You might also like
- Permaculture - Plants Suitable For Ground Cover (P) - Plants For A FutureDocument2 pagesPermaculture - Plants Suitable For Ground Cover (P) - Plants For A Futurecontadino_impazzitoNo ratings yet
- Graha YuddhaDocument10 pagesGraha YuddhaHeather WilliamsNo ratings yet
- MRI of The Breast and Emerging TechnologiesDocument15 pagesMRI of The Breast and Emerging Technologiesგიორგი ჯიქიძე100% (1)
- Heat Sink Capacity Mesurment in Inservice PipelineDocument13 pagesHeat Sink Capacity Mesurment in Inservice PipelineSomeshNo ratings yet
- Quarter3 English ModuleDocument6 pagesQuarter3 English ModuleIan Daquipil100% (2)
- Polynesian MigrationsDocument2 pagesPolynesian Migrationskinneyjeffrey100% (1)
- CardiomyopathyDocument1 pageCardiomyopathyTrisha VergaraNo ratings yet
- Poulos, A., & McLean, D. (2004) - The Application of Breast ...Document7 pagesPoulos, A., & McLean, D. (2004) - The Application of Breast ...casscactusNo ratings yet
- Digital Mammography Novel Applications. Radiologic Clinics of North AmericaDocument13 pagesDigital Mammography Novel Applications. Radiologic Clinics of North AmericaEduardo Alejandro IIINo ratings yet
- Articulo de Cancer de Mama 2Document2 pagesArticulo de Cancer de Mama 2Brigitte GutierrezNo ratings yet
- External Validation of A Deep Learning Model For Predicting Mammographic Breast Density in Routine Clinical PracticeDocument6 pagesExternal Validation of A Deep Learning Model For Predicting Mammographic Breast Density in Routine Clinical PracticehaiminalNo ratings yet
- Density and Tailored Breast Cancer Screening: Practice and Prediction - An OverviewDocument12 pagesDensity and Tailored Breast Cancer Screening: Practice and Prediction - An Overviewelisabeth harahapNo ratings yet
- Abdominal Ultrasound For Pediatric Blunt Trauma FAST Is Not Always BetterDocument3 pagesAbdominal Ultrasound For Pediatric Blunt Trauma FAST Is Not Always BetterInryuu ZenNo ratings yet
- Detection and Characterization of Breast Masses With Ultrasound Tomography - Clinical Results - Duric Et Al - 2009Document8 pagesDetection and Characterization of Breast Masses With Ultrasound Tomography - Clinical Results - Duric Et Al - 2009samouille6666No ratings yet
- Contrast Enhancement in Breast Cancer and Background Mammary-Gland Tissue During The Super-Early Phase of Dynamic Breast Magnetic Resonance ImagingDocument7 pagesContrast Enhancement in Breast Cancer and Background Mammary-Gland Tissue During The Super-Early Phase of Dynamic Breast Magnetic Resonance ImagingBenitaNo ratings yet
- SurveyDocument18 pagesSurveyসাঁচিপাট অসমNo ratings yet
- Berger 2007Document9 pagesBerger 2007Benfredj KhalilNo ratings yet
- Ijerph 19 00759Document10 pagesIjerph 19 00759Choi Min YoungNo ratings yet
- Application of Computer-Aided Diagnosis On Breast UltrasonographyDocument8 pagesApplication of Computer-Aided Diagnosis On Breast UltrasonographySummrina KanwalNo ratings yet
- Potential Impact of Tomosynthesis On The Detection and Diagnosis of Breast LesionsDocument11 pagesPotential Impact of Tomosynthesis On The Detection and Diagnosis of Breast LesionsMR Emam - GamingNo ratings yet
- Beriwal 2006Document5 pagesBeriwal 2006Bruno MendesNo ratings yet
- Self-Compression Technique Vs Standard Compression in Mammographya Randomized Clinical TrialDocument13 pagesSelf-Compression Technique Vs Standard Compression in Mammographya Randomized Clinical TrialMonica Afrillies HardianiNo ratings yet
