You might also like
- Fast Facts: Treatment-Free Remission in Chronic Myeloid Leukemia: From concept to practice and beyondFrom EverandFast Facts: Treatment-Free Remission in Chronic Myeloid Leukemia: From concept to practice and beyondNo ratings yet
- Nakayama, 2006Document22 pagesNakayama, 2006Giulia AndreeaNo ratings yet
- DHA Stop Cellular ProliferationDocument7 pagesDHA Stop Cellular ProliferationHamza SaidiNo ratings yet
- Tannic Acid Attenuates Vascular Calcification Induced PR - 2021 - Biomedicine PDFDocument12 pagesTannic Acid Attenuates Vascular Calcification Induced PR - 2021 - Biomedicine PDFFernando MaffeisNo ratings yet
- J Exp Med-1993-Woodrow-1517-22Document6 pagesJ Exp Med-1993-Woodrow-1517-22Omar Sánchez AntonioNo ratings yet
- Int. Immunol.-1999-Staal-317-23Document7 pagesInt. Immunol.-1999-Staal-317-23Karthik AripakaNo ratings yet
- T Cell Activation and Signaling: TCR TalinDocument8 pagesT Cell Activation and Signaling: TCR TalinMst Monira KhatonNo ratings yet
- TRPC 6 As A Molecular Target in Diabetic NephropathyDocument4 pagesTRPC 6 As A Molecular Target in Diabetic NephropathySSR-IIJLS JournalNo ratings yet
- Tissue Plasminogen Activator Neurovascular Toxicity Is Controlled by Activated Protein CDocument5 pagesTissue Plasminogen Activator Neurovascular Toxicity Is Controlled by Activated Protein CAmit JoshiNo ratings yet
- s41598 020 73667 ZDocument13 pagess41598 020 73667 ZCarolina RicárdezNo ratings yet
- NHE3 ZIjian XieDocument9 pagesNHE3 ZIjian Xienilberto2No ratings yet
- Hilgemann 1996Document4 pagesHilgemann 1996Giulia AndreeaNo ratings yet
- Pic RenderDocument9 pagesPic Renderkora_c995No ratings yet
- Novel Strategy For Measuring Creatine Kinase Reaction Rate in The in Vivo HeartDocument10 pagesNovel Strategy For Measuring Creatine Kinase Reaction Rate in The in Vivo HeartYoung-Hoon SungNo ratings yet
- Hypertonic Stress Regulates T Cell Function Via Pannexin-1 Hemichannels and P2X ReceptorsDocument9 pagesHypertonic Stress Regulates T Cell Function Via Pannexin-1 Hemichannels and P2X ReceptorsjavillusNo ratings yet
- Ca 1.3 and BK Channels For Timing and Regulating Cell FiringDocument14 pagesCa 1.3 and BK Channels For Timing and Regulating Cell FiringGabriel L. DebastianiNo ratings yet
- Targeting Calcium Signaling in Cancer TherapyDocument15 pagesTargeting Calcium Signaling in Cancer TherapyLeonel LedezmaNo ratings yet
- TRP Channels in Neuronal and Glial Signal Transduction: Christian Harteneck and Kristina LeunerDocument22 pagesTRP Channels in Neuronal and Glial Signal Transduction: Christian Harteneck and Kristina Leunerkj185No ratings yet
- Phosphorylation of P-Glycoprotein by PKA and PKC Modulates Swelling-Activated CL CurrentsDocument9 pagesPhosphorylation of P-Glycoprotein by PKA and PKC Modulates Swelling-Activated CL CurrentsDr-Dalya ShakirNo ratings yet
- Embo Embo Embo: C-Secretase ActivityDocument11 pagesEmbo Embo Embo: C-Secretase ActivityMaria Vonny WijayaNo ratings yet
- Cas PaseDocument34 pagesCas PaseRafael Dall'AlbaNo ratings yet
