You might also like
- Introduction To TCCC ASM Didactic PresentationDocument36 pagesIntroduction To TCCC ASM Didactic PresentationPaulo De Fão SousaNo ratings yet
- Introduction To TCCC ASM Didactic Presentation (With Videos)Document43 pagesIntroduction To TCCC ASM Didactic Presentation (With Videos)thallesnetNo ratings yet
- Module 04 - Principles and Application of TFC: Speaker NotesDocument7 pagesModule 04 - Principles and Application of TFC: Speaker NotesSae Tum100% (1)
- Intro To Tactical MedicineDocument70 pagesIntro To Tactical MedicinePaula Pinto Beerens100% (4)
- Chapter 1 Tactical Combat Casualty CareDocument52 pagesChapter 1 Tactical Combat Casualty Care120v60hz100% (1)
- Pre-Hospital Trauma CareDocument8 pagesPre-Hospital Trauma Carecorsaru100% (1)
- TCCCDocument117 pagesTCCCthallesnet100% (3)
- Tactical Casualty Combat Care Handbook v5 PDFDocument133 pagesTactical Casualty Combat Care Handbook v5 PDFJose Torres100% (5)
- Acute Respiratory Failure Lecture 2014-2015 (5!1!14) FINALDocument60 pagesAcute Respiratory Failure Lecture 2014-2015 (5!1!14) FINALrentedmule00No ratings yet
- Silver Sol TechnologyDocument2 pagesSilver Sol Technologyapi-261829418No ratings yet
- Questionnaire (ISBB)Document14 pagesQuestionnaire (ISBB)Angelo Mercede100% (2)
- Module 01 - SpeakerDocument9 pagesModule 01 - SpeakerRoger RonconiNo ratings yet
- Module 14 - Analgesia and Antibiotic Administration: Speaker NotesDocument5 pagesModule 14 - Analgesia and Antibiotic Administration: Speaker NotesSae TumNo ratings yet
- Asm Course Speaker NotesDocument15 pagesAsm Course Speaker NotesJesse RobertNo ratings yet
- Module 02 - Medical Equipment: Speaker NotesDocument7 pagesModule 02 - Medical Equipment: Speaker NotesDERIL PRASETYONo ratings yet
- Module 02 - Medical Equipment: Speaker NotesDocument7 pagesModule 02 - Medical Equipment: Speaker NotesDERIL PRASETYONo ratings yet
- Performing Tactical Combat Casualty CareDocument12 pagesPerforming Tactical Combat Casualty CareRich AdamsNo ratings yet
- TCCC CourseDocument22 pagesTCCC CourseSteve Fetalino Demaala100% (1)
- Combat Life Saver Module 1: OverviewDocument14 pagesCombat Life Saver Module 1: Overviewsrtmedic100% (2)
- United States Marine Corps: Introduction To Tactical Combat Casualty CareDocument10 pagesUnited States Marine Corps: Introduction To Tactical Combat Casualty CareHaris Pratama RebornNo ratings yet
- 010303A TCCC-MP Tactical Field Care #1 IG 160603Document43 pages010303A TCCC-MP Tactical Field Care #1 IG 160603herralainNo ratings yet
- Cuf 03Document23 pagesCuf 03Roland Astudillo CuevaNo ratings yet
- TCCC Cls Didactics Mod 01 - 24 Jun 20Document22 pagesTCCC Cls Didactics Mod 01 - 24 Jun 20Giovanni RossiNo ratings yet
- Tactical Combat Casualty CareDocument93 pagesTactical Combat Casualty CareJoseph carl Bañaria100% (1)
- Module 08 - Respiration Assessment and Management in TFC: Speaker NotesDocument8 pagesModule 08 - Respiration Assessment and Management in TFC: Speaker NotesSae TumNo ratings yet
- Instructor Guide For Introduction To TCCC-MP 180801Document16 pagesInstructor Guide For Introduction To TCCC-MP 180801M. Owen ErwinNo ratings yet
- Module 07 - Airway Management in TFC: Speaker NotesDocument7 pagesModule 07 - Airway Management in TFC: Speaker NotesSae TumNo ratings yet
- Skill Instr Mod 5 JunioDocument5 pagesSkill Instr Mod 5 JunioSae TumNo ratings yet
- Cls Student PDFDocument137 pagesCls Student PDFOzkar ZaldivarNo ratings yet
- Tactical Combat Casualty CareDocument128 pagesTactical Combat Casualty CareAr HongNo ratings yet
- A Proposed Guideline For Tactical Medical Self-Care in The Civilian EnvironmentDocument6 pagesA Proposed Guideline For Tactical Medical Self-Care in The Civilian EnvironmentfreemedicNo ratings yet
