Efficacy On Physical and Cognitive Performance 2022Document9 pagesThe Effects of Self-Efficacy On Physical and Cognitive Performance 2022Adrienn VargaNo ratings yet
- EVIDENCE-BASED PROJECT, PART 3 CRITICAL APPRAISAL OF RESEARCHDocument13 pagesEVIDENCE-BASED PROJECT, PART 3 CRITICAL APPRAISAL OF RESEARCHjennylovex4realNo ratings yet
- Assessing Workload in Neuropsychology: An Illustration With The Tower of Hanoi TestDocument9 pagesAssessing Workload in Neuropsychology: An Illustration With The Tower of Hanoi TestMaxNo ratings yet
- School of Psychology: Exam ID Assessment TitleDocument16 pagesSchool of Psychology: Exam ID Assessment TitleSerge SedunovsNo ratings yet
- Anxiety Working MemoryDocument23 pagesAnxiety Working Memoryt mdeNo ratings yet
- Mork 2015Document10 pagesMork 2015andresNo ratings yet
- Loewenstein Occupational T Erapy Cognitive Assessment (LOTCA) Battery For Brain-Injured Patients: Reliability and ValidityDocument9 pagesLoewenstein Occupational T Erapy Cognitive Assessment (LOTCA) Battery For Brain-Injured Patients: Reliability and ValidityZaira Sánchez GonzaloNo ratings yet
- Human - Performance - Under - Sustained - Operat20151127 6440 A9djjs With Cover Page v2Document11 pagesHuman - Performance - Under - Sustained - Operat20151127 6440 A9djjs With Cover Page v2Aljho AljhoNo ratings yet
- The Job Content Questionnaire (JCQ) : An Instrument For Internationally Comparative Assessments of Psychosocial Job CharacteristicsDocument35 pagesThe Job Content Questionnaire (JCQ) : An Instrument For Internationally Comparative Assessments of Psychosocial Job CharacteristicsIonela BogdanNo ratings yet
- Psychological Empowerment and Burnout: Different Patterns of Relationship With Three Types of Job DemandsDocument13 pagesPsychological Empowerment and Burnout: Different Patterns of Relationship With Three Types of Job DemandsAlber QuemasdaNo ratings yet
- Ahsberg 2000 Perceive Fatigue SOFIDocument18 pagesAhsberg 2000 Perceive Fatigue SOFIMerydian JosephineNo ratings yet
- 135 Li (2013) Job Demands Job Resources and Safety OutcomesDocument10 pages135 Li (2013) Job Demands Job Resources and Safety OutcomesMohammad RidswanNo ratings yet
- Raichlen 2016Document14 pagesRaichlen 2016GsNo ratings yet
- Basso Etal.2015 PDFDocument12 pagesBasso Etal.2015 PDFSixto Guardo MarmolNo ratings yet
- The Effect of Perceptual Load On Performance Within IDE in People With ADHD SymptomsDocument20 pagesThe Effect of Perceptual Load On Performance Within IDE in People With ADHD SymptomsViorelMocanuNo ratings yet
- The Role of The Medial Prefrontal Cortex in Moderating Neural Representations of Self and Other in PrimatesDocument19 pagesThe Role of The Medial Prefrontal Cortex in Moderating Neural Representations of Self and Other in PrimatesKriss Ioana AgapieNo ratings yet
- 1 s2.0 S0169814108000309 MainDocument7 pages1 s2.0 S0169814108000309 MainQNE INTERNALNo ratings yet
- Electrical Stimulation of Visual Cortex Relevance For TheDocument34 pagesElectrical Stimulation of Visual Cortex Relevance For TheroachikitoNo ratings yet
- Karasek Et Al 1998 PDFDocument34 pagesKarasek Et Al 1998 PDFCarlos Manuel AbalosNo ratings yet
- The Job Characteristics Theory: A Review: October 1997Document14 pagesThe Job Characteristics Theory: A Review: October 1997Sînziana SmutzerNo ratings yet
