You might also like
- Post Insertion Denture ProblemsDocument48 pagesPost Insertion Denture ProblemsAswitha GanapathyNo ratings yet
- Cluster IXDocument12 pagesCluster IXTJ OberioNo ratings yet
- ENDO Q&A Mosby PDFDocument7 pagesENDO Q&A Mosby PDFShikhaNo ratings yet
- 1 30Document3 pages1 30ay daNo ratings yet
- 2010 AnsDocument37 pages2010 AnsArjun NarangNo ratings yet
- Quiz Pharma and OrthoDocument5 pagesQuiz Pharma and OrthoMonaNo ratings yet
- Test 4 - Prosthetic Dentistry & Dental Materials (Student Copy)Document8 pagesTest 4 - Prosthetic Dentistry & Dental Materials (Student Copy)dr.jah9No ratings yet
- Post-Insertion Denture ProblemsDocument10 pagesPost-Insertion Denture ProblemsRahul MahajanNo ratings yet
- Ndebreleasedquestions 2019 1 PDFDocument383 pagesNdebreleasedquestions 2019 1 PDFManish JunejaNo ratings yet
- s3 Resto Commdent2Document50 pagess3 Resto Commdent2Tara Lingating100% (1)
- DHA 2014 Revision - OziDent (1) - Compressed PDFDocument297 pagesDHA 2014 Revision - OziDent (1) - Compressed PDFWaheed QuadriNo ratings yet
- Ideas Wts - Mds - Prostho Q&ADocument18 pagesIdeas Wts - Mds - Prostho Q&AMostafa Fayad100% (1)
- Partial Veneer Crowns: by Dr. M.B.Santos MaccayDocument17 pagesPartial Veneer Crowns: by Dr. M.B.Santos MaccayGENECA MAY G. RAPADA100% (1)
- CD Qa1Document5 pagesCD Qa1DontoNo ratings yet
- Englishwritten Released 2018 PDFDocument401 pagesEnglishwritten Released 2018 PDFbobobo96No ratings yet
- Prostho MCQ Www-Matterhere-Com NRRDocument10 pagesProstho MCQ Www-Matterhere-Com NRRYoung FlameNo ratings yet
- Cluster III: Restorative Dentistry and Community DentistryDocument11 pagesCluster III: Restorative Dentistry and Community DentistryTJ Oberio100% (1)
- Darby: Mosby's Comprehensive Review of Dental Hygiene, 7 EditionDocument10 pagesDarby: Mosby's Comprehensive Review of Dental Hygiene, 7 EditiontoancaoNo ratings yet
- Chapter 5Document3 pagesChapter 5DANA ISABELLE PILAPILNo ratings yet
- MCQs in Chapter 1 of Contemporary OrthodonticsDocument12 pagesMCQs in Chapter 1 of Contemporary OrthodonticsDr.Fadi76% (34)
- 1 eNDODONTICS To PrintDocument19 pages1 eNDODONTICS To PrintDENTAL REVIEWER ONLYNo ratings yet
- Mid-2022 (Answers)Document6 pagesMid-2022 (Answers)نور كاضمNo ratings yet
- 2nd ExamDocument12 pages2nd Examيارا حسين100% (1)
- Paper 1Document29 pagesPaper 1Andrii DyvnychNo ratings yet
- MCQ c2 Spring1 2013Document3 pagesMCQ c2 Spring1 2013Hassan TantawyNo ratings yet
- Oral Anatomy and Physiology (Review Center)Document13 pagesOral Anatomy and Physiology (Review Center)yellow rangerNo ratings yet
- Endo Set 3 QuestionsDocument3 pagesEndo Set 3 QuestionsBinayak Upadhyaya100% (1)
- Rudman 2 ProsthodonticsDocument36 pagesRudman 2 Prosthodonticscath.rada17No ratings yet
- Problems, Diagnosis & Management in Complete Denture ProsthesisDocument106 pagesProblems, Diagnosis & Management in Complete Denture ProsthesisDrrksundar KumarNo ratings yet
- 6 Released - 2015 - EnglishDocument459 pages6 Released - 2015 - Englishuncia123No ratings yet
- Denture Trouble Shooting GuideDocument5 pagesDenture Trouble Shooting Guideheri asriyadiNo ratings yet
- Tissue Response To Complete DentureDocument7 pagesTissue Response To Complete DentureEVA MONSERRATNo ratings yet
- Endodontics (Review Center)Document10 pagesEndodontics (Review Center)LangNo ratings yet
- ADC 2001 Prilims Part 2Document22 pagesADC 2001 Prilims Part 2Saj198567% (3)
- ComplaintDocument52 pagesComplaintmarwaNo ratings yet
- Ortho ReviewersDocument6 pagesOrtho ReviewersdanebuentipoNo ratings yet
- Answendo PerioDocument5 pagesAnswendo Periof9fhzxszqcNo ratings yet
- Post Insertion Problems in Complete Denture: A Review: IP Annals of Prosthodontics and Restorative DentistryDocument5 pagesPost Insertion Problems in Complete Denture: A Review: IP Annals of Prosthodontics and Restorative DentistrySharon LawNo ratings yet
- DeepbiteDocument15 pagesDeepbiteagdroubiNo ratings yet
- HPSC Dental Surgeon Model Question PaperDocument10 pagesHPSC Dental Surgeon Model Question PapergauravkokraNo ratings yet
- Reviewer Cwe 2 2Document15 pagesReviewer Cwe 2 2Joane DirectoNo ratings yet
- Operative DentistryDocument6 pagesOperative DentistryLangNo ratings yet
- AHEAD Test and Discussions - COMPLETE DENTUREDocument16 pagesAHEAD Test and Discussions - COMPLETE DENTUREMostafa Fayad100% (1)
- Pediatric Dent & Orthodontics (Review Center)Document9 pagesPediatric Dent & Orthodontics (Review Center)yellow rangerNo ratings yet
- Group 3 Oral-Radiology-Assignment1Document16 pagesGroup 3 Oral-Radiology-Assignment1Nur IbrahimNo ratings yet
- MaloklusiiDocument6 pagesMaloklusiicahayaNo ratings yet
- University of The East College of Dentistry Orthodontics PDFDocument40 pagesUniversity of The East College of Dentistry Orthodontics PDFPatchNo ratings yet
- Ped Exam MacqsDocument99 pagesPed Exam MacqsIvailo FartalevNo ratings yet
- 2 OS To PrintDocument12 pages2 OS To PrintDENTAL REVIEWER ONLY0% (1)
- Post Insertion Problems For Complete Denture and Their ManagementDocument8 pagesPost Insertion Problems For Complete Denture and Their ManagementTaha AlaamryNo ratings yet
- T - D - Anatomy - (Day - 1) Questions PDFDocument9 pagesT - D - Anatomy - (Day - 1) Questions PDFRizzz AhmNo ratings yet
- Compre Ortho PedoDocument11 pagesCompre Ortho PedoPatricia L.No ratings yet
- 2014 Revision Questions - OziDent PDFDocument297 pages2014 Revision Questions - OziDent PDFMohsen Saeed OzaibiNo ratings yet
- TEST 7 - Orthodontics & Pedodontics (STUDENT COPY)Document6 pagesTEST 7 - Orthodontics & Pedodontics (STUDENT COPY)dr.jah9No ratings yet
- 4 5997026495686510171 220613 040632Document11 pages4 5997026495686510171 220613 040632Zaynab EidNo ratings yet
- Interceptive Orthodontics: A Practical Guide to Occlusal ManagementFrom EverandInterceptive Orthodontics: A Practical Guide to Occlusal ManagementNo ratings yet
- Oral Medicine & Pathology from A-ZFrom EverandOral Medicine & Pathology from A-ZRating: 5 out of 5 stars5/5 (9)
- Crown Lengthening Vs Forced EruptionDocument4 pagesCrown Lengthening Vs Forced EruptionbarbieNo ratings yet
- 6.rpa Clasp DesignDocument3 pages6.rpa Clasp DesignbarbieNo ratings yet
- V. B.A.,D.D.S. : Complete DenturesDocument10 pagesV. B.A.,D.D.S. : Complete DenturesbarbieNo ratings yet
- 2 Registration Stage 2Document6 pages2 Registration Stage 2barbieNo ratings yet
- Selection of Artificial TeethDocument11 pagesSelection of Artificial TeethbarbieNo ratings yet
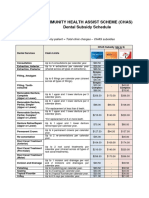
- CHAS Dental Subsidy ScheduleDocument1 pageCHAS Dental Subsidy ScheduleEugeneNo ratings yet
- Complete Dentures: Frederick S. Meyer, Minneapolis, MinnDocument13 pagesComplete Dentures: Frederick S. Meyer, Minneapolis, MinnMansoor Ahmed KhanNo ratings yet
- Telescopic Crowns As Attachments For Implant Supported Restorations A Case SeriesDocument9 pagesTelescopic Crowns As Attachments For Implant Supported Restorations A Case SeriesmaxNo ratings yet
- Impression Technique PDFDocument4 pagesImpression Technique PDFPremshith Cp100% (1)
- A Review: Flexible Removable Partial Dentures: Dr. Atulya Sharma, Dr. Shashidhara H.SDocument5 pagesA Review: Flexible Removable Partial Dentures: Dr. Atulya Sharma, Dr. Shashidhara H.SAnisa DyahNo ratings yet
- Color Stability, Water Sorption and Cytotoxicity Jap-7-278Document10 pagesColor Stability, Water Sorption and Cytotoxicity Jap-7-278drgunNo ratings yet
- CHAPTER 13 - Preparation of The Mouth For R - 2011 - McCracken S Removable Parti PDFDocument20 pagesCHAPTER 13 - Preparation of The Mouth For R - 2011 - McCracken S Removable Parti PDFFlorin Razvan CurcăNo ratings yet
- Ijphrd Jan-March 2012Document200 pagesIjphrd Jan-March 2012dockedarNo ratings yet
- Association of Neutral Zone Position With Age, Gender, and Period of EdentulismDocument9 pagesAssociation of Neutral Zone Position With Age, Gender, and Period of EdentulismNetra TaleleNo ratings yet
- FACE BOW / Orthodontic Courses by Indian Dental AcademyDocument24 pagesFACE BOW / Orthodontic Courses by Indian Dental Academyindian dental academyNo ratings yet
- Abnormal Involuntary Movement Scale (AIMS) - Overview: Clinical UtilityDocument3 pagesAbnormal Involuntary Movement Scale (AIMS) - Overview: Clinical UtilityBTNo ratings yet
- 1 Partially Edentulous Epidemiology Physiology and Terminology 1Document6 pages1 Partially Edentulous Epidemiology Physiology and Terminology 1Alexandra CastilloNo ratings yet
- Final C2 Spring 2o17 2Document11 pagesFinal C2 Spring 2o17 2Hassan TantawyNo ratings yet
- What Makes It Beautiful VitaDocument8 pagesWhat Makes It Beautiful VitaVladimir DrăgoiNo ratings yet
- Accurate Location of Postpalatal Seal Area On The Maxillary Complete Denture CastDocument2 pagesAccurate Location of Postpalatal Seal Area On The Maxillary Complete Denture CastCentro de Rehabilitacion Oral DEENTNo ratings yet
- Immediate Denture Fabrication: A Clinical Report: January 2013Document6 pagesImmediate Denture Fabrication: A Clinical Report: January 2013kapilqqqNo ratings yet
- Use of Polyvinyl Siloxane Material For An Altered Cast Impression Tray PDFDocument2 pagesUse of Polyvinyl Siloxane Material For An Altered Cast Impression Tray PDFNguyen Thi Minh HienNo ratings yet
- GlossectomyDocument68 pagesGlossectomyRohan GroverNo ratings yet
- Border MouldingDocument13 pagesBorder MouldingSwati Pathak GiriNo ratings yet
- Fabrication of Complete/partial Dentures (Different Final Impression Techniques and Materials) For Treating Edentulous Patients (Protocol)Document18 pagesFabrication of Complete/partial Dentures (Different Final Impression Techniques and Materials) For Treating Edentulous Patients (Protocol)Padmini ReddyNo ratings yet
- Posterior Palatal SealDocument55 pagesPosterior Palatal SealEazhil RajNo ratings yet
- CD Bernard LevinDocument172 pagesCD Bernard LevinIndrani Das50% (2)
- Lingualized Occlusion Dental Lab International PDFDocument3 pagesLingualized Occlusion Dental Lab International PDFArun PrasadNo ratings yet
- Vestibuloplasty: Related TermsDocument29 pagesVestibuloplasty: Related Termsمظفر منعم ميران عباسNo ratings yet
- Dimensions of The DentureDocument8 pagesDimensions of The DentureetequetaquiNo ratings yet
- Overdenture Abutment Under Fix Partial Denture PDFDocument4 pagesOverdenture Abutment Under Fix Partial Denture PDFDeasireeNo ratings yet
- ART4Document6 pagesART4Madalina MihailaNo ratings yet
- 1907-Article Text-6791-1-10-20190925Document4 pages1907-Article Text-6791-1-10-20190925shuhaib latifNo ratings yet
- Maxillary Occlusal RimDocument19 pagesMaxillary Occlusal Rimvarsha ammu0% (1)
- RPD STL PDFDocument7 pagesRPD STL PDFJohnnyDEro100% (2)