- 3 - Care Under Fire ThreatDocument11 pages3 - Care Under Fire ThreatCarlos MaravilhaNo ratings yet
- Care Under Fire: Tactical Combat Casualty Care For Medical Personnel August 2018Document84 pagesCare Under Fire: Tactical Combat Casualty Care For Medical Personnel August 2018alyssaNo ratings yet
- Military TriageDocument23 pagesMilitary TriagemeeniemauNo ratings yet
- Tactical EMSDocument23 pagesTactical EMSafifnordin88No ratings yet
- Cert Ig Unit3 Jan20112Document60 pagesCert Ig Unit3 Jan20112testNo ratings yet
- Module 11 - Hypothermia Prevention: Speaker NotesDocument6 pagesModule 11 - Hypothermia Prevention: Speaker NotesSae TumNo ratings yet
- Point of Wounding CareDocument49 pagesPoint of Wounding CareAr HongNo ratings yet
- 2 Care Under FireDocument92 pages2 Care Under FireИгорь ВасильевичNo ratings yet
- 2 CufDocument98 pages2 CufBruno SilvaNo ratings yet
- 087 Pre Hospital Trauma CareDocument9 pages087 Pre Hospital Trauma CareabbuahmedibbuNo ratings yet
- 7 - Airway Management in TFCDocument18 pages7 - Airway Management in TFCCarlos MaravilhaNo ratings yet
- MD0001 Evacuation in The FieldDocument185 pagesMD0001 Evacuation in The FieldMaria Herciu100% (1)
- Care Under Fire: Skill InstructionsDocument10 pagesCare Under Fire: Skill InstructionsSae TumNo ratings yet
- Care Under Fire: Skill InstructionsDocument10 pagesCare Under Fire: Skill InstructionsSae TumNo ratings yet
- Tactical First Aid 0410+Document265 pagesTactical First Aid 0410+Carlos SanzNo ratings yet
- Hmpe 4 Final PeriodDocument8 pagesHmpe 4 Final PeriodMichael P. CelisNo ratings yet
- Triage Made EasyDocument7 pagesTriage Made EasyCamille Lou Cariaga AbellaNo ratings yet
- Airway Management in TFC: Skill InstructionsDocument8 pagesAirway Management in TFC: Skill InstructionsSae TumNo ratings yet
- 1 Triage NursingDocument28 pages1 Triage NursingRebecca FerolinoNo ratings yet
- Performtacticalcombatcasualtycare 110212013252 Phpapp01Document39 pagesPerformtacticalcombatcasualtycare 110212013252 Phpapp01Alexandre Cássio LopesNo ratings yet
- Trauma-Focused Individual Training: Revised and Updated January 2005Document101 pagesTrauma-Focused Individual Training: Revised and Updated January 2005Mark Cheney100% (2)
- UN FMAC Student HandbookDocument134 pagesUN FMAC Student HandbookernaNo ratings yet
- BLS For TeacherrDocument166 pagesBLS For TeacherrGavinKarl Mianabanatao100% (1)
- Atbf Ista PDFDocument12 pagesAtbf Ista PDFSae TumNo ratings yet
- US Army Medical Course MD0001-200 - Evacuation in The FieldDocument190 pagesUS Army Medical Course MD0001-200 - Evacuation in The FieldGeorges100% (2)
- Tactical Combat Casualty Care 1Document132 pagesTactical Combat Casualty Care 1Andre Aguiar100% (1)
- Tactical Combat Casualty CareDocument114 pagesTactical Combat Casualty Caresrtmedic100% (5)
- Module 16: Burn Treatment: TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document19 pagesModule 16: Burn Treatment: TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Luis-alfredo Perez Bolde HernandezNo ratings yet
- Basic Life SupportDocument46 pagesBasic Life SupportRuruni Kenchin Batusai50% (2)
- Massive Hemorrhage Control in TFC: Skill InstructionsDocument8 pagesMassive Hemorrhage Control in TFC: Skill InstructionsSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 11: Hypothermia PreventionDocument2 pagesSkills Assessment Checklist: MODULE 11: Hypothermia PreventionSae TumNo ratings yet
- One-Person Bag Valve Mask (BVM) : MarchDocument1 pageOne-Person Bag Valve Mask (BVM) : MarchSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 14: Pain Medication and Antibiotic AdministrationDocument2 pagesSkills Assessment Checklist: MODULE 14: Pain Medication and Antibiotic AdministrationSae TumNo ratings yet