- The Effect of Blue Light Filtration On Sleep & Work OutcomesDocument13 pagesThe Effect of Blue Light Filtration On Sleep & Work OutcomesAries YeungNo ratings yet
- 2012 - A Key Role For Experimental Task Performance Effects of Math Talent, Gender and Performance On The Neural Correlates of Mental RotationDocument14 pages2012 - A Key Role For Experimental Task Performance Effects of Math Talent, Gender and Performance On The Neural Correlates of Mental RotationClinica EvolueNo ratings yet
- Neuroimaging Primer for Clinical NeuroscienceDocument9 pagesNeuroimaging Primer for Clinical NeuroscienceCarola ValdésNo ratings yet
- Do Cognitive Appraisals Moderate The Link Between Qualitative Job Insecurity and Psychological-Behavioral Well-Being?Document18 pagesDo Cognitive Appraisals Moderate The Link Between Qualitative Job Insecurity and Psychological-Behavioral Well-Being?Ian SafiyanNo ratings yet
- 2 Functional Imaging and Related TechniquesDocument33 pages2 Functional Imaging and Related TechniquesAlaa Naser HunikelNo ratings yet
- The Relationship Between Executive Functions and Uid Intelligence in Parkinson's DiseaseDocument8 pagesThe Relationship Between Executive Functions and Uid Intelligence in Parkinson's DiseaseEugenia FiginiNo ratings yet
- Karasekea 1998Document35 pagesKarasekea 1998Ronamaruko KiranaNo ratings yet
- 10 1126@science Aba3313 PDFDocument16 pages10 1126@science Aba3313 PDFFerviferrazNo ratings yet
- Urbina Barraza David (2019) Return To Work After An Acquired Brain Injury Why The Subjective Experience of The Patient Is ImportantDocument3 pagesUrbina Barraza David (2019) Return To Work After An Acquired Brain Injury Why The Subjective Experience of The Patient Is Importantdavid.urbinaNo ratings yet
- Essence and Consequences of Stress in The Work Place.: January 2012Document12 pagesEssence and Consequences of Stress in The Work Place.: January 2012112Mellania Widya NNo ratings yet
- Impact of Job Stress by Shahid HafeezDocument9 pagesImpact of Job Stress by Shahid HafeezShahid HafeezNo ratings yet
- The Relationship Between Working Memory Capacity and Executive Functioning: Evidence for a Common Executive Attention ConstructDocument38 pagesThe Relationship Between Working Memory Capacity and Executive Functioning: Evidence for a Common Executive Attention ConstructKanika BhaskarNo ratings yet
- PVQ Technical ManualDocument38 pagesPVQ Technical Manualnaneshwari98No ratings yet
- Journal of Applied Psychology Volume 79 Issue 3 1994 (Doi 10.1037/0021-9010.79.3.364) Lee, Cynthia Bobko, Philip - Self-Efficacy Beliefs - Comparison of Five Measures. PDFDocument6 pagesJournal of Applied Psychology Volume 79 Issue 3 1994 (Doi 10.1037/0021-9010.79.3.364) Lee, Cynthia Bobko, Philip - Self-Efficacy Beliefs - Comparison of Five Measures. PDFAjeng Tita NawangsariNo ratings yet
- Bab 1&2Document21 pagesBab 1&2Muhammad Rizki syahputra, S.TNo ratings yet
- Cognitive Ergonomics and Its Role For Industry Safety Enhancements 2165 7556 1000e158Document3 pagesCognitive Ergonomics and Its Role For Industry Safety Enhancements 2165 7556 1000e158Sutris YandriNo ratings yet
- Psychophysiological assessment of human cognition and its enhancement by a non-invasive methodFrom EverandPsychophysiological assessment of human cognition and its enhancement by a non-invasive methodNo ratings yet
- Psych 1 2017 15Document14 pagesPsych 1 2017 15BrunoNo ratings yet
