You might also like
- Endovenous Laser Treatment of Varicose Veins EVLTDocument18 pagesEndovenous Laser Treatment of Varicose Veins EVLTCTAFDocuments100% (1)
- Temporary Pacemakers: Senior Clinical Specialist Medtronic CRDM Central PA DistrictDocument49 pagesTemporary Pacemakers: Senior Clinical Specialist Medtronic CRDM Central PA DistrictHendi Hendi100% (2)
- Hemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHemangiomas, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Atlas of Clinical Vascular MedicineFrom EverandAtlas of Clinical Vascular MedicineMichael R. JaffNo ratings yet
- ArthritisDocument8 pagesArthritissdorji72No ratings yet
- Vasovagal Reflex SyndromeDocument19 pagesVasovagal Reflex SyndromeJalalludin AnNo ratings yet
- Percutaneous Transhepatic Biliary InterventionsDocument11 pagesPercutaneous Transhepatic Biliary InterventionsLe Hu ThaNo ratings yet
- Diabetic UlcerDocument56 pagesDiabetic UlcermucfhsinNo ratings yet
- Jurnal DigestiveDocument9 pagesJurnal DigestiveFrancesc OktofabregasNo ratings yet
- KARDIOMYOPATI - Kuliah DR - ErlinaDocument28 pagesKARDIOMYOPATI - Kuliah DR - ErlinaArif Zulfian MubarokNo ratings yet
- Guidelines 2015 Ed3Document318 pagesGuidelines 2015 Ed3MonicaLadyMelohNo ratings yet
- Veins2 120123093329 Phpapp02Document49 pagesVeins2 120123093329 Phpapp02Yuli Setio Budi PrabowoNo ratings yet
- Syok Hypovolemik-IH FK UMSU2012Document45 pagesSyok Hypovolemik-IH FK UMSU2012Ratika Ayu PiliangNo ratings yet
- Diabetes Mellitus Pada Anak KuliahDocument51 pagesDiabetes Mellitus Pada Anak KuliahNisha AnggiaNo ratings yet
- Penyakit Thromboemboli Vena - DR IsmonDocument27 pagesPenyakit Thromboemboli Vena - DR IsmonSyarif MalawatNo ratings yet
- FAM (Fibroadenoma Mammae)Document4 pagesFAM (Fibroadenoma Mammae)Regia Verent MNo ratings yet
- Temporary Pace MakerDocument32 pagesTemporary Pace Makerpur handayaniNo ratings yet
- Deep Vein ThrombosisDocument16 pagesDeep Vein ThrombosisB1 TutorialNo ratings yet
- Lapsus IFADocument18 pagesLapsus IFAifaNo ratings yet
- Catetan Dekya Radiologi - 20190506102535Document129 pagesCatetan Dekya Radiologi - 20190506102535BakingpancakesNo ratings yet
- Flaps: BY:-Dr. P. Koushik GUIDE: - DR (Brig.) B. B. DograDocument27 pagesFlaps: BY:-Dr. P. Koushik GUIDE: - DR (Brig.) B. B. DograSumit HadgaonkarNo ratings yet
- Metastasis Bone DiseaseDocument11 pagesMetastasis Bone DiseasedrkurniatiNo ratings yet
- Referat: Hernia Nukleus PulposusDocument26 pagesReferat: Hernia Nukleus PulposustebehidayatullahNo ratings yet
- Meningocele BasalisDocument18 pagesMeningocele BasalisCharan Pal SinghNo ratings yet
- Kuliah Spine TraumaDocument91 pagesKuliah Spine Traumatutor tujuhNo ratings yet
- The 'Ins' and 'Outs' of Ureteric ObstructionDocument65 pagesThe 'Ins' and 'Outs' of Ureteric ObstructionThe Kidney ClubNo ratings yet
- Guildelines For Hiv Testing NacoDocument165 pagesGuildelines For Hiv Testing NacoNagendra Singh BeniwalNo ratings yet
- Batu PyelumDocument29 pagesBatu PyelumDanniel KamarudinNo ratings yet
- LONG CASE Luka BakarDocument16 pagesLONG CASE Luka BakarAfiazka LuthfitaNo ratings yet
- Albumin in Liver Cirrhosis, SADocument37 pagesAlbumin in Liver Cirrhosis, SADwinita ViviantiNo ratings yet
- Anatomi Kardio PDFDocument49 pagesAnatomi Kardio PDFDestrini Anjani LandaNo ratings yet
- The Hepatorenal SyndromeDocument26 pagesThe Hepatorenal SyndromeWaraBawanaNo ratings yet
- Diagnosa Dan Tatalaksana Awal Stroke Hemoragik Dan Iskemik Di Igd Pada Era Intervensi NeurologisDocument26 pagesDiagnosa Dan Tatalaksana Awal Stroke Hemoragik Dan Iskemik Di Igd Pada Era Intervensi NeurologisekaNo ratings yet
- DR - TrisuloDocument35 pagesDR - TrisuloZaky prasetyaNo ratings yet
- Acute Limb Ischemia Vs Critical Limb Ischemia: Clinical PracticeDocument51 pagesAcute Limb Ischemia Vs Critical Limb Ischemia: Clinical PracticedrhendyjuniorNo ratings yet
- Role of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy LestariDocument32 pagesRole of DOAC in The Management of COVID-19 Patients: Desak Nyoman Desy Lestaridesy lestariNo ratings yet
- Retinopati DiabetikDocument5 pagesRetinopati DiabetikMuhammad Afriadi HamdanNo ratings yet
- Airway Management - DR Dedi SpAnDocument120 pagesAirway Management - DR Dedi SpAnBagus Abdillah WinataNo ratings yet
- Batu Saluran Kemih: Dr. Suhaemi, SPPD, FinasimDocument57 pagesBatu Saluran Kemih: Dr. Suhaemi, SPPD, FinasimAfri AdiNo ratings yet
- Ahmad Kurnia: Prediksi, Intervensi, Deteksi Dini Kanker PyudaraDocument79 pagesAhmad Kurnia: Prediksi, Intervensi, Deteksi Dini Kanker PyudaraTekkhapulephel ParidudinNo ratings yet
- (Upgraded) BDH6 - Emergency Trauma & Non Trauma UroDocument122 pages(Upgraded) BDH6 - Emergency Trauma & Non Trauma Uronabila safiraNo ratings yet
- Pseudomonad GroupDocument18 pagesPseudomonad GroupNikita MarieNo ratings yet
- 2 DHF InternaDocument59 pages2 DHF Internasaladass 2No ratings yet
- Tumor GinjalDocument63 pagesTumor GinjalNurhidayah100% (1)
- Assessment Pre Op Dan USG - DR MursidDocument27 pagesAssessment Pre Op Dan USG - DR MursidSyarif MalawatNo ratings yet
- Antikoagulan JurnalDocument5 pagesAntikoagulan JurnalansyemomoleNo ratings yet
- Acute Limb IschaemiaDocument32 pagesAcute Limb IschaemiaAnonymous 9wHscM100% (1)
- Biliary Tract Dis Pancreatitis 2015Document143 pagesBiliary Tract Dis Pancreatitis 2015eiad-mahmoudNo ratings yet
- Trombosis Vena Dalam: Pendidikan Kedokteran Berkelanjutan (PKB) XXI 2013Document13 pagesTrombosis Vena Dalam: Pendidikan Kedokteran Berkelanjutan (PKB) XXI 2013IkaNo ratings yet
- Number: JanuaryDocument134 pagesNumber: JanuaryYaz ValenzuelaNo ratings yet
- The Effect of Zinc Supplementation in Adult Patients With Acute Diarrhea PDFDocument5 pagesThe Effect of Zinc Supplementation in Adult Patients With Acute Diarrhea PDFAsrori AzharNo ratings yet
- Acute Scrotum 231016 PDFDocument50 pagesAcute Scrotum 231016 PDFDany Dias100% (1)
- Penile CaDocument76 pagesPenile CaUsmle GuyNo ratings yet
- Management of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientDocument12 pagesManagement of Diabetes and Hyperglycemia in The