- IdentifyinggapsDocument6 pagesIdentifyinggapsapi-426094285No ratings yet
- Role of MRI in The Staging of Breast Cancer Patients: Does Histological Type and Molecular Subtype Matter?Document6 pagesRole of MRI in The Staging of Breast Cancer Patients: Does Histological Type and Molecular Subtype Matter?Ther RayNo ratings yet
- BSGIstudiesDocument40 pagesBSGIstudiessayed hossein hashemiNo ratings yet
- Diffusion WeightedDocument27 pagesDiffusion WeightedDaniela FerrariNo ratings yet
- Consensus Guideline On Breast Cancer Lumpectomy MarginsDocument6 pagesConsensus Guideline On Breast Cancer Lumpectomy MarginsSubhamSarthakNo ratings yet
- D R Dance 2000 Phys. Med. Biol. 45 308Document17 pagesD R Dance 2000 Phys. Med. Biol. 45 308Erika Xiomara Cely SeguraNo ratings yet
- Image Features of True Positive and False Negative Cancers in Screening MammogramsDocument9 pagesImage Features of True Positive and False Negative Cancers in Screening MammogramsTher RayNo ratings yet
- 1 s2.0 S0360301619303165 Main PDFDocument9 pages1 s2.0 S0360301619303165 Main PDFmuhsyaifulNo ratings yet
- Comparative Effectiveness of Digital Breast Tomosynthesis For Breast Cancer Screening Among Women 40-64 Years OldDocument8 pagesComparative Effectiveness of Digital Breast Tomosynthesis For Breast Cancer Screening Among Women 40-64 Years OldAmalia fhyNo ratings yet
- Comparison of Ultrasound and Mammography For Early DiagnosisDocument8 pagesComparison of Ultrasound and Mammography For Early Diagnosishdh1224No ratings yet
- De Faria Castro Fleury Et Al 2022 Management of Non Mass Enhancement at Breast Magnetic Resonance in Screening SettingsDocument9 pagesDe Faria Castro Fleury Et Al 2022 Management of Non Mass Enhancement at Breast Magnetic Resonance in Screening Settingsdr.elahe.babantaherNo ratings yet
- Case-Control Study of Mammographic Density and Breast Cancer Risk Using Processed Digital MammogramsDocument4 pagesCase-Control Study of Mammographic Density and Breast Cancer Risk Using Processed Digital MammogramsEmasHarnasAkbarNo ratings yet
- Radiol 2019181753Document10 pagesRadiol 2019181753Esteban PalaciosNo ratings yet
- CM 93 335Document7 pagesCM 93 335Sol Valeria Mejia GarciaNo ratings yet
- The Role of Nonenhanced Mri in Measuring Flap Volume Variability in Postbariatric Women After Mastopexy With Autologous Tissue Aug 2161 1173Document5 pagesThe Role of Nonenhanced Mri in Measuring Flap Volume Variability in Postbariatric Women After Mastopexy With Autologous Tissue Aug 2161 1173Anonymous 3dbJapZ9i0No ratings yet
- Benefits, Harms, and Cost-Effectiveness of Supplemental Ultrasonography Screening For Women With Dense BreastsDocument15 pagesBenefits, Harms, and Cost-Effectiveness of Supplemental Ultrasonography Screening For Women With Dense BreastsHarshoi KrishannaNo ratings yet
- Organ and Effective Dose Reduction in Adult Chest CT UsingDocument7 pagesOrgan and Effective Dose Reduction in Adult Chest CT UsingIshani Anushika JayakodyNo ratings yet
- Paper Third DraftDocument19 pagesPaper Third Draftapi-405398222No ratings yet
- Mri - Best Practice - Bisi - 2020 PDFDocument7 pagesMri - Best Practice - Bisi - 2020 PDFBISI IndiaNo ratings yet
- Ditkofsky 2015Document28 pagesDitkofsky 2015Allython Jureth Peña ReyesNo ratings yet
- MAIN REVIEW Zugasti and Hontanilla 2021Document11 pagesMAIN REVIEW Zugasti and Hontanilla 2021Walid SasiNo ratings yet