- 2d7b0cb6f2e3ef5b78e7788c4ab19c17Document286 pages2d7b0cb6f2e3ef5b78e7788c4ab19c17BrunoNo ratings yet
- The Fantastic Redemption of Reality: Temenuga TrifonovaDocument25 pagesThe Fantastic Redemption of Reality: Temenuga TrifonovaBrunoNo ratings yet
- Nouvelle Manga and Cinema: Temenuga TrifonovaDocument16 pagesNouvelle Manga and Cinema: Temenuga TrifonovaBrunoNo ratings yet
- Multiple Personality and The Discourse of The Multiple in Hollywood CinemaDocument29 pagesMultiple Personality and The Discourse of The Multiple in Hollywood CinemaBrunoNo ratings yet
- Nouvelle Manga and Cinema: Temenuga TrifonovaDocument16 pagesNouvelle Manga and Cinema: Temenuga TrifonovaBrunoNo ratings yet
- Kiralyfalvi 1983Document4 pagesKiralyfalvi 1983BrunoNo ratings yet
- Studies in Documentary FilmDocument18 pagesStudies in Documentary FilmBrunoNo ratings yet
- The European Realist Tradition: Studies in European CinemaDocument15 pagesThe European Realist Tradition: Studies in European CinemaBrunoNo ratings yet
- David B. Cooper - Alcohol Use (2000)Document307 pagesDavid B. Cooper - Alcohol Use (2000)BrunoNo ratings yet
- The Hudson Review, IncDocument5 pagesThe Hudson Review, IncBrunoNo ratings yet
- Intelligent Materialism - Essays On Hegel and Dialectics by Evald Ilyenkov, Translated by Evgeni PavlovDocument265 pagesIntelligent Materialism - Essays On Hegel and Dialectics by Evald Ilyenkov, Translated by Evgeni Pavlovirulala100% (3)
- Moretti - Atlas of The European NovelDocument112 pagesMoretti - Atlas of The European Novelincilosh100% (1)
- The Johns Hopkins University PressDocument8 pagesThe Johns Hopkins University PressBrunoNo ratings yet
- Cooper, David B - Developing Services in Mental Health-Substance Use-CRC Press (2016) PDFDocument242 pagesCooper, David B - Developing Services in Mental Health-Substance Use-CRC Press (2016) PDFBrunoNo ratings yet
- (Mental Health-Substance Use 7) Cooper, David B - Ethics in Mental-Health Substance Use-Routledge (2017)Document383 pages(Mental Health-Substance Use 7) Cooper, David B - Ethics in Mental-Health Substance Use-Routledge (2017)Bruno75% (4)
- (Mental Health-Substance Use.) Cooper, David B. - Zarconi, Joseph - Introduction To Mental Health - Substance Use.-Chapman and Hall - CRC (2017)Document224 pages(Mental Health-Substance Use.) Cooper, David B. - Zarconi, Joseph - Introduction To Mental Health - Substance Use.-Chapman and Hall - CRC (2017)Bruno0% (1)
- 1978 - Sexism and Science PDFDocument196 pages1978 - Sexism and Science PDFBrunoNo ratings yet
- 2010 - Social Structure and Forms of Consciousness. Vol. 1, The Social Determination of MethodDocument464 pages2010 - Social Structure and Forms of Consciousness. Vol. 1, The Social Determination of MethodBrunoNo ratings yet
- The Hidden Tools of Comedy The Serious Business of Being Funny PDFDocument190 pagesThe Hidden Tools of Comedy The Serious Business of Being Funny PDFMina89% (18)
- Ethics and Heritage Essays On The Philosophy of Agnes Heller PDFDocument256 pagesEthics and Heritage Essays On The Philosophy of Agnes Heller PDFBrunoNo ratings yet
- First Exam Fifa CorruptionDocument3 pagesFirst Exam Fifa Corruptionarmy kaNo ratings yet
- A Review of Research On Teacher Beliefs and PracticesDocument20 pagesA Review of Research On Teacher Beliefs and Practiceschikondi sepulaNo ratings yet
