You might also like
- Risk of Gastrointestinal Bleeding in Patients With End-Stage Renal DiseaseDocument10 pagesRisk of Gastrointestinal Bleeding in Patients With End-Stage Renal DiseaseEuclea MandolangNo ratings yet
- Heart Failure: Peter A. Mccullough, MD, MPH, Facc, Facp, Faha, FCCPDocument54 pagesHeart Failure: Peter A. Mccullough, MD, MPH, Facc, Facp, Faha, FCCPDenisse Tinajero SánchezNo ratings yet
- Acute Coronary SyndromeDocument50 pagesAcute Coronary SyndromeAnggi KusumaNo ratings yet
- Acute Coronary SyndromesDocument40 pagesAcute Coronary Syndromesandi siregarNo ratings yet
- Sindrom Koroner Akut: DR Yosman SP JP RSUD Setjonegoro Wonosobo 2018Document46 pagesSindrom Koroner Akut: DR Yosman SP JP RSUD Setjonegoro Wonosobo 2018Fino GunnersNo ratings yet
- What the guidelines say about ACS diagnosis and managementDocument43 pagesWhat the guidelines say about ACS diagnosis and managementberthyNo ratings yet
- Angina Pect & Infark Miokard (Dr. Ilham Uddin, SP - JP (K) )Document108 pagesAngina Pect & Infark Miokard (Dr. Ilham Uddin, SP - JP (K) )Vania Nazhara FitrianaNo ratings yet
- Insufficienza Cardiaca: Prof. Carlo MoroniDocument43 pagesInsufficienza Cardiaca: Prof. Carlo MoroniGiuseppe FoggiaNo ratings yet
- Treatment Based On: Pathophysiology of HyperglycemiaDocument38 pagesTreatment Based On: Pathophysiology of HyperglycemiaRoby KieranNo ratings yet
- Lecture 5 Macrovascular ComplicationsDocument51 pagesLecture 5 Macrovascular ComplicationsCristinaGheorgheNo ratings yet
- Peripheral VascularDocument35 pagesPeripheral VascularAren Denmark GamboaNo ratings yet
- Vascular: DiseasesDocument4 pagesVascular: DiseasesRiah Mae MertoNo ratings yet
- Sindrom Koroner AkutDocument46 pagesSindrom Koroner AkutLilik Niswatun FazaNo ratings yet
- Impact of Using Non-Rebreathing Mask in Patients With Respiratory FailureDocument17 pagesImpact of Using Non-Rebreathing Mask in Patients With Respiratory Failureedsel ligiantaNo ratings yet
- Ventricular Septal Defect: Present by Nur Kurnia Putri Halim Supervisor Dr. Akhtar Fajar M, SPJP, FihaDocument31 pagesVentricular Septal Defect: Present by Nur Kurnia Putri Halim Supervisor Dr. Akhtar Fajar M, SPJP, FihaChintya Fidelia MontangNo ratings yet
- StrokeDocument53 pagesStrokeGhinaSofianaLestari100% (1)
- ACS LectureDocument74 pagesACS Lecturekarin amalia sabrinaNo ratings yet
- Acute Coronary SyndromeDocument5 pagesAcute Coronary SyndromeLuis OportoNo ratings yet
- Tuko SrimulyoDocument56 pagesTuko SrimulyoRiri EltadezaNo ratings yet
- Patofisiologi ACSDocument48 pagesPatofisiologi ACSImelva GirsangNo ratings yet
- Hipertensiunea ArterialaDocument89 pagesHipertensiunea ArterialaDaniela ChelaruNo ratings yet
- Chest Pain Evaluation and Management - 2023 - Physician Assistant ClinicsDocument16 pagesChest Pain Evaluation and Management - 2023 - Physician Assistant ClinicsJose AnaconaNo ratings yet
- NSTEMIDocument22 pagesNSTEMImadeputraNo ratings yet
- Chest Pain: Differential Diagnosis Walid TARCHA, MD Umc Rizk HospitalDocument56 pagesChest Pain: Differential Diagnosis Walid TARCHA, MD Umc Rizk HospitalAli B. SafadiNo ratings yet
- Hennekens Cardio Aspirin Past To FutureDocument20 pagesHennekens Cardio Aspirin Past To FutureLona LetwarNo ratings yet
- Cardiovascular Diseases in GeriatricsDocument31 pagesCardiovascular Diseases in Geriatricsnurul dwi ratihNo ratings yet
- Hamaguchi 2009Document7 pagesHamaguchi 2009Nur Syamsiah MNo ratings yet
- DR Rahul VarshneyDocument64 pagesDR Rahul VarshneyIMNo ratings yet
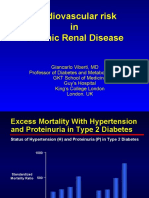
- Cardiovascular Risk in Chronic Renal DiseaseDocument36 pagesCardiovascular Risk in Chronic Renal DiseaseahkyenNo ratings yet
- FinalDocument44 pagesFinalBader KamelNo ratings yet
- Family Medicine Study GuideDocument240 pagesFamily Medicine Study GuideJeremy Christmann100% (1)
- Arrhythmia risks after thrombolytic therapyDocument5 pagesArrhythmia risks after thrombolytic therapyTaniaNo ratings yet
- Askep Pada Acute Coronary Syndrome AcsDocument62 pagesAskep Pada Acute Coronary Syndrome Acsdefi rhNo ratings yet
- DIABertelt2017 14Document7 pagesDIABertelt2017 14marsim92No ratings yet
- NSTEMI Refarat Cardio 2016Document48 pagesNSTEMI Refarat Cardio 2016Anonymous IOkNvM8VbtNo ratings yet
- BHD 285 - 294Document10 pagesBHD 285 - 294nurul hidayatiNo ratings yet
- Coronary Artery Disease Risk Factors and TreatmentDocument60 pagesCoronary Artery Disease Risk Factors and TreatmentliliNo ratings yet
- Update Management ACS Irvan PekanbaruDocument52 pagesUpdate Management ACS Irvan PekanbaruSri IsminartiNo ratings yet
- Artículo Arritmias Cardiacas en Enfermedades AutoinmunesDocument10 pagesArtículo Arritmias Cardiacas en Enfermedades AutoinmunesDiana ArmasNo ratings yet
- Kolesterol-16-21Document6 pagesKolesterol-16-21PersonaliacNo ratings yet
- K21 - Stroke Hemoragik (Neurologi)Document34 pagesK21 - Stroke Hemoragik (Neurologi)juardyNo ratings yet
- Acute Coronary Syndrome Sindroma Koroner Akut: Toni Mustahsani Aprami, DR., SPPD, SPJPDocument57 pagesAcute Coronary Syndrome Sindroma Koroner Akut: Toni Mustahsani Aprami, DR., SPPD, SPJPrian susantoNo ratings yet
- Recent Management Hypertension of Hypertensive Emergency in Stroke What We Learn From The Newest Evidence Dr. Paulus PDFDocument70 pagesRecent Management Hypertension of Hypertensive Emergency in Stroke What We Learn From The Newest Evidence Dr. Paulus PDFAndi Tiara S. AdamNo ratings yet
- Association Between Platelet-to-Lymphocyte Ratio and Severity of Coronary Artery DiseaseDocument7 pagesAssociation Between Platelet-to-Lymphocyte Ratio and Severity of Coronary Artery DiseaseMaferNo ratings yet
- Konsep Tatalaksana Pada ImaDocument57 pagesKonsep Tatalaksana Pada Imariska silviaNo ratings yet
- CVD in Diabetes - EADSG 2016Document57 pagesCVD in Diabetes - EADSG 2016OmarNo ratings yet
- Current Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFDocument51 pagesCurrent Management Strategies in ACS-Intervention or Conservative - Note, Dr. Faris B, SP - JP (K) FAP PDFSofia KusumadewiNo ratings yet
- STEMIDocument28 pagesSTEMIGP HMHNo ratings yet
- Based on the history, physical exam findings and investigations, what is the most likely diagnosisDocument44 pagesBased on the history, physical exam findings and investigations, what is the most likely diagnosisDila AswitaliaNo ratings yet
- Acute Coronary SyndromesDocument65 pagesAcute Coronary SyndromesrevininNo ratings yet
- Jurnal Kesmas - Neurological Manifestations in COVID-19 Patients at The Covid-19 National Emergency Hospital Wisma Atlet Kemayoran, IndonesiaDocument16 pagesJurnal Kesmas - Neurological Manifestations in COVID-19 Patients at The Covid-19 National Emergency Hospital Wisma Atlet Kemayoran, IndonesianskhldNo ratings yet
- Association of Multiple Infarctions and ICAS With Outcomes of Minor Stroke and TIADocument9 pagesAssociation of Multiple Infarctions and ICAS With Outcomes of Minor Stroke and TIAJhonny Churata HuarachiNo ratings yet
- SKA Webinar RS Dr. SoedarsoDocument49 pagesSKA Webinar RS Dr. SoedarsoRahmad RamadhaniNo ratings yet
- JurnalDocument16 pagesJurnalGemmy SistarinaNo ratings yet
- Managing Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoDocument45 pagesManaging Hidden Cardiovascular Risk in Diabetes Mellitus: Agus YuwonoaprinaaaNo ratings yet
- Ehf2 7 1125Document5 pagesEhf2 7 1125Pranvera ApostoliNo ratings yet
- IT 12 Coronary Artery DiseaseDocument53 pagesIT 12 Coronary Artery DiseaseM Fiqih ArrachmanNo ratings yet
- Pulseless Disease (Takayasu arteritis), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandPulseless Disease (Takayasu arteritis), A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Inhaled Corticosteroids and COVID-19-related Mortality: Confounding or Clarifying?Document2 pagesInhaled Corticosteroids and COVID-19-related Mortality: Confounding or Clarifying?Ecaterina StavilaNo ratings yet
- Ijms 20 01475 PDFDocument28 pagesIjms 20 01475 PDFFernanda GLNo ratings yet
- Diagnosis IPF Full LengthDocument25 pagesDiagnosis IPF Full LengthMark Vertiz CernaNo ratings yet
- Diagnosis IPF Full LengthDocument25 pagesDiagnosis IPF Full LengthMark Vertiz CernaNo ratings yet
- The Dyspnoea - Inactivity Vicious Circle in COPD: Development and External Validation of A Conceptual ModelDocument11 pagesThe Dyspnoea - Inactivity Vicious Circle in COPD: Development and External Validation of A Conceptual ModelEcaterina StavilaNo ratings yet
- Angioinvasive Aspergillosis in A 68-Yr-Old Male With Severe NeutropeniaDocument1 pageAngioinvasive Aspergillosis in A 68-Yr-Old Male With Severe NeutropeniaEcaterina StavilaNo ratings yet
- Bushings BrochureDocument14 pagesBushings Brochurebpd21No ratings yet
- Manual Carpa Instant TentDocument2 pagesManual Carpa Instant TentBermans Olivares LayNo ratings yet
- Science Report - Stem CellsDocument7 pagesScience Report - Stem CellsKay NeethlingNo ratings yet
- Present Perfect and Simple Past Tenses in ESL Grammar ExercisesDocument36 pagesPresent Perfect and Simple Past Tenses in ESL Grammar ExercisesNguyen Quoc AnhNo ratings yet
- De-Escalation of Critical Care and Prevention of Iatrogenicity Through PICU Liberation Rounding Process and A Daily Rounding ChecklistDocument1 pageDe-Escalation of Critical Care and Prevention of Iatrogenicity Through PICU Liberation Rounding Process and A Daily Rounding ChecklistdarlingcarvajalduqueNo ratings yet
- Saa6d170e-5 HPCR Egr Sen00190-04Document415 pagesSaa6d170e-5 HPCR Egr Sen00190-04Ahmad Mubarok100% (4)
- Max Out On Squats Every Day PDFDocument7 pagesMax Out On Squats Every Day PDFsamsung684No ratings yet
- Syllabus For TR Supervisors Quality AssurnaceDocument67 pagesSyllabus For TR Supervisors Quality Assurnaceadnanlibra194No ratings yet
- Official All Things Turmeric PPT GuidebookDocument14 pagesOfficial All Things Turmeric PPT Guidebookapi-507527047No ratings yet
- Pneumatic System and Basic Valve UsedDocument401 pagesPneumatic System and Basic Valve Usedtarang srivasNo ratings yet
- HeavyMetalLimits For Leachability PROP 65 PB and CDDocument3 pagesHeavyMetalLimits For Leachability PROP 65 PB and CDspades24kNo ratings yet
- ACS Appl. Energy Mater. 5 (2022) 367-379 PDFDocument13 pagesACS Appl. Energy Mater. 5 (2022) 367-379 PDFEdgar QuintanillaNo ratings yet
- TEGO® Airex 901 W: Description Technical DataDocument1 pageTEGO® Airex 901 W: Description Technical Datahai nguyen100% (1)
- Benefits of Acupressure Health 2014Document44 pagesBenefits of Acupressure Health 2014Linh Tinh100% (1)
- Using Coffee Grounds as FertilizerDocument18 pagesUsing Coffee Grounds as FertilizerKyle BARRIOSNo ratings yet
- Tron Time Delay Fuse 500vDocument1 pageTron Time Delay Fuse 500valexjoelNo ratings yet
- Detection Dogs Allow For Systematic Non-Invasive Collection of DNA Samples From Eurasian LynxDocument5 pagesDetection Dogs Allow For Systematic Non-Invasive Collection of DNA Samples From Eurasian Lynxsusey madelit apaza mamaniNo ratings yet
- Surgical Methods of MTPDocument44 pagesSurgical Methods of MTPRajeev Sood100% (1)
- Aryatech Brochure IndiaDocument12 pagesAryatech Brochure IndiaHari RamNo ratings yet
- Graphing linear functions and writing equations in standard formDocument15 pagesGraphing linear functions and writing equations in standard formnmarjonoNo ratings yet
- 1Document36 pages1Abrvalg_1No ratings yet
- Compounding Pharmacy Information SheetDocument2 pagesCompounding Pharmacy Information SheetSatish HiremathNo ratings yet
- Chennai Public School: CH 3 Coordinate Geometry Multiple AssessmentDocument3 pagesChennai Public School: CH 3 Coordinate Geometry Multiple Assessment11F10 RUCHITA MAARANNo ratings yet
- Cology MCQDocument4 pagesCology MCQHemant BaraiNo ratings yet
- SB 10054865 6305Document15 pagesSB 10054865 6305Ralph WamaeNo ratings yet
- MANAURITE XM Material PDFDocument8 pagesMANAURITE XM Material PDFkbc404No ratings yet
- Tamil HoroscopeDocument3 pagesTamil HoroscopecivaasNo ratings yet
- Banaba Tea Aids Weight LossDocument5 pagesBanaba Tea Aids Weight LossAveriAlonzoNo ratings yet
- Bangla FoodsDocument6 pagesBangla FoodsSubadrika DarmadewiNo ratings yet
- Luftwaffe Night Fighter Control MethodsDocument17 pagesLuftwaffe Night Fighter Control MethodsKIRU SILVIU100% (3)