- Release 2+ and Independently of Sarcoplasmic Reticulum Ca Mediated TRPC3 Channel Activation Receptor 3 Constricts Cerebral Arteries Via IP 3 IPDocument18 pagesRelease 2+ and Independently of Sarcoplasmic Reticulum Ca Mediated TRPC3 Channel Activation Receptor 3 Constricts Cerebral Arteries Via IP 3 IPicanadaaNo ratings yet
- Zisowsky 2007Document10 pagesZisowsky 2007Marco BrithoNo ratings yet
- Nat Immunol 2014navarroDocument8 pagesNat Immunol 2014navarrotri sutrianiNo ratings yet
- NIH Public Access: Author ManuscriptDocument29 pagesNIH Public Access: Author ManuscriptVenkata Raghuram GorantlaNo ratings yet
- Kollarik 2004Document9 pagesKollarik 2004Mariana ThielNo ratings yet
- Jvms 83 997Document7 pagesJvms 83 997Blanca A SerranoNo ratings yet
- BF02462837Document4 pagesBF02462837ttqnhu.rhmNo ratings yet
- Kondo 2000, Putative Ryanodine Receptors in The Sarcolemma of Ventricular Myocytes.Document7 pagesKondo 2000, Putative Ryanodine Receptors in The Sarcolemma of Ventricular Myocytes.Alessio LissoniNo ratings yet
- A Dual Thrombin Receptor System For Platelet Activation: Nature September 1998Document6 pagesA Dual Thrombin Receptor System For Platelet Activation: Nature September 1998Kamonashis Sarkar TendulNo ratings yet
- Hpertensi Dan GGKDocument33 pagesHpertensi Dan GGKJemz AlbertNo ratings yet
- Stores in MPTP OpeningDocument20 pagesStores in MPTP OpeningCarolina RicárdezNo ratings yet
- Fauconnier2007 Insulin TRPC3Document10 pagesFauconnier2007 Insulin TRPC3Giulia AndreeaNo ratings yet
- The Role of The NaDocument13 pagesThe Role of The NamrtiborhornyikNo ratings yet
- Cardiotonic Steroids Differentially Affect Intracellular Na and (Na) / (K) - Independent Signaling in C7-MDCK CellsDocument8 pagesCardiotonic Steroids Differentially Affect Intracellular Na and (Na) / (K) - Independent Signaling in C7-MDCK CellsHugo MartínezNo ratings yet
- Cloning and Expression of A cDNA Encoding The Transporter of Taurine and /8-Alanine in Mouse BrainDocument5 pagesCloning and Expression of A cDNA Encoding The Transporter of Taurine and /8-Alanine in Mouse BrainJana NgNo ratings yet
- NROSCI 1012 - Lecture 24Document4 pagesNROSCI 1012 - Lecture 24HonzaNo ratings yet
- UntitledDocument7 pagesUntitledTuấn Nguyen AnhNo ratings yet
- 1999 - Mechanisms of Altered Excitation-Contraction Coupling in Canine Tachycardia-Induced Heart Failure, IDocument9 pages1999 - Mechanisms of Altered Excitation-Contraction Coupling in Canine Tachycardia-Induced Heart Failure, IBeto RamirezNo ratings yet
- PIIS0021925820650190Document9 pagesPIIS0021925820650190thehardbait12No ratings yet
- Transferrin: Cdna Chromosomal Localization : Human Characterization andDocument5 pagesTransferrin: Cdna Chromosomal Localization : Human Characterization andAndrimencitNo ratings yet
- FTPDocument7 pagesFTPAlema PelesićNo ratings yet
- Volk 2003, A Polycystin-2-Like Large Conductance Cation Channel in Rat LeftDocument13 pagesVolk 2003, A Polycystin-2-Like Large Conductance Cation Channel in Rat LeftAlessio LissoniNo ratings yet
- Jurnal 55Document1 pageJurnal 55rizalmantaNo ratings yet
- Electrophysiology and Electro Physio Pharmacology of Cardiac Cells - Docclass 2 Electrophysiology and Electro Physio Pharmacology of Cardiac CellsDocument71 pagesElectrophysiology and Electro Physio Pharmacology of Cardiac Cells - Docclass 2 Electrophysiology and Electro Physio Pharmacology of Cardiac CellsdcicareNo ratings yet
