You might also like
- 15-Foundation of TowerDocument57 pages15-Foundation of Towerhari1008108100% (2)
- Pulley Support AssemblyDocument3 pagesPulley Support Assemblyquanckb67% (3)
- Schneider 2001Document9 pagesSchneider 2001gbgzeraNo ratings yet
- Total Knee Arthroplasty: Aspects On Improved Fixation in The Younger PatientDocument77 pagesTotal Knee Arthroplasty: Aspects On Improved Fixation in The Younger PatientAndreea TudorascuNo ratings yet
- Measurement of Bone Defects Adjacent To Acetabular Components of Hip ReplacementDocument9 pagesMeasurement of Bone Defects Adjacent To Acetabular Components of Hip Replacementehabede6445No ratings yet
- Jfasap 8 201Document5 pagesJfasap 8 201vandhani79No ratings yet
- Comparison of Stainless Steel and Titanium Alloy Orthodontic Miniscrew Implants - A Mechanical and Histologic AnalysisDocument9 pagesComparison of Stainless Steel and Titanium Alloy Orthodontic Miniscrew Implants - A Mechanical and Histologic AnalysisDiego Andres Hincapie HerreraNo ratings yet
- Increase of Pullout Strength of Spinal Pedicle Screws With Conical Core: Biomechanical Tests and Finite Element AnalysesDocument7 pagesIncrease of Pullout Strength of Spinal Pedicle Screws With Conical Core: Biomechanical Tests and Finite Element AnalysesJavier Antonio Cardenas OliverosNo ratings yet
- CJV 017Document9 pagesCJV 017malifaragNo ratings yet
- Reduced Articular Surface of One-Piece Cups: A Cause of Runaway Wear and Early FailureDocument5 pagesReduced Articular Surface of One-Piece Cups: A Cause of Runaway Wear and Early FailureDarren LongNo ratings yet
- Osseointegration and Defect Repair With A New Porous Titanium Screw in Ovine Long-Bone Models For Gap-Healing, Osteonecrosis, and Bone IngrowthDocument1 pageOsseointegration and Defect Repair With A New Porous Titanium Screw in Ovine Long-Bone Models For Gap-Healing, Osteonecrosis, and Bone IngrowthMehmet TopuzNo ratings yet
- Suchenski 1992Document6 pagesSuchenski 1992piyush joshiNo ratings yet
- Bun PIIS174391911400973XDocument5 pagesBun PIIS174391911400973XNorin FornaNo ratings yet
- Degernes Et Al 1998 Holding Power of Different Pin Designs and Pin Insertion Methods in AviaDocument6 pagesDegernes Et Al 1998 Holding Power of Different Pin Designs and Pin Insertion Methods in AviaWalter Ezequiel CondoriNo ratings yet
- Alveolar Bone Response To Light-Force Tipping and Bodily Movement in Maxillary Incisor Advancement: A Prospective Randomized Clinical TrialDocument9 pagesAlveolar Bone Response To Light-Force Tipping and Bodily Movement in Maxillary Incisor Advancement: A Prospective Randomized Clinical TrialFelipeArroyoBonillaNo ratings yet
- FulltextDocument10 pagesFulltextDenis AlexandruNo ratings yet
- Pi Is 0889540607001448Document1 pagePi Is 0889540607001448djosephjohn89No ratings yet
- (2009) Garbuz - Metal On Metal Hip Resyrfacing X Large Diameter Head Metal Metal Total Hip ArthroplastyDocument9 pages(2009) Garbuz - Metal On Metal Hip Resyrfacing X Large Diameter Head Metal Metal Total Hip ArthroplastySandro Luiz Machado CarvalhoNo ratings yet
- Comparison of Stability of Titanium and Absorbable Plate and Screw Fixation For Mandibular Angle FracturesDocument6 pagesComparison of Stability of Titanium and Absorbable Plate and Screw Fixation For Mandibular Angle FracturesklimasNo ratings yet
