You might also like
- Nursing Orientation Program Intravenous TherapyDocument45 pagesNursing Orientation Program Intravenous TherapyMarianne LayloNo ratings yet
- Victorian Alphabets, Monograms and Names For Needleworkers - From Godey's Lady's Book and Peterson's Magazine (PDFDrive)Document113 pagesVictorian Alphabets, Monograms and Names For Needleworkers - From Godey's Lady's Book and Peterson's Magazine (PDFDrive)sheidi100% (4)
- Orthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingFrom EverandOrthopedic Inpatient Protocols: A Guide to Orthopedic Inpatient RoundingNo ratings yet
- (ASRA) Guidelines Neuraxial and AnticoagulationDocument6 pages(ASRA) Guidelines Neuraxial and Anticoagulationfraditayyunus82% (11)
- Fabella NotesDocument96 pagesFabella NotesAndrassy Twinkle AlineaNo ratings yet
- Upload 8Document2 pagesUpload 8cingyaNo ratings yet
- Best Practice ProtocolsDocument46 pagesBest Practice ProtocolsRaigheil LayNo ratings yet
- Echofish JRC Jfc-180bbDocument4 pagesEchofish JRC Jfc-180bbJERINsmileNo ratings yet
- Hammer Pulse TempDocument12 pagesHammer Pulse Temppeter911cm100% (1)
- OB Med Order KodigsDocument1 pageOB Med Order KodigsfloramaeyecyecNo ratings yet
- NCP + Dosage & Solution LectureDocument7 pagesNCP + Dosage & Solution LecturechristineNo ratings yet
- FLCCC Alliance MATHplus Protocol ENGLISHDocument2 pagesFLCCC Alliance MATHplus Protocol ENGLISHBhanu Kumar100% (1)
- TAM Poster 17 5 PRINTDocument1 pageTAM Poster 17 5 PRINTtonywiharjitoNo ratings yet
- Diabetes Mellitus TranscribingDocument23 pagesDiabetes Mellitus TranscribingJasmin B. ERMITANo ratings yet
- Nanotechnology in Civil EngineeringDocument22 pagesNanotechnology in Civil EngineeringNehad AhmedNo ratings yet
- Pre-Operative Orders Post-Op Orders (Ga)Document3 pagesPre-Operative Orders Post-Op Orders (Ga)Alissandra OcampoNo ratings yet
- Vancomycin DRUGSTUDYDocument3 pagesVancomycin DRUGSTUDYEmagra AzilNo ratings yet
- Business Law Syllabus (BLT)Document4 pagesBusiness Law Syllabus (BLT)Glene NallaNo ratings yet
- LESSON EXEMPLAR in ENGLISHDocument4 pagesLESSON EXEMPLAR in ENGLISHFelices Christy C. CorderoNo ratings yet
- Drug Study: Adult: Induction: 40 MGDocument2 pagesDrug Study: Adult: Induction: 40 MGpretty_mary100% (4)
- Clinical Pathway WhippleDocument4 pagesClinical Pathway WhipplemariamNo ratings yet
- Post-Op Orders - Reginald W. Martin, M.DDocument2 pagesPost-Op Orders - Reginald W. Martin, M.DIbrahim AlmohiniNo ratings yet
- Name of Patient. For GRP 3 1 Docx 2Document2 pagesName of Patient. For GRP 3 1 Docx 2Keisha BartolataNo ratings yet
- Pat Legault STUDENT COPY FALL2018Document7 pagesPat Legault STUDENT COPY FALL2018Sarah Jane VasquezNo ratings yet
- Document PDFDocument4 pagesDocument PDFDebasis SahooNo ratings yet
- AWR Pathway POCKET GUIDE OHSU 2016 01 06 SBODocument1 pageAWR Pathway POCKET GUIDE OHSU 2016 01 06 SBOhenryyech2No ratings yet
- Endorsement Sheet ICUDocument3 pagesEndorsement Sheet ICULANCE CHRISTIAN CUENCANo ratings yet
- RFH COVID-19 ICU Resource Pack FULL PDFDocument15 pagesRFH COVID-19 ICU Resource Pack FULL PDFQuique GarciaNo ratings yet