- Inhibition of The K Channel Kca3.1 Ameliorates T Cell-Mediated ColitisDocument9 pagesInhibition of The K Channel Kca3.1 Ameliorates T Cell-Mediated ColitisKatie RufoNo ratings yet
- Pi Is 0022282817303115Document11 pagesPi Is 0022282817303115EdgarNo ratings yet
- KJPP 23 345Document12 pagesKJPP 23 345Aldin Mendoza AguilarNo ratings yet
- Notes On MusclesDocument6 pagesNotes On MusclesJohn PagnuNo ratings yet
- Meissner 2008Document13 pagesMeissner 2008Farhana AnuarNo ratings yet
- Taniguchi 1983Document10 pagesTaniguchi 1983Giulia AndreeaNo ratings yet
- Good PaperDocument12 pagesGood Paperlkanth1No ratings yet
- Effects of PMCA and SERCA Pump Over Expression On The Kinetics of Cell CA+2 SignallingDocument10 pagesEffects of PMCA and SERCA Pump Over Expression On The Kinetics of Cell CA+2 SignallingjanethkeNo ratings yet
- Nucleotide JorgeDocument5 pagesNucleotide JorgeMonique SamaanNo ratings yet
- Animal Toxins and Renal Ion Transport: Another Dimension in Tropical NephrologyDocument8 pagesAnimal Toxins and Renal Ion Transport: Another Dimension in Tropical NephrologyMiguel SierraNo ratings yet
- 2014 KhatamiDocument6 pages2014 Khatamiporfyra_No ratings yet
- TPTP PDFDocument8 pagesTPTP PDFCarolina RicárdezNo ratings yet
- 1 s2.0 S002075190800180X MainDocument10 pages1 s2.0 S002075190800180X Mainyujiao MaNo ratings yet
- Research Paper NS11021, A Novel Opener of Large-Conductance Ca - Activated K Channels, Enhances Erectile Responses in RatsDocument12 pagesResearch Paper NS11021, A Novel Opener of Large-Conductance Ca - Activated K Channels, Enhances Erectile Responses in RatsCarlos LabradaNo ratings yet
- tPA and NMDA Receptor PDFDocument9 pagestPA and NMDA Receptor PDFsaurabh mahajanNo ratings yet
- Nihms 181336Document6 pagesNihms 181336Giulia AndreeaNo ratings yet
- Mehta 2011Document10 pagesMehta 2011Giulia AndreeaNo ratings yet
- Nattel&Carlsson2006 Antiarrhythmic Drugs TaseDocument16 pagesNattel&Carlsson2006 Antiarrhythmic Drugs TaseGiulia AndreeaNo ratings yet
- Yong Y 2009Document6 pagesYong Y 2009Giulia AndreeaNo ratings yet
- Fujiwara Et Al., 2011Document6 pagesFujiwara Et Al., 2011Giulia AndreeaNo ratings yet
- GB 2003 4 3 207Document7 pagesGB 2003 4 3 207Giulia AndreeaNo ratings yet
- Jphysiol01394 0087Document28 pagesJphysiol01394 0087Giulia AndreeaNo ratings yet
- The Structure of Ion Channels in Membranes of Excitable Cells ReviewDocument12 pagesThe Structure of Ion Channels in Membranes of Excitable Cells ReviewGiulia AndreeaNo ratings yet
- Maen Sarhan, 2009Document10 pagesMaen Sarhan, 2009Giulia AndreeaNo ratings yet
- Hilgemann 1996Document4 pagesHilgemann 1996Giulia AndreeaNo ratings yet
- Hermann, 2011Document9 pagesHermann, 2011Giulia AndreeaNo ratings yet
- Biochemical and Biophysical Research CommunicationsDocument7 pagesBiochemical and Biophysical Research CommunicationsGiulia AndreeaNo ratings yet
- Molecular Physiology of Low-Voltage-Activated T-Type Calcium ChannelsDocument45 pagesMolecular Physiology of Low-Voltage-Activated T-Type Calcium ChannelsGiulia AndreeaNo ratings yet