- Final CapstoneDocument11 pagesFinal Capstoneapi-603721790No ratings yet
- Nishele Lenards, PHD, CMD, RT (R) (T), FaamdDocument8 pagesNishele Lenards, PHD, CMD, RT (R) (T), Faamdapi-450246598No ratings yet
- Xu 2021Document9 pagesXu 2021Drsaumyta MishraNo ratings yet
- Journal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardDocument6 pagesJournal of Surgical Oncology - 2013 - Fortunato - When Mastectomy Is Needed Is The Nipple Sparing Procedure A New StandardJethro ConcepcionNo ratings yet
- Article: Prevalence of Women With Dense Breasts in Korea: Results From A Nationwide Cross-Sectional StudyDocument18 pagesArticle: Prevalence of Women With Dense Breasts in Korea: Results From A Nationwide Cross-Sectional StudyDani PairaNo ratings yet
- Comparison of Dose Volume Parameters Evaluated UsiDocument15 pagesComparison of Dose Volume Parameters Evaluated UsiBenfredj KhalilNo ratings yet
- 1 s2.0 S174868151730181X MainDocument9 pages1 s2.0 S174868151730181X MainChiara BoccalettoNo ratings yet
- 5 +diastase+e+gestac A oDocument9 pages5 +diastase+e+gestac A oJuliana MariaNo ratings yet
- Breast Imaging Outcomes Following Abnormal ThermographyDocument6 pagesBreast Imaging Outcomes Following Abnormal ThermographyJuan José Delgado QuesadaNo ratings yet
- Ijcmr 1184 Dec 28Document3 pagesIjcmr 1184 Dec 28BayuHernawanRahmatMuhariaNo ratings yet
- Tiwari 2017Document3 pagesTiwari 2017Dewa OkaNo ratings yet
- Final Draft2 Group10 10-24Document24 pagesFinal Draft2 Group10 10-24api-602263051No ratings yet
- Optical Imaging InbreastsDocument11 pagesOptical Imaging InbreastsCezara RasinarNo ratings yet
- Beriwal Et Al 2006 Comparison of 2d Vs 3d Dosimetry For Rotte y Applicator High Dose Rate Brachytherapy For MedicallyDocument7 pagesBeriwal Et Al 2006 Comparison of 2d Vs 3d Dosimetry For Rotte y Applicator High Dose Rate Brachytherapy For MedicallyMilda InayahNo ratings yet
- A Representation For Mammographic Image Processing: Ralph Highnam, Michael Brady and Basil ShepstoneDocument18 pagesA Representation For Mammographic Image Processing: Ralph Highnam, Michael Brady and Basil ShepstoneMario SansoneNo ratings yet
- Poljradiol 81 415Document7 pagesPoljradiol 81 415Moe Wai MyintNo ratings yet
- Estro AcropDocument12 pagesEstro AcropAndreyson SilvaNo ratings yet
- 1 s2.0 S2405632423000197 MainDocument11 pages1 s2.0 S2405632423000197 Mainsaros22568No ratings yet
- Breast Imaging - Mammography and UltrasonographyDocument24 pagesBreast Imaging - Mammography and UltrasonographyhozainNo ratings yet
- Group 1 Draft IIDocument9 pagesGroup 1 Draft IIapi-450475136No ratings yet
- Contrast-Enhanced MammographyFrom EverandContrast-Enhanced MammographyMarc LobbesNo ratings yet
- Supine Breast MRIDocument6 pagesSupine Breast MRIpunct_org3256No ratings yet
- 816-Article Text-5949-1-10-20230609Document6 pages816-Article Text-5949-1-10-20230609NikadekPramesti Dewi Puspita SariNo ratings yet
- Role of Medical Education in Cultivating LifelongDocument4 pagesRole of Medical Education in Cultivating LifelongRudolph SunnydaysNo ratings yet
- Pub 4Document6 pagesPub 4Rudolph SunnydaysNo ratings yet
- Pub 3Document5 pagesPub 3Rudolph SunnydaysNo ratings yet
- An Assessment of Medical Students Proficiency RegDocument8 pagesAn Assessment of Medical Students Proficiency RegRudolph SunnydaysNo ratings yet