- ICU General Admission Orders: OthersDocument2 pagesICU General Admission Orders: OthersHANIMNo ratings yet
- 002 POS Format 1Document9 pages002 POS Format 1Roland Philip GoNo ratings yet
- PUD AdmitDocument2 pagesPUD AdmitLynn Marie Igos DelgadoNo ratings yet
- MODULE 3 STANDARDIZE PATIENT - INTRAPARTUM StudentsDocument7 pagesMODULE 3 STANDARDIZE PATIENT - INTRAPARTUM StudentsalliahjaneadlawanNo ratings yet
- Contrast Reaction Card PediatricDocument2 pagesContrast Reaction Card PediatricJenniffer FlorenciaNo ratings yet
- Cardio Case Study 11Document5 pagesCardio Case Study 11api-646131765No ratings yet
- Fdar ActionsDocument3 pagesFdar ActionsClaire LimosNo ratings yet
- Table 16-3 - Nonopioid AnalgesicsDocument1 pageTable 16-3 - Nonopioid AnalgesicsDragutin PetrićNo ratings yet
- ERAS Visual AbstractsDocument15 pagesERAS Visual AbstractssaukimirzaNo ratings yet
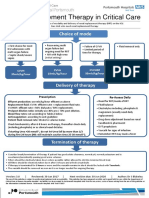
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- H MoleDocument3 pagesH Molemark OrpillaNo ratings yet
- 1st Half GORDON FUNCTIONAL HEALTH PATTERN - Head InjuryDocument2 pages1st Half GORDON FUNCTIONAL HEALTH PATTERN - Head InjuryTerence SalamatNo ratings yet
- Initial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentDocument3 pagesInitial Full-Dose Heparin For Adult: 1-Venous Thromboembolism (DVT/PE), TreatmentLamNo ratings yet
- FDARDocument3 pagesFDARbeefy school onlyNo ratings yet
- IBD With Surgical Intervention: Pre-And Postoperative ManagementDocument2 pagesIBD With Surgical Intervention: Pre-And Postoperative ManagementJavier GlezqNo ratings yet
- Hospital Treatment Protocol For Covid-19Document4 pagesHospital Treatment Protocol For Covid-19Adrian BoboceaNo ratings yet
- AcetaminophenDocument1 pageAcetaminophensalwakh266No ratings yet
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
- ASA Physical Status ClassificationDocument5 pagesASA Physical Status Classificationpolushky100% (1)
- 5 Pre Op CS & Major Surgery 22.06.2015Document5 pages5 Pre Op CS & Major Surgery 22.06.2015Mahesh RathnayakeNo ratings yet
- Electrolyte Replacement Infusions Pediatrics 0713Document2 pagesElectrolyte Replacement Infusions Pediatrics 0713Hakobito Dela RosaNo ratings yet
- CVD Protocol ENGLISHDocument2 pagesCVD Protocol ENGLISHCornel ComanNo ratings yet
- Surgery Nursing Patient AnesthesiaDocument2 pagesSurgery Nursing Patient AnesthesiaTri Mardiana MahaNo ratings yet
- Date 13-8-20 2 Floor Ext.: 6431Document4 pagesDate 13-8-20 2 Floor Ext.: 6431Ali El SafadiNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- NSD: 2 NSD DayDocument3 pagesNSD: 2 NSD Day'jan JanNo ratings yet
- O&G Off-Tag Assesment Logbook: Traces-Pdf-248732173Document9 pagesO&G Off-Tag Assesment Logbook: Traces-Pdf-248732173niwasNo ratings yet
- Patient Units Severe Sepsis Screening ToolDocument2 pagesPatient Units Severe Sepsis Screening ToolArnelli HutagalungNo ratings yet
- Antibiotic ProtocolDocument37 pagesAntibiotic ProtocolSrinivas VadtheNo ratings yet
- Dopamine - IV AdministrationDocument4 pagesDopamine - IV AdministrationAlexandra RainNo ratings yet
- Pediatric ER Standing Order ProtocolsDocument2 pagesPediatric ER Standing Order ProtocolsCharlene FernándezNo ratings yet
- ERAS ChecklistDocument7 pagesERAS ChecklistHazImnike IGniteNo ratings yet
- NH Protocol For Covid Management FinalDocument7 pagesNH Protocol For Covid Management FinalhoneyworksNo ratings yet
- Case PCAPDocument2 pagesCase PCAPNina Anne ParacadNo ratings yet
- Case Study: Medical Colleges of Northern PhilippinesDocument16 pagesCase Study: Medical Colleges of Northern Philippinesmark OrpillaNo ratings yet
- Hospital Treatment Protocol For Covid-19Document2 pagesHospital Treatment Protocol For Covid-19Nandor KissNo ratings yet
- Module 2 - Case 1Document9 pagesModule 2 - Case 1Joselyn M. LachicaNo ratings yet
- Module 3 - Case 1Document9 pagesModule 3 - Case 1Joselyn M. LachicaNo ratings yet
- Week 1 Heparin Examples With AnswersDocument20 pagesWeek 1 Heparin Examples With Answersمريم حجيNo ratings yet
- Risk Management Framework at DCB BankDocument10 pagesRisk Management Framework at DCB BankRavi KumarNo ratings yet
- Pointy Hat - The Cowboy - Ranger ConclaveDocument5 pagesPointy Hat - The Cowboy - Ranger Conclave678ojyhiopNo ratings yet
- UNIT-5 ppspNOTESDocument29 pagesUNIT-5 ppspNOTESEverbloom EverbloomNo ratings yet
- Business Income Calculation UdomDocument23 pagesBusiness Income Calculation UdomMaster Kihimbwa100% (1)
- Jeselo O. Gorme, RN, MNDocument109 pagesJeselo O. Gorme, RN, MNcoosa liquorsNo ratings yet
- Islam in The Middle Ages - WORKSHEETDocument4 pagesIslam in The Middle Ages - WORKSHEETcrabbydreamerNo ratings yet
- Lab Report 2Document3 pagesLab Report 2Shah jalalNo ratings yet
- Lindsey Position PaperDocument14 pagesLindsey Position PaperRamil DumasNo ratings yet
- Information Processing 2Document6 pagesInformation Processing 2Owen RamiscalNo ratings yet
- Darfur Now Not On Our Watch Teaching UnitDocument73 pagesDarfur Now Not On Our Watch Teaching UnitFacing History and Ourselves100% (12)
- 312 Listening List III FinalDocument2 pages312 Listening List III FinalJakeNo ratings yet
- Antacyd PDFDocument5 pagesAntacyd PDFIra YunrarzNo ratings yet
- Print Book FinalDocument25 pagesPrint Book FinalKhurram AliNo ratings yet
- David Acheson - The Digital Defamation Damages DilemmaDocument16 pagesDavid Acheson - The Digital Defamation Damages DilemmaDavid AchesonNo ratings yet
- Containers For Every Need: Maersk Equipment GuideDocument12 pagesContainers For Every Need: Maersk Equipment GuideSharath RadhakrishnanNo ratings yet
- Villaseñor vs. AbanoDocument2 pagesVillaseñor vs. AbanoFrancess PiloneoNo ratings yet
- Summer ReadingDocument1 pageSummer ReadingDonna GurleyNo ratings yet
- Quantitative Reasearch KINDS OF RESEARCHDocument1 pageQuantitative Reasearch KINDS OF RESEARCHEivie SonioNo ratings yet
- Second SundayDocument6 pagesSecond SundayAlfred LochanNo ratings yet
- Potter's House Christian FellowshipDocument12 pagesPotter's House Christian Fellowshipwattssteve21No ratings yet
- Walt Disney BiographyDocument8 pagesWalt Disney BiographyIsaacRodríguezNo ratings yet
- Bank of South Sudan Act, 2011 - Bank of South SudanDocument59 pagesBank of South Sudan Act, 2011 - Bank of South SudanAnnadevaraNageswararaoNo ratings yet
- NPJH50465Document3 pagesNPJH50465Samuel PerezNo ratings yet