- Wang2007 Alpha2 Adrenergic HCN Prefrontal CortexDocument14 pagesWang2007 Alpha2 Adrenergic HCN Prefrontal CortexGiulia AndreeaNo ratings yet
- Molecular Mechanism of cAMP Modulation of HCN Pacemaker ChannelsDocument6 pagesMolecular Mechanism of cAMP Modulation of HCN Pacemaker ChannelsGiulia AndreeaNo ratings yet
- Taniguchi 1983Document10 pagesTaniguchi 1983Giulia AndreeaNo ratings yet
- Mashour2018-Correlates of ConsciousnessDocument3 pagesMashour2018-Correlates of ConsciousnessGiulia AndreeaNo ratings yet
- Print Brain Imaging Technique Identifies Previously Undetected Epileptic Seizure Sites - BiocompareDocument2 pagesPrint Brain Imaging Technique Identifies Previously Undetected Epileptic Seizure Sites - BiocompareGiulia AndreeaNo ratings yet
- Science 2015 Huang 42 4Document4 pagesScience 2015 Huang 42 4Giulia AndreeaNo ratings yet
- Multimodal Confocal MicrosDocument10 pagesMultimodal Confocal MicrosGiulia AndreeaNo ratings yet
- Lipinski - 2007 - Journal of The American College of CardiologyDocument7 pagesLipinski - 2007 - Journal of The American College of CardiologyGiulia AndreeaNo ratings yet
- Fauconnier2007 Insulin TRPC3Document10 pagesFauconnier2007 Insulin TRPC3Giulia AndreeaNo ratings yet
- Frischauf2008 STIM Orai CouplingDocument8 pagesFrischauf2008 STIM Orai CouplingGiulia AndreeaNo ratings yet
- Composing Life: ReportsDocument6 pagesComposing Life: ReportsGiulia AndreeaNo ratings yet
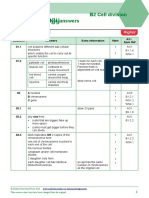
- B2 Cell Division Exam Style AnswersDocument2 pagesB2 Cell Division Exam Style Answersjimmy100% (4)
- Asexual and Sexual Reproduction 2016Document14 pagesAsexual and Sexual Reproduction 2016PikaNo ratings yet
- Platinum Taq DNA PolymeraseDocument2 pagesPlatinum Taq DNA PolymeraseAndré OliveiraNo ratings yet
- Nutritional Classification of BacteriaDocument7 pagesNutritional Classification of BacteriaRalphpinno SanchezNo ratings yet
- COPII-mediated Vesicle Formation at A GlanceDocument4 pagesCOPII-mediated Vesicle Formation at A GlanceMădălina MarincaşNo ratings yet
- VivaDiag SARS-CoV-2 Ag Rapid Test Brochure (En) PDFDocument1 pageVivaDiag SARS-CoV-2 Ag Rapid Test Brochure (En) PDFBPG ServiceNo ratings yet
- Unit Respiration: Ow EverDocument23 pagesUnit Respiration: Ow EverAbhishek KumarNo ratings yet
- Sbstta 18 Inf 03 enDocument63 pagesSbstta 18 Inf 03 enPasta LoverNo ratings yet
- JURNAL Tingkal IndonesiaDocument14 pagesJURNAL Tingkal IndonesiaIwilja Nanda RissaNo ratings yet
- GLYCOLYSISDocument6 pagesGLYCOLYSISHAZEL SANDRONo ratings yet
- VMP 930 Veterinary Parasitology: PlatyhelminthesDocument81 pagesVMP 930 Veterinary Parasitology: PlatyhelminthesRenien Khim BahayaNo ratings yet
- Descriptors For FIGS Ficus CaricaDocument63 pagesDescriptors For FIGS Ficus CaricaHanafizar Hanafi Napi AtanNo ratings yet
- Bayombong Nueva Vizcaya: Saint Mary's UniversityDocument5 pagesBayombong Nueva Vizcaya: Saint Mary's UniversityThempty WrayterNo ratings yet
- Microbiology and ParasitologyDocument14 pagesMicrobiology and ParasitologyTyRa cHiAnE A. LaPeRa86% (43)