- Assessment of Health Care Providers Knowledge, Attitude and Practice Towards Professional Ethics in Public and Private Health Facilities in Ambo Town, Central Ethiopia, 2016Document9 pagesAssessment of Health Care Providers Knowledge, Attitude and Practice Towards Professional Ethics in Public and Private Health Facilities in Ambo Town, Central Ethiopia, 2016Rudolph SunnydaysNo ratings yet
- Doosan Dielsel Forklift d35s 7 d40s 7 d45s 7 d50c 7 d55c 7 d40sc 7 d45sc 7 d50sc 7 d55sc 7 Part Book Sb1223e01Document22 pagesDoosan Dielsel Forklift d35s 7 d40s 7 d45s 7 d50c 7 d55c 7 d40sc 7 d45sc 7 d50sc 7 d55sc 7 Part Book Sb1223e01daleherrera100788nke100% (23)
- Sa 387Document6 pagesSa 387ismaelarchilacastilloNo ratings yet
- CekocideDocument1 pageCekocideKaren Claire HorcaNo ratings yet
- Fishery MachinesDocument9 pagesFishery Machinesirshad hussainNo ratings yet
- Criaturas Do Reino DistanteDocument53 pagesCriaturas Do Reino DistanteDaniel Marinho100% (1)
- Herpes Simplex KeratitisDocument20 pagesHerpes Simplex KeratitisriskhapangestikaNo ratings yet
- GD - 202011 - G2 Inverter - Sungrow Single Phase Inverter Commissioning Guide - V1.0Document13 pagesGD - 202011 - G2 Inverter - Sungrow Single Phase Inverter Commissioning Guide - V1.0AbbasNo ratings yet
- AE240 Notes Early-Airfoil-Development-Handout-1Document5 pagesAE240 Notes Early-Airfoil-Development-Handout-1mohamedNo ratings yet
- Appendix 2-4.ep31422 - g-16Document15 pagesAppendix 2-4.ep31422 - g-16bsnegi111No ratings yet
- uPASS Target: Installation GuideDocument40 pagesuPASS Target: Installation GuideMohammed ElsayedNo ratings yet
- GFRC Floating Concrete Hearth For Concrete Wood FiDocument11 pagesGFRC Floating Concrete Hearth For Concrete Wood FiJuliano. PQMNo ratings yet
- Proline Table-Top Machines Z005 Up To Z100: Product InformationDocument2 pagesProline Table-Top Machines Z005 Up To Z100: Product InformationErika Mae EnticoNo ratings yet
- Bubble Slabs Burned at 800 °C With Different Periods: IOP Conference Series: Materials Science and EngineeringDocument10 pagesBubble Slabs Burned at 800 °C With Different Periods: IOP Conference Series: Materials Science and Engineeringshilpa jacobNo ratings yet
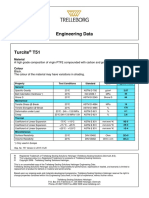
- Turcite T51 Engineering DataDocument1 pageTurcite T51 Engineering DataAntonio Rivera VillavicencioNo ratings yet
- Example Lab ReportDocument12 pagesExample Lab ReportHung Dang QuangNo ratings yet
- Measure Guide Air Cond DiagnosticsDocument70 pagesMeasure Guide Air Cond Diagnosticsayad60No ratings yet
- Mesoamerica: Where Civilizations Flourished, and Crashed, RepeatedlyDocument8 pagesMesoamerica: Where Civilizations Flourished, and Crashed, RepeatedlyEnvyAmarr •No ratings yet
- Mita Lifestyle Agenda ContentDocument263 pagesMita Lifestyle Agenda Contentnacentral13517No ratings yet
- Modules With Available Quota - 2019!11!12 - 9amDocument7 pagesModules With Available Quota - 2019!11!12 - 9amdhmanoharNo ratings yet
- A 388 - A 388M - 03 - Qtm4oc9bmzg4tqDocument8 pagesA 388 - A 388M - 03 - Qtm4oc9bmzg4tqRod RoperNo ratings yet
- EngineeringDocument107 pagesEngineeringSuezakumeNo ratings yet
- Numerology 666 Meaning: What Angel Number 666 REALLY Means!Document2 pagesNumerology 666 Meaning: What Angel Number 666 REALLY Means!LlNo ratings yet
- Matter 1A Forms Properties and ChangesDocument47 pagesMatter 1A Forms Properties and ChangesSamKris Guerrero Malasaga100% (2)
- Cause and Effect PowerpointDocument20 pagesCause and Effect PowerpointSherly V.LizardoNo ratings yet