You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5819)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (845)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Lesson Plan On DVTDocument18 pagesLesson Plan On DVTAlma Susan100% (1)
- SYCDW 2011 Coag Made EasyDocument17 pagesSYCDW 2011 Coag Made EasyRose KasidiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Hem Lab Microhematocrit F15Document10 pagesHem Lab Microhematocrit F15Joan Christie WijayaNo ratings yet
- Capillary Puncture Equipment and ProcedureDocument3 pagesCapillary Puncture Equipment and ProcedureSieg100% (1)
- Fractures of FemurDocument1 pageFractures of FemurYogi drNo ratings yet
- Fractures of FemurDocument1 pageFractures of FemurYogi drNo ratings yet
- Maternal and Neonatal Outcomes of Pregnant Women With COVID-19 Pneumonia: A Case-Control StudyDocument20 pagesMaternal and Neonatal Outcomes of Pregnant Women With COVID-19 Pneumonia: A Case-Control StudyYogi drNo ratings yet
- Pathology of Fructure & OsteoprosisDocument3 pagesPathology of Fructure & OsteoprosisYogi drNo ratings yet
- Pathology of OsteoarthritisDocument2 pagesPathology of OsteoarthritisYogi drNo ratings yet
- Nonsteroidal Anti-Inflamatory DrugsDocument4 pagesNonsteroidal Anti-Inflamatory DrugsYogi drNo ratings yet
- Neuromuscular Blocking DrugsDocument3 pagesNeuromuscular Blocking DrugsYogi drNo ratings yet
- Muscles of The Gluteal RegionDocument2 pagesMuscles of The Gluteal RegionYogi drNo ratings yet
- Comments, Opinions, and Reviews: Vascular Syndromes of The ThalamusDocument15 pagesComments, Opinions, and Reviews: Vascular Syndromes of The ThalamusYogi drNo ratings yet
- Abdominal Wall Defects: Omphalocele and Gastroschisis: DR - Enono Yhoshu Department of Pediatric SurgeryDocument42 pagesAbdominal Wall Defects: Omphalocele and Gastroschisis: DR - Enono Yhoshu Department of Pediatric SurgeryYogi drNo ratings yet
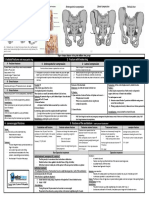
- Fracturte of Pelvis PDFDocument2 pagesFracturte of Pelvis PDFYogi drNo ratings yet
- Cardiac Arrest PDFDocument4 pagesCardiac Arrest PDFYogi drNo ratings yet
- Surgical Anatomy-Anal Canal: Dr. Belal MansoorDocument79 pagesSurgical Anatomy-Anal Canal: Dr. Belal MansoorYogi drNo ratings yet
- Abdominal Wall Defects: Omphalocele GastroschisisDocument20 pagesAbdominal Wall Defects: Omphalocele GastroschisisYogi drNo ratings yet
- Human Kidney Is A Target For Novel Severe Acute Respiratory Syndrome Coronavirus 2 (Sars-Cov-2) InfectionDocument16 pagesHuman Kidney Is A Target For Novel Severe Acute Respiratory Syndrome Coronavirus 2 (Sars-Cov-2) InfectionYogi drNo ratings yet
- Sexually Transmitted Diseases 1Document3 pagesSexually Transmitted Diseases 1Yogi drNo ratings yet
- Axonal Degeneration: Nerve RegenerationDocument1 pageAxonal Degeneration: Nerve RegenerationYogi drNo ratings yet
- Gender Differences in Patients With COVID-19: Focus On Severity and MortalityDocument18 pagesGender Differences in Patients With COVID-19: Focus On Severity and MortalityYogi drNo ratings yet
- Medial Longitudinal BundleDocument14 pagesMedial Longitudinal BundleYogi drNo ratings yet