- Exercício Físico, Densidade Mineral Óssea e OsteoporoseDocument87 pagesExercício Físico, Densidade Mineral Óssea e OsteoporoseThomasKauamNo ratings yet
- Ch. 22 Origin of Species S18Document24 pagesCh. 22 Origin of Species S18Elyzabeth BeauchampNo ratings yet
- Bio 175 Lab Test I Study GuideDocument2 pagesBio 175 Lab Test I Study GuideMarco CalvaraNo ratings yet
- HowTo Finding SNP by BLASTDocument4 pagesHowTo Finding SNP by BLASTIsabel Luiza LimaNo ratings yet
- Notes On Mutect2: Broad Institute, 415 Main Street, Cambridge, MA 02142Document14 pagesNotes On Mutect2: Broad Institute, 415 Main Street, Cambridge, MA 02142Min JiaNo ratings yet
- Homework 1Document1 pageHomework 1evdm evdmNo ratings yet
- Different Advancement in Science and Technology: 1. Semiconductor ChipsDocument5 pagesDifferent Advancement in Science and Technology: 1. Semiconductor ChipsRegiena AnicieteNo ratings yet
- Sterilization By: Physical MethodsDocument36 pagesSterilization By: Physical MethodstashaNo ratings yet
- Cancer Immune TherapyDocument452 pagesCancer Immune TherapyatyNo ratings yet
- Grade 8 Budget of Work FinalDocument8 pagesGrade 8 Budget of Work FinalNar ZieNo ratings yet
- Part 1: Your First BLAST SearchDocument24 pagesPart 1: Your First BLAST SearchFernanda RodríguezNo ratings yet
- Questions-Biological Science DavaoDocument10 pagesQuestions-Biological Science DavaoMARY ANN TIONGSONNo ratings yet
- Cell DivisionDocument5 pagesCell DivisionSsonko EdrineNo ratings yet
- Bioc202 Problem SetsDocument14 pagesBioc202 Problem SetsSYZCNo ratings yet
- How It All Began My ArticleDocument6 pagesHow It All Began My ArticleDr Kadiyali M SrivatsaNo ratings yet
- BDDCS Predictions, Self-Correcting Aspects of BDDCS Assignments, BDDCS Assignment Corrections, and Classification For More Than 175 Additional DrugsDocument10 pagesBDDCS Predictions, Self-Correcting Aspects of BDDCS Assignments, BDDCS Assignment Corrections, and Classification For More Than 175 Additional DrugsBagoes AsNo ratings yet
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4.5 out of 5 stars4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Tales from Both Sides of the Brain: A Life in NeuroscienceFrom EverandTales from Both Sides of the Brain: A Life in NeuroscienceRating: 3 out of 5 stars3/5 (18)
- A Series of Fortunate Events: Chance and the Making of the Planet, Life, and YouFrom EverandA Series of Fortunate Events: Chance and the Making of the Planet, Life, and YouRating: 4.5 out of 5 stars4.5/5 (62)
- Who's in Charge?: Free Will and the Science of the BrainFrom EverandWho's in Charge?: Free Will and the Science of the BrainRating: 4 out of 5 stars4/5 (65)
- Undeniable: How Biology Confirms Our Intuition That Life Is DesignedFrom EverandUndeniable: How Biology Confirms Our Intuition That Life Is DesignedRating: 4 out of 5 stars4/5 (11)
- 10% Human: How Your Body's Microbes Hold the Key to Health and HappinessFrom Everand10% Human: How Your Body's Microbes Hold the Key to Health and HappinessRating: 4 out of 5 stars4/5 (33)
- Return of the God Hypothesis: Three Scientific Discoveries That Reveal the Mind Behind the UniverseFrom EverandReturn of the God Hypothesis: Three Scientific Discoveries That Reveal the Mind Behind the UniverseRating: 4.5 out of 5 stars4.5/5 (52)
