You might also like
- The Icon Ficha EditávelDocument2 pagesThe Icon Ficha EditávelRenato CarvalhoNo ratings yet
- 4.section 3 - Routine MaintenanceDocument96 pages4.section 3 - Routine MaintenanceMyo minNo ratings yet
- Laboratory Procedure Prescription: RetainersDocument1 pageLaboratory Procedure Prescription: Retainersdrmohamad drmohamadNo ratings yet
- RX Dentist BiotempsDocument2 pagesRX Dentist BiotempsdamingeniusNo ratings yet
- RX Dentist Itrs Final RestorationDocument1 pageRX Dentist Itrs Final RestorationdamingeniusNo ratings yet
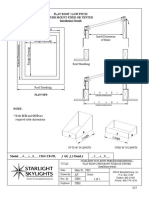
- FlatDocument1 pageFlatNoha GamalNo ratings yet
- 330C D 336D Final Drive Spec Sheet 11 8 18 Hi ResDocument2 pages330C D 336D Final Drive Spec Sheet 11 8 18 Hi ResJean Claude EidNo ratings yet
- Please Attached For Con: Project Name Location: ....... Floor Carpark Area: Date: Daswin Office Tower ProjectDocument4 pagesPlease Attached For Con: Project Name Location: ....... Floor Carpark Area: Date: Daswin Office Tower ProjectWahyu Rohmad DiantoNo ratings yet
- RX Dentist RemovableDocument2 pagesRX Dentist RemovabledamingeniusNo ratings yet
- Form Commtest TADocument9 pagesForm Commtest TAAdi SusenoNo ratings yet
- Coming Apart - Playbooks (PbtA)Document9 pagesComing Apart - Playbooks (PbtA)JUDGENo ratings yet
- Aichi Boom Lifts Telescopic Spec 823132Document2 pagesAichi Boom Lifts Telescopic Spec 823132sebastian romanNo ratings yet
- Structural ModelingDocument21 pagesStructural ModelingWilbert ReuyanNo ratings yet
- 3 AmadeusAlteaNDC SeatAvailability 18.1 ImplementationGuide 20230623Document81 pages3 AmadeusAlteaNDC SeatAvailability 18.1 ImplementationGuide 20230623thanhhuyenNo ratings yet
- Catalog KennametalDocument749 pagesCatalog KennametalTrí PhạmNo ratings yet
- 2019 Version ComparisonDocument1 page2019 Version Comparisonsathiya priyaNo ratings yet
- Casa de La Calidad QFDDocument33 pagesCasa de La Calidad QFDCristian MosqueraNo ratings yet
- Biobase Microscope BrochureDocument3 pagesBiobase Microscope BrochureJim DonaireNo ratings yet
- Specification For Instrument Cable: Pecification For Nstrument AbleDocument18 pagesSpecification For Instrument Cable: Pecification For Nstrument Ableamini_mohiNo ratings yet
- PD-F 03 .Engineering Change Note - Internal & Sup. InitiationDocument2 pagesPD-F 03 .Engineering Change Note - Internal & Sup. InitiationHarjeet SinghNo ratings yet
- MBV - Products - List V-Belt VNDocument1 pageMBV - Products - List V-Belt VNSteven PhamNo ratings yet
- Copy of JEA HIRAC TemplateDocument11 pagesCopy of JEA HIRAC TemplateWilliam BautistaNo ratings yet
- Specification For Temperature Element/Instrument: S T E / IDocument14 pagesSpecification For Temperature Element/Instrument: S T E / Iamini_mohiNo ratings yet
- Welder Worksheet - ASME - SMAW - 6GDocument2 pagesWelder Worksheet - ASME - SMAW - 6GKarim ZahranNo ratings yet
- Dokumen - Tips - Octopus 300 Octopus Perimetry You Can Trust Swiss 300 Octopus 900 11 OctopusDocument14 pagesDokumen - Tips - Octopus 300 Octopus Perimetry You Can Trust Swiss 300 Octopus 900 11 OctopusItiNo ratings yet
- Manual de Operacion MotorDocument27 pagesManual de Operacion MotorMileidy Severiche AvilaNo ratings yet
- Ficha Instalacion Dock Levelers Specs MechDocument2 pagesFicha Instalacion Dock Levelers Specs MechKelvin ToledoNo ratings yet
- Final Enquiry List For ValvesDocument12 pagesFinal Enquiry List For ValvesnikhilNo ratings yet
- P111 - CBP Cost EstimateDocument17 pagesP111 - CBP Cost EstimateAmmar KhuderNo ratings yet
- Camshaft MeasurementDocument1 pageCamshaft Measurementesa masivNo ratings yet
- Catálogo 37FSDocument6 pagesCatálogo 37FSMarcos Marcandali de JesusNo ratings yet
- MIP17 Confined Space Entry PlanDocument3 pagesMIP17 Confined Space Entry PlanAmeerHamzaWarraichNo ratings yet
- Checklist of Enclose-Rev00Document1 pageChecklist of Enclose-Rev00muth sokvisalNo ratings yet
- 17052023-Layout DB Wing 01 RDocument78 pages17052023-Layout DB Wing 01 RSann SeyhaNo ratings yet
- GKM Series (Global Miniature Safety Key Interlock Switch) : FeaturesDocument100 pagesGKM Series (Global Miniature Safety Key Interlock Switch) : FeaturesyonesNo ratings yet
- Aws Qc13 2006 Specification For The Certification of Welding SupervisorsDocument1 pageAws Qc13 2006 Specification For The Certification of Welding SupervisorsEdmilson FaustinoNo ratings yet
- Marco GDocument3 pagesMarco GMAEBNo ratings yet
- Pin BorDocument1 pagePin Borsofiatun khoirohNo ratings yet
- Gear Data For 71400418Document2 pagesGear Data For 71400418Pratap ThakurNo ratings yet
- GMA Garnet Blast Abrasive Product LineDocument6 pagesGMA Garnet Blast Abrasive Product Linetokyo casaNo ratings yet
- Hub Seal Reference Chart: FootnotesDocument2 pagesHub Seal Reference Chart: FootnotesLuis OvandoNo ratings yet
- Thermocouple Te 101 A-FDocument2 pagesThermocouple Te 101 A-Friswan nugrahaNo ratings yet
- LP - Abrasive and Water Blasting Plan - Best Practice - Form - v2 - RTRDocument5 pagesLP - Abrasive and Water Blasting Plan - Best Practice - Form - v2 - RTRawq.pablo90No ratings yet
- JSA - Main Turbine Lub Oil Pumps - OHDocument2 pagesJSA - Main Turbine Lub Oil Pumps - OHShubham Gupta0% (1)
- Finitura Flange e GuarnizioniDocument1 pageFinitura Flange e GuarnizioniBrooke CraigNo ratings yet
- IPG Laser Welding D30 D50 Wobble BrochureDocument6 pagesIPG Laser Welding D30 D50 Wobble BrochureSinthu ChanthapanNo ratings yet
- 12th Physics - One ShotDocument74 pages12th Physics - One ShotKaranNo ratings yet
- MGT7 Eco SetupDocument1 pageMGT7 Eco Setupmarcelo.salamaNo ratings yet
- Sylax Gas B: Technical ManualDocument15 pagesSylax Gas B: Technical Manualseeralan_1986No ratings yet
- CDC-rupture Disk Product-Selection-Guide-1Document24 pagesCDC-rupture Disk Product-Selection-Guide-1Thefairman UnkownNo ratings yet
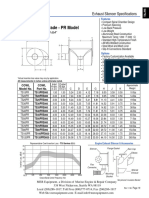
- TS PR Residential SeriesDocument2 pagesTS PR Residential SeriesGégé di TPNo ratings yet
- Classroom Repair and Mentenance ReportDocument2 pagesClassroom Repair and Mentenance ReportAlbertoPeraltaNo ratings yet
- Om-03 Hose Handling Crane PDFDocument126 pagesOm-03 Hose Handling Crane PDFcpîndaruNo ratings yet
- Lmo, Lmovs Lmo HP Lmo VHP: Installation AND Operating InstructionsDocument12 pagesLmo, Lmovs Lmo HP Lmo VHP: Installation AND Operating InstructionsVaibhav ChauhanNo ratings yet
- Digital SAT Prep in CaliforniaDocument18 pagesDigital SAT Prep in Californiasarika523No ratings yet
- DriveTechnology p174 p193 Steel Laminae CouplingsDocument20 pagesDriveTechnology p174 p193 Steel Laminae CouplingsNhật Quang PhạmNo ratings yet
- Composite p715g PDFDocument44 pagesComposite p715g PDFAlexandre SouzaNo ratings yet
- Syllabus DistributionDocument10 pagesSyllabus DistributionTashaNo ratings yet
- InvoiceDocument2 pagesInvoiceNick TurnbullNo ratings yet
- FAQ Change Classification PDFDocument10 pagesFAQ Change Classification PDFmycopteraviationNo ratings yet
- E4-E5 - Text - Chapter 2. ISO 9001-2015 QUALITY MANAGEMENT SYSTEMDocument17 pagesE4-E5 - Text - Chapter 2. ISO 9001-2015 QUALITY MANAGEMENT SYSTEMAGM S&M-CMNo ratings yet
- Mrunal Handout 12 CSP20Document84 pagesMrunal Handout 12 CSP20SREEKANTHNo ratings yet
- TextDocument3 pagesTextKristineNo ratings yet
- CNA Candidate HandbookDocument57 pagesCNA Candidate HandbookSummerNo ratings yet
- UNIT 3 Polymer and Fuel ChemistryDocument10 pagesUNIT 3 Polymer and Fuel Chemistryld6225166No ratings yet
- DoveDocument11 pagesDovekattyperrysherryNo ratings yet
- Sialoree BotoxDocument5 pagesSialoree BotoxJocul DivinNo ratings yet
- Ppr.1 Circ.5 Gesamp Ehs ListDocument93 pagesPpr.1 Circ.5 Gesamp Ehs ListTRANNo ratings yet
- Esc200 12Document1 pageEsc200 12Anzad AzeezNo ratings yet
- Diagnostic Evaluation and Management of The Solitary Pulmonary NoduleDocument21 pagesDiagnostic Evaluation and Management of The Solitary Pulmonary NoduleGonzalo Leal100% (1)
- 27nov12 PA Task Force On Child Protection ReportDocument445 pages27nov12 PA Task Force On Child Protection ReportDefendAChildNo ratings yet
- 2-Phase Synchronous-Rectified Buck Controller For Mobile GPU PowerDocument18 pages2-Phase Synchronous-Rectified Buck Controller For Mobile GPU PowerMax Assistência TécnicaNo ratings yet
- Keandalan Bangunan Rumah SusunDocument9 pagesKeandalan Bangunan Rumah SusunDewi ARimbiNo ratings yet
- Module 6 - Addictions Prayer ServiceDocument6 pagesModule 6 - Addictions Prayer Serviceapi-450520432No ratings yet
- Choke Manifold Procedures 3932324 01Document4 pagesChoke Manifold Procedures 3932324 01Saïd Ben Abdallah100% (1)
- Electrolux EKF7700 Coffee MachineDocument76 pagesElectrolux EKF7700 Coffee MachineTudor Sergiu AndreiNo ratings yet
- SPKT Thiet Ke Co Khi 1Document33 pagesSPKT Thiet Ke Co Khi 1Chiến PhanNo ratings yet
- Resume - Arun BhartiDocument3 pagesResume - Arun BhartiArun AbNo ratings yet
- Material Specification: Mechanical Property RequirementsDocument2 pagesMaterial Specification: Mechanical Property RequirementsNguyễn Tấn HảiNo ratings yet
- Practice Test: Ielts UsaDocument11 pagesPractice Test: Ielts UsajoseNo ratings yet
- Damasco - Cpi - Activity No. 10Document18 pagesDamasco - Cpi - Activity No. 10LDCU - Damasco, Erge Iris M.No ratings yet
- Mediclinic Weekly Progress Report No 29Document27 pagesMediclinic Weekly Progress Report No 29Julius Ceasar SanorjoNo ratings yet
- Mental Health & TravelDocument18 pagesMental Health & TravelReyza HasnyNo ratings yet
- Big Elephants Are Useful Mnemonics & IdiomsDocument144 pagesBig Elephants Are Useful Mnemonics & IdiomsNachoAndrésLlorente100% (1)
- Northbrook CollegeDocument10 pagesNorthbrook CollegeDaniyal AsifNo ratings yet
- Canfield FairDocument3 pagesCanfield Fairapi-546463844No ratings yet
- Agriculture and FisheryDocument5 pagesAgriculture and FisheryJolliven JamiloNo ratings yet
- Radial Lead Varistors LA Varistor SeriesDocument13 pagesRadial Lead Varistors LA Varistor SeriesLeman SihotangNo ratings yet