- Emcee King & QueenDocument8 pagesEmcee King & QueenMaryHazelClaveBeniga100% (10)
- English to Oromo Machine Translation ExperimentDocument86 pagesEnglish to Oromo Machine Translation ExperimentAnonymous 2WKRBqFlfNo ratings yet
- 100 Awesome Chess Moves by Eric Schiller PDFDocument290 pages100 Awesome Chess Moves by Eric Schiller PDFAbhilasha0% (1)
- Ebook - Return-to-Gentleness by Anthony M McCrovitzDocument192 pagesEbook - Return-to-Gentleness by Anthony M McCrovitzSónia CarvalhoNo ratings yet
- A Study On Marketing Practices in Select PDFDocument137 pagesA Study On Marketing Practices in Select PDFSadik SadikaramaniNo ratings yet
- Chapter 32Document22 pagesChapter 32Clifford BacsarzaNo ratings yet
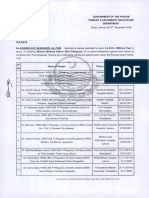
- Punjab govt grants EOL to doctors for postgraduate trainingDocument2 pagesPunjab govt grants EOL to doctors for postgraduate trainingMasroor HassanNo ratings yet
- Modernist PoetryDocument14 pagesModernist PoetryFaisal JahangirNo ratings yet
- Comparative ResearchDocument22 pagesComparative Researchtshiringtmg7No ratings yet
- PhilosophyDocument1 pagePhilosophyElena Luneta-BibeNo ratings yet
- Theories of StressDocument15 pagesTheories of Stressyared desta100% (1)
- Verbal and Nonverbal Communication - Business Communication Skills For ManagersDocument7 pagesVerbal and Nonverbal Communication - Business Communication Skills For ManagersCINDY BALANONNo ratings yet
- Audit of Receivables Pre-Assessment: Acctg35Document3 pagesAudit of Receivables Pre-Assessment: Acctg35Jeane Mae BooNo ratings yet
- Freud BabaDocument11 pagesFreud Babapartha19881062No ratings yet
- Labour Law Course WorkDocument5 pagesLabour Law Course WorkUncle BrianNo ratings yet
- The Pen Pal ProjectDocument1 pageThe Pen Pal ProjectMelanie Yosiris Mayorga FonsecaNo ratings yet
- 3 Week Lit 121Document48 pages3 Week Lit 121Cassandra Dianne Ferolino MacadoNo ratings yet
- UWORLD Notes by Subject (Main Division) (Usmle Grassroots)Document80 pagesUWORLD Notes by Subject (Main Division) (Usmle Grassroots)Mital Bhakta83% (18)
- Y4A Practice Book Answers White Rose Maths EditionDocument20 pagesY4A Practice Book Answers White Rose Maths EditionNgọc YếnNo ratings yet
- Author's Purpose in WritingDocument37 pagesAuthor's Purpose in WritingJenna Alyssa BaligatNo ratings yet
- Music in The United KingdomDocument33 pagesMusic in The United KingdomIonut PetreNo ratings yet
- People v Garaygay Ruling on Motion to Quash Search WarrantDocument1 pagePeople v Garaygay Ruling on Motion to Quash Search WarrantchiccostudentNo ratings yet
- DevStat8e 16 04Document28 pagesDevStat8e 16 04SaadiShahwanNo ratings yet
- A Case Study of A Turnaround PrincipalDocument7 pagesA Case Study of A Turnaround PrincipalReynante Roxas MalanoNo ratings yet
- Experiential Marketing How To Get Customers To Sense, Feel, Think, Act, RelateDocument6 pagesExperiential Marketing How To Get Customers To Sense, Feel, Think, Act, RelateBhaumik NayakNo ratings yet
- Abb Ag CN12Document3 pagesAbb Ag CN12Francisco ViglusNo ratings yet
- Acute cholecystitis pathogenesis, diagnosis and clinical featuresDocument38 pagesAcute cholecystitis pathogenesis, diagnosis and clinical featuresAdrian BăloiNo ratings yet
- The Tracking Shot in Kapo Serge Daney Senses of CinemaDocument22 pagesThe Tracking Shot in Kapo Serge Daney Senses of CinemaMarcos GonzálezNo ratings yet