- Comparison of Strength and Failure Mode of Seven Implant Systems: An in Vitro TestDocument10 pagesComparison of Strength and Failure Mode of Seven Implant Systems: An in Vitro TestDr FarhatNo ratings yet
- Weiler 1998Document9 pagesWeiler 1998piyush joshiNo ratings yet
- English AJODO 2004Document3 pagesEnglish AJODO 2004Diego Andres Hincapie HerreraNo ratings yet
- Ijirstv2i4040 PDFDocument3 pagesIjirstv2i4040 PDFTejas krishnakanthNo ratings yet
- Bone Stress When Miniplates Are Used For OrthodontDocument7 pagesBone Stress When Miniplates Are Used For OrthodontNicolasFernandezNo ratings yet
- Li 2011Document11 pagesLi 2011Hurāirāh ĐāřNo ratings yet
- On Healing of Titanium Implants in Iliac Crest BonDocument77 pagesOn Healing of Titanium Implants in Iliac Crest BonHelena KalmatNo ratings yet
- Strength-Durability Correlation of OsteosynthesisDocument17 pagesStrength-Durability Correlation of OsteosynthesisdeniNo ratings yet
- 2015 - Biomechanical Evaluation of Different Angle-Stable Locking Plating Systems For Mandibular SurgeryDocument30 pages2015 - Biomechanical Evaluation of Different Angle-Stable Locking Plating Systems For Mandibular SurgeryLeandro Nascimento Rodrigues dos santosNo ratings yet
- Mechanical CharacteristicDocument7 pagesMechanical CharacteristicJuankNo ratings yet
- Hydroxyapatite Ceramic Coating For Bone Implant FixationDocument60 pagesHydroxyapatite Ceramic Coating For Bone Implant FixationCerita KitaNo ratings yet
- CatalogoDocument7 pagesCatalogoIsabela Campos SánchezNo ratings yet
- Australian Football Players' Achilles Tendons Respond To Game Loads Within 2 Days: An Ultrasound Tissue Characterisation (UTC) StudyDocument8 pagesAustralian Football Players' Achilles Tendons Respond To Game Loads Within 2 Days: An Ultrasound Tissue Characterisation (UTC) StudyMarian DMNo ratings yet
- On Force and Tooth Movement PDFDocument14 pagesOn Force and Tooth Movement PDFSelvaNo ratings yet
- Biomechanical Evaluation of The Surgical Implant Generation Network (SIGN) Intramedullary Tibial NailDocument1 pageBiomechanical Evaluation of The Surgical Implant Generation Network (SIGN) Intramedullary Tibial NailTefera LeteboNo ratings yet
- Cuñas MetalicasDocument8 pagesCuñas MetalicasOciel AcostaNo ratings yet
- 784 2022 Article 4781Document11 pages784 2022 Article 4781Thibaut BossuytNo ratings yet
- Biomechanical Characteristics of Rib Fracture FixaDocument7 pagesBiomechanical Characteristics of Rib Fracture Fixaduke3443No ratings yet
- J Arth 2015 09 001Document7 pagesJ Arth 2015 09 001Carlos Mauricio Salazar BedollaNo ratings yet
- Three-Dimensional Finite Element Analysis of Extra Short Implants Focusing On Implant Designs and Materials. Int J Implant Dent, 2020Document10 pagesThree-Dimensional Finite Element Analysis of Extra Short Implants Focusing On Implant Designs and Materials. Int J Implant Dent, 2020Marlene Kasumi Gantier TakanoNo ratings yet
- Dissertation Retrospektive AnalyseDocument7 pagesDissertation Retrospektive AnalysePaperWritingServiceSuperiorpapersOmaha100% (1)
- Locking T-Plate Repair of Ilial Fractures in Cats and Small DogsDocument8 pagesLocking T-Plate Repair of Ilial Fractures in Cats and Small DogsNayra Cristina Herreira do ValleNo ratings yet
- (2008 Weng) Influence of Microgap Location and Configuration On The Periimplant Bone Morphology in Submerged Implants. An Experimental Study in DogsDocument7 pages(2008 Weng) Influence of Microgap Location and Configuration On The Periimplant Bone Morphology in Submerged Implants. An Experimental Study in Dogsyena1010No ratings yet
- A Finite Element and Experimental Investigation of The Femoral Component Mechanics in A Total Hip Arthroplasty - Cameron Gordon Bell - Thesis - 2005Document388 pagesA Finite Element and Experimental Investigation of The Femoral Component Mechanics in A Total Hip Arthroplasty - Cameron Gordon Bell - Thesis - 2005Henrique Rodrigues OliveiraNo ratings yet
- Jos 2 61Document6 pagesJos 2 61Bethiza CamposNo ratings yet
- Absorbible InglesDocument9 pagesAbsorbible InglesTamara PricilaNo ratings yet
- Total Knee Prosthesis - Final - Andaç - Anıl - ÇOBANDocument19 pagesTotal Knee Prosthesis - Final - Andaç - Anıl - ÇOBANAndaç ÇobanNo ratings yet
- Comparison of The Amount of Maxillary Canine RetraDocument6 pagesComparison of The Amount of Maxillary Canine RetrasmritiNo ratings yet
- Influência Das Forças Rotacionais Na Estabilidade Do Mini-Implante - ChoDocument6 pagesInfluência Das Forças Rotacionais Na Estabilidade Do Mini-Implante - ChoUrsula Pantigozo MoránNo ratings yet
- Tsumita 2013Document5 pagesTsumita 2013JesusCordobaNo ratings yet
- The Biomechanics of Lag Screw Insertion A ComparisDocument2 pagesThe Biomechanics of Lag Screw Insertion A ComparisCamilo Marin TovarNo ratings yet
- Cios 3 107Document7 pagesCios 3 107Ashish UpadhyayNo ratings yet
- 00-Age Variations in The Properties of Human Tibial Trabecular Bone and CartilageDocument48 pages00-Age Variations in The Properties of Human Tibial Trabecular Bone and CartilageYONATAN FABIAN TOVAR TOVARNo ratings yet
- Shear Strength CTI2001Document6 pagesShear Strength CTI2001Ieuan MorrisNo ratings yet
- Relations of Mechanical Properties To Density and CT Numbers in Human BoneDocument9 pagesRelations of Mechanical Properties To Density and CT Numbers in Human BoneNikola MijailovićNo ratings yet
- Hip Resurfacing Expectations and LimitationsDocument4 pagesHip Resurfacing Expectations and LimitationsCristian BenayNo ratings yet
- Araoye IB - Use of Intramedullary Carbon Fiber Nail in Hindfoot Fusion A SmallDocument6 pagesAraoye IB - Use of Intramedullary Carbon Fiber Nail in Hindfoot Fusion A SmallHariom ShuklaNo ratings yet
- Research and Education: Section EditorDocument12 pagesResearch and Education: Section EditorMayra Ortiz HerreraNo ratings yet
- Torque Efficiency of Different Archwires in 0.018-And 0.022-Inch Conventional BracketsDocument6 pagesTorque Efficiency of Different Archwires in 0.018-And 0.022-Inch Conventional BracketsCynthia AlfaroNo ratings yet
- Oseo 3Document4 pagesOseo 3mishel orlandoNo ratings yet
- Bone ReactionDocument9 pagesBone ReactionFourthMolar.comNo ratings yet
- Very Good To ReadDocument15 pagesVery Good To ReadGunall SNo ratings yet
- Short ImplantsFrom EverandShort ImplantsBoyd J. TomasettiNo ratings yet
- WorkshopDocument1 pageWorkshopNileshTipanNo ratings yet
- Remodelamiento Oseo de Las FracturasDocument5 pagesRemodelamiento Oseo de Las FracturasJulián Amaya MújicaNo ratings yet
- Chronology of Bioactive Glass Development and Clinical ApplicationsDocument7 pagesChronology of Bioactive Glass Development and Clinical ApplicationsNileshTipanNo ratings yet
- 4 NTDocument13 pages4 NTNileshTipanNo ratings yet
- Accepted ManuscriptDocument27 pagesAccepted ManuscriptNileshTipanNo ratings yet
- Metallography of Magnesium and Its Alloys: By: George Vander VoortDocument5 pagesMetallography of Magnesium and Its Alloys: By: George Vander VoortNileshTipanNo ratings yet
- WorkshopDocument1 pageWorkshopNileshTipanNo ratings yet
- Inflammation, Ageing, and Bone Regeneration: SciencedirectDocument8 pagesInflammation, Ageing, and Bone Regeneration: SciencedirectNileshTipanNo ratings yet
- JFB 08 00044Document15 pagesJFB 08 00044OoNo ratings yet
- Biomedical Applications of Biodegradable Polymers: Bret D. Ulery, Lakshmi S. Nair, Cato T. LaurencinDocument33 pagesBiomedical Applications of Biodegradable Polymers: Bret D. Ulery, Lakshmi S. Nair, Cato T. LaurencinSneha MadhuNo ratings yet
- Biodegradable Scaffold of Natural Polymer and Hydroxyapatite For Bone Tissue Engineering: A Short ReviewDocument6 pagesBiodegradable Scaffold of Natural Polymer and Hydroxyapatite For Bone Tissue Engineering: A Short ReviewNileshTipanNo ratings yet
- Biodegradable Polymers and Their Bone Applications: A ReviewDocument19 pagesBiodegradable Polymers and Their Bone Applications: A ReviewNileshTipanNo ratings yet
- Biodegradable Polymers and Their Bone Applications: A ReviewDocument19 pagesBiodegradable Polymers and Their Bone Applications: A ReviewNileshTipanNo ratings yet
- Strew and Stre H Re Ntion in of Absorbable, Self-Reinforced Polyglycolide (PGA) Rods For Fracture FixationDocument3 pagesStrew and Stre H Re Ntion in of Absorbable, Self-Reinforced Polyglycolide (PGA) Rods For Fracture FixationNileshTipanNo ratings yet
- Composites For Bone Repair: Phosphate Glass Fibre Reinforced PLA With Varying Fibre ArchitectureDocument10 pagesComposites For Bone Repair: Phosphate Glass Fibre Reinforced PLA With Varying Fibre ArchitectureNileshTipanNo ratings yet
- Materials in Particulate Form For Tissue Engineering. 2. Applications in BoneDocument13 pagesMaterials in Particulate Form For Tissue Engineering. 2. Applications in BoneNileshTipanNo ratings yet
- Chronology of Bioactive Glass Development and Clinical ApplicationsDocument7 pagesChronology of Bioactive Glass Development and Clinical ApplicationsNileshTipanNo ratings yet
- Complications of Posterior Iliac Crest Bone Grafting in Spine Surgery in ChildrenDocument3 pagesComplications of Posterior Iliac Crest Bone Grafting in Spine Surgery in ChildrenNileshTipanNo ratings yet
- Shaper Tool Head AssemblyDocument6 pagesShaper Tool Head Assemblyjagadeesh01No ratings yet
- Ikada PEreviewDocument16 pagesIkada PEreviewmorychosNo ratings yet
- Lactic Acid Recent Advances in ProductsDocument11 pagesLactic Acid Recent Advances in ProductsMathilda PasaribuNo ratings yet
- Bone Graft For Revision Hip Arthroplasty: Biology and Future Applications Seth C. Gamradt, MD and Jay R. Lieberman, MDDocument12 pagesBone Graft For Revision Hip Arthroplasty: Biology and Future Applications Seth C. Gamradt, MD and Jay R. Lieberman, MDNileshTipanNo ratings yet
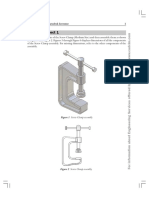
- Student Project 1: Student Projects - Autodesk Inventor 1Document3 pagesStudent Project 1: Student Projects - Autodesk Inventor 1NileshTipan100% (1)
- Stock Bracket AssemblyDocument3 pagesStock Bracket AssemblyAdam Gomez100% (1)
- Press Tool AssemblyDocument2 pagesPress Tool AssemblyVampy SacrificeNo ratings yet
- V Block Assembly TutorialDocument2 pagesV Block Assembly TutorialIlie MarianaNo ratings yet
- Wheel Support Assembly PDFDocument2 pagesWheel Support Assembly PDFManuel Djeredjian100% (1)
- 6BASShock AssemblyDocument3 pages6BASShock AssemblyAlcides Luis Fabián BráñezNo ratings yet
- Module 4 - Speed of SoundDocument16 pagesModule 4 - Speed of SoundLaiza GranaNo ratings yet
- Overhead TankDocument55 pagesOverhead TankamanrajNo ratings yet
- Oslo 1Document69 pagesOslo 1Roberto Carlos Barragán CamposNo ratings yet
- Results and DiscussionDocument2 pagesResults and DiscussionazuldraconNo ratings yet
- The Design of Propeller LED Based On AT89S52Document2 pagesThe Design of Propeller LED Based On AT89S52Nong SuriyaNo ratings yet
- KKS Plant Tagging Procedure - SubmissionDocument71 pagesKKS Plant Tagging Procedure - SubmissionIshwar Alt100% (1)
- Phys 1111 SygsuDocument4 pagesPhys 1111 SygsuLeporeNo ratings yet
- High Voltage EngineeringDocument38 pagesHigh Voltage EngineeringsjNo ratings yet
- Elementary-Lessons - Text in Electricity and MagnetismDocument557 pagesElementary-Lessons - Text in Electricity and MagnetismDhiraj ChaudharyNo ratings yet
- Qualifying Stress Direction From Borehole Shear Sonic Anisotropy PDFDocument11 pagesQualifying Stress Direction From Borehole Shear Sonic Anisotropy PDFLok Bahadur RanaNo ratings yet
- q1wk1 gp1 La1Document1 pageq1wk1 gp1 La1ian babiloniaNo ratings yet
- Enescu M. (Balas)Document6 pagesEnescu M. (Balas)FarahatNo ratings yet
- Application Modules With Demag Dedrive Compact: Complete Solutions For Travel and Lifting ApplicationsDocument2 pagesApplication Modules With Demag Dedrive Compact: Complete Solutions For Travel and Lifting ApplicationsAnonymous v1oFsM6igNo ratings yet
- MODULE 6 - Linear Equations of The First OrderDocument7 pagesMODULE 6 - Linear Equations of The First OrderKNARF FRANKNo ratings yet
- Physics430 Lecture03Document21 pagesPhysics430 Lecture03chaciNo ratings yet
- A Biomechanical Analysis of Rowing (CrossFit Journal)Document7 pagesA Biomechanical Analysis of Rowing (CrossFit Journal)AnaNo ratings yet
- Chem Lab - A Velocity Constant TitrationDocument6 pagesChem Lab - A Velocity Constant TitrationMiguel Ackah-Yensu50% (2)
- 1.0 Introduction To Construction Materials and TestingDocument8 pages1.0 Introduction To Construction Materials and TestingPearl Mae AngusNo ratings yet
- PQP 01 Puc II Maths 2024Document8 pagesPQP 01 Puc II Maths 2024Anagha BLNo ratings yet
- Fenner-Dunlop Conveyor Problems & SolutionsDocument18 pagesFenner-Dunlop Conveyor Problems & Solutionsmickey262010No ratings yet
- Huang 2018Document22 pagesHuang 2018Bendol GalihNo ratings yet
- Full Download Organic Chemistry Wade 8th Edition Test Bank PDF Full ChapterDocument36 pagesFull Download Organic Chemistry Wade 8th Edition Test Bank PDF Full Chapterattabaldigitulejp7tl100% (18)
- Landau RSTDocument11 pagesLandau RSTpbaculimaNo ratings yet
- Thermal Radiation30Document1 pageThermal Radiation30Nirmal SubudhiNo ratings yet
- SKF TMJL 100: Hydraulic PumpDocument8 pagesSKF TMJL 100: Hydraulic PumpreinaldosidejuniorNo ratings yet
- Physics I ProblemsDocument1 pagePhysics I ProblemsbosschellenNo ratings yet
- RIYA Physics ProjectDocument18 pagesRIYA Physics ProjectRiya RoheraNo ratings yet
- GR 12 - Mathematics ATP - 2024Document9 pagesGR 12 - Mathematics ATP - 2024alwandeolwethu36No ratings yet
- Dice Half Life ExperimentDocument1 pageDice Half Life ExperimentEsmond TangNo ratings yet