- Head-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedDocument1 pageHead-Tilt/Chin-Lift: DO NOT Use If A Spinal or Neck Injury Is SuspectedSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : Skill InstructionsDocument3 pagesPrinciples and Application of Tactical Field Care (TFC) : Skill InstructionsSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : Skill InstructionsDocument3 pagesPrinciples and Application of Tactical Field Care (TFC) : Skill InstructionsSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 19: Pre-Evacuation Procedures, Communication, and DocumentationDocument3 pagesSkills Assessment Checklist: MODULE 19: Pre-Evacuation Procedures, Communication, and DocumentationSae TumNo ratings yet
- Atbf PDFDocument1 pageAtbf PDFSae TumNo ratings yet
- One-Person Drag/Carry: Kit or Arm DragDocument5 pagesOne-Person Drag/Carry: Kit or Arm DragSae TumNo ratings yet
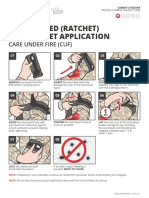
- One-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Document1 pageOne-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Sae TumNo ratings yet
- Atbf Ista PDFDocument12 pagesAtbf Ista PDFSae TumNo ratings yet
- Two-Person Drag/Carry: Kit or Arm DragDocument3 pagesTwo-Person Drag/Carry: Kit or Arm DragSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCDocument7 pagesSkills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 7: Airway ManagementDocument6 pagesSkills Assessment Checklist: MODULE 7: Airway ManagementSae TumNo ratings yet
- Skills Assessment Checklist: MODULE 11: Hypothermia PreventionDocument2 pagesSkills Assessment Checklist: MODULE 11: Hypothermia PreventionSae TumNo ratings yet
- Module 14 - Analgesia and Antibiotic Administration: Speaker NotesDocument5 pagesModule 14 - Analgesia and Antibiotic Administration: Speaker NotesSae TumNo ratings yet
- Two-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Document1 pageTwo-Handed (Ratchet) Tourniquet Application: Care Under Fire (Cuf)Sae TumNo ratings yet
- Skills Assessment Checklist: MODULE 4: Principles and Application of Tactical Field CareDocument1 pageSkills Assessment Checklist: MODULE 4: Principles and Application of Tactical Field CareSae TumNo ratings yet
- Evacuation Procedures: Skill InstructionsDocument3 pagesEvacuation Procedures: Skill InstructionsSae TumNo ratings yet
- Analgesia Administration/ Antibiotic Admin: Skill InstructionsDocument3 pagesAnalgesia Administration/ Antibiotic Admin: Skill InstructionsSae TumNo ratings yet
- Massive Hemorrhage Control in TFC: Skill InstructionsDocument8 pagesMassive Hemorrhage Control in TFC: Skill InstructionsSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document17 pagesPrinciples and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Sae TumNo ratings yet
- Module 11 - Hypothermia Prevention: Speaker NotesDocument6 pagesModule 11 - Hypothermia Prevention: Speaker NotesSae TumNo ratings yet
- Principles and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Document17 pagesPrinciples and Application of Tactical Field Care (TFC) : TCCC Tier 4 TCCC Tier 1 TCCC Tier 3Sae Tum0% (1)
- Massive Hemorrhage Control in TFC: Skill InstructionsDocument8 pagesMassive Hemorrhage Control in TFC: Skill InstructionsSae TumNo ratings yet
- Module 13 - Eye Injuries: Speaker NotesDocument5 pagesModule 13 - Eye Injuries: Speaker NotesSae TumNo ratings yet
- Module 07 - Airway Management in TFC: Speaker NotesDocument7 pagesModule 07 - Airway Management in TFC: Speaker NotesSae TumNo ratings yet
- Eye Injuries: Skill InstructionsDocument3 pagesEye Injuries: Skill InstructionsSae TumNo ratings yet
- Module 08 - Respiration Assessment and Management in TFC: Speaker NotesDocument8 pagesModule 08 - Respiration Assessment and Management in TFC: Speaker NotesSae TumNo ratings yet
- Airway Management in TFC: Skill InstructionsDocument8 pagesAirway Management in TFC: Skill InstructionsSae TumNo ratings yet
- Food Allergy and IntoleranceDocument5 pagesFood Allergy and IntoleranceSonja LekovicNo ratings yet
- Anaemia in PregnancyDocument29 pagesAnaemia in PregnancySampritha P GNo ratings yet
- Clinical Manifestations and Diagnosis of HHT (Osler-Weber-Rendu Syndrome) - UpToDateDocument14 pagesClinical Manifestations and Diagnosis of HHT (Osler-Weber-Rendu Syndrome) - UpToDateArturoNo ratings yet
- Mongtu Ngo ResumeDocument1 pageMongtu Ngo ResumeKrissy NgoNo ratings yet
- Starland International School Senior High School Department 1st Semester Prelim Exams S.Y. 2021-2022 Physical Education 11Document2 pagesStarland International School Senior High School Department 1st Semester Prelim Exams S.Y. 2021-2022 Physical Education 11Ken PaiiNo ratings yet
- TumorsDocument11 pagesTumorscocoNo ratings yet
- ATI Respiratory PowerpointDocument90 pagesATI Respiratory PowerpointAnn KelseaNo ratings yet
- Hospitals of NepalDocument21 pagesHospitals of NepalSuresh DhunganaNo ratings yet
- Tensimeter - Erkameter EDocument8 pagesTensimeter - Erkameter EeryNo ratings yet
- PTH 732-Vestibular EvalDocument8 pagesPTH 732-Vestibular Evalapi-551496110No ratings yet
- Dermatology JournalDocument17 pagesDermatology JournalKoas PatoNo ratings yet
- 20.1. Treatment Planning. Retention of The Natural Dentition and The Replacement of Missing Teeth. Endodontics Colleagues For Excellence (A.A.E.)Document8 pages20.1. Treatment Planning. Retention of The Natural Dentition and The Replacement of Missing Teeth. Endodontics Colleagues For Excellence (A.A.E.)Ixaya ZisuyatraNo ratings yet
- Cardiology MnemonicDocument46 pagesCardiology MnemonicA.h.Murad100% (1)
- ch116 Part2Document102 pagesch116 Part2p'eng matchima h.No ratings yet
- IAPT Positive Practice Guide For Working With People Who Use Drugs and Alcohol NhsDocument7 pagesIAPT Positive Practice Guide For Working With People Who Use Drugs and Alcohol NhsBete FerreiraNo ratings yet
- Practices in Paediatric Gastrointestinal Endoscopy at Kenyatta National Hospital and Gertrudes Children's Hospital in Nairobi KenyaDocument11 pagesPractices in Paediatric Gastrointestinal Endoscopy at Kenyatta National Hospital and Gertrudes Children's Hospital in Nairobi Kenyafrankline nyabutoNo ratings yet
- AOSpine Thoracolumbar Classification System - PosterDocument1 pageAOSpine Thoracolumbar Classification System - PosterFernanda AhumadaNo ratings yet
- ImmunizationDocument12 pagesImmunizationpppammNo ratings yet
- Anemia - Pato ClinicaDocument2 pagesAnemia - Pato ClinicaJean Pierre Loli PinNo ratings yet
- Pharmacology NotesDocument6 pagesPharmacology NotesHarsh PawarNo ratings yet
- Biochemistry of Down SyndromDocument3 pagesBiochemistry of Down SyndromJosephine mbahNo ratings yet
- Table of Different ParasitesDocument6 pagesTable of Different ParasitesYowan05No ratings yet
- What Is The Digestive SystemDocument4 pagesWhat Is The Digestive SystemAngelica CorpuzNo ratings yet
- The Concept of DeliriumDocument5 pagesThe Concept of DeliriumHirofumi AboNo ratings yet
- Livro Robbins PathologyDocument18 pagesLivro Robbins Pathologyernestooliveira50% (2)
- AmantadineDocument1 pageAmantadinemahmoud mohamedNo ratings yet
- How Is The Neonatal Resuscitation Program Algorithm Structured?Document7 pagesHow Is The Neonatal Resuscitation Program Algorithm Structured?Czarina Mae Quinones TadeoNo ratings yet