- Imaging in Acute Abdomen: Dr. Wan Najwa Zaini Wan Mohamed Radiologist, Hospital Queen Elizabeth IiDocument70 pagesImaging in Acute Abdomen: Dr. Wan Najwa Zaini Wan Mohamed Radiologist, Hospital Queen Elizabeth IiYogi drNo ratings yet
- Skull CommunicationDocument56 pagesSkull CommunicationYogi drNo ratings yet
- Vitamin B12 Deficiency and Anemia in 140 Taiwanese Female Lacto-VegetariansDocument13 pagesVitamin B12 Deficiency and Anemia in 140 Taiwanese Female Lacto-VegetariansLunaNo ratings yet
- Blood Bank List HariyanaDocument22 pagesBlood Bank List HariyanadaniNo ratings yet
- CASE REPORT COMPETITION With Identifying FeaturesDocument12 pagesCASE REPORT COMPETITION With Identifying FeaturesJoel Cesar AtinadoNo ratings yet
- Histology Laboratory Manual: Olgga A. Hara MSDocument77 pagesHistology Laboratory Manual: Olgga A. Hara MSMark LopezNo ratings yet
- Muscular SystemDocument3 pagesMuscular SystemJanica Pauline DaydayNo ratings yet
- Campbell Biology 12e (1) - 921-946Document26 pagesCampbell Biology 12e (1) - 921-946Lâm PhạmNo ratings yet
- Transfusion and Apheresis Science: Ravneet Kaur Bedi, Kshitija Mittal, Tanvi Sood, Rakesh Kumar, Ajay S. PraveenDocument3 pagesTransfusion and Apheresis Science: Ravneet Kaur Bedi, Kshitija Mittal, Tanvi Sood, Rakesh Kumar, Ajay S. PraveenLuis Enrique Tinoco JuradoNo ratings yet
- Epithelial TissueDocument26 pagesEpithelial Tissueaimi BatrisyiaNo ratings yet
- Tissue Level Lab Exercise ModuleDocument14 pagesTissue Level Lab Exercise Modulecasseyareola100% (1)
- MUST To KNOW in Blood Banking 1Document19 pagesMUST To KNOW in Blood Banking 1Aya Virtucio100% (1)
- Haematopathology 3:: Leucocytosis/LeucopeniaDocument113 pagesHaematopathology 3:: Leucocytosis/LeucopeniaarwaNo ratings yet
- Lab Report Ayham FaisalDocument7 pagesLab Report Ayham Faisalayham omariNo ratings yet
- Human Blood GroupsDocument12 pagesHuman Blood GroupsAme Roxan AwidNo ratings yet
- Blood Case 6Document12 pagesBlood Case 6إنعام الحفيانNo ratings yet
- Patient Medical Transcript C++ Mini ProjectDocument9 pagesPatient Medical Transcript C++ Mini ProjectAzmi Bin A MataliNo ratings yet
- Blood DonationDocument19 pagesBlood Donationsundesh4100% (1)
- 3-Differential WBC CountDocument11 pages3-Differential WBC CountdlerNo ratings yet
- Guidelines On The Management of Massive Blood Loss: GuidelineDocument8 pagesGuidelines On The Management of Massive Blood Loss: GuidelineRatna AgustinaNo ratings yet
- XS 1000i English PDFDocument8 pagesXS 1000i English PDFTanveerNo ratings yet
- TissuesDocument9 pagesTissuesAtharv AggarwalNo ratings yet
- Notes: Heparin-Induced Thrombocytopenia (Hit)Document6 pagesNotes: Heparin-Induced Thrombocytopenia (Hit)MOHIT SHARMANo ratings yet
- Physiology of Muscle Tissue: A Marvel of Movement!Document119 pagesPhysiology of Muscle Tissue: A Marvel of Movement!romiNo ratings yet
- Notes - Structural Organisation in AnimalsDocument41 pagesNotes - Structural Organisation in AnimalsAnubhab SilNo ratings yet
- EpitheliumDocument48 pagesEpitheliumdrpankaj28100% (1)
- Chapter8-Transport in HumansDocument15 pagesChapter8-Transport in HumansミーチェルNo ratings yet
- Leunase and TrombolismDocument12 pagesLeunase and TrombolismSanta UlinaNo ratings yet