- The Rise and Fall of the Dinosaurs: A New History of a Lost WorldFrom EverandThe Rise and Fall of the Dinosaurs: A New History of a Lost WorldRating: 4 out of 5 stars4/5 (598)
- The Dragons of Eden: Speculations on the Evolution of Human IntelligenceFrom EverandThe Dragons of Eden: Speculations on the Evolution of Human IntelligenceRating: 4 out of 5 stars4/5 (633)
- Seven and a Half Lessons About the BrainFrom EverandSeven and a Half Lessons About the BrainRating: 4 out of 5 stars4/5 (111)
- The Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionFrom EverandThe Ancestor's Tale: A Pilgrimage to the Dawn of EvolutionRating: 4 out of 5 stars4/5 (812)
- Buddha's Brain: The Practical Neuroscience of Happiness, Love & WisdomFrom EverandBuddha's Brain: The Practical Neuroscience of Happiness, Love & WisdomRating: 4 out of 5 stars4/5 (217)
- The Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceFrom EverandThe Molecule of More: How a Single Chemical in Your Brain Drives Love, Sex, and Creativity--and Will Determine the Fate of the Human RaceRating: 4.5 out of 5 stars4.5/5 (517)
- A Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsFrom EverandA Brief History of Intelligence: Evolution, AI, and the Five Breakthroughs That Made Our BrainsRating: 4.5 out of 5 stars4.5/5 (6)
- The Other Side of Normal: How Biology Is Providing the Clues to Unlock the Secrets of Normal and Abnormal BehaviorFrom EverandThe Other Side of Normal: How Biology Is Providing the Clues to Unlock the Secrets of Normal and Abnormal BehaviorNo ratings yet
- Good Without God: What a Billion Nonreligious People Do BelieveFrom EverandGood Without God: What a Billion Nonreligious People Do BelieveRating: 4 out of 5 stars4/5 (66)
- Minds Make Societies: How Cognition Explains the World Humans CreateFrom EverandMinds Make Societies: How Cognition Explains the World Humans CreateRating: 4.5 out of 5 stars4.5/5 (24)
- Human: The Science Behind What Makes Your Brain UniqueFrom EverandHuman: The Science Behind What Makes Your Brain UniqueRating: 3.5 out of 5 stars3.5/5 (38)
- Why We Sleep: Unlocking the Power of Sleep and DreamsFrom EverandWhy We Sleep: Unlocking the Power of Sleep and DreamsRating: 4.5 out of 5 stars4.5/5 (2083)
- The Lives of Bees: The Untold Story of the Honey Bee in the WildFrom EverandThe Lives of Bees: The Untold Story of the Honey Bee in the WildRating: 4.5 out of 5 stars4.5/5 (44)
- Lymph & Longevity: The Untapped Secret to HealthFrom EverandLymph & Longevity: The Untapped Secret to HealthRating: 4.5 out of 5 stars4.5/5 (13)
- The Invention of Tomorrow: A Natural History of ForesightFrom EverandThe Invention of Tomorrow: A Natural History of ForesightRating: 4.5 out of 5 stars4.5/5 (5)
- Remnants of Ancient Life: The New Science of Old FossilsFrom EverandRemnants of Ancient Life: The New Science of Old FossilsRating: 3 out of 5 stars3/5 (3)
- Crypt: Life, Death and Disease in the Middle Ages and BeyondFrom EverandCrypt: Life, Death and Disease in the Middle Ages and BeyondRating: 4 out of 5 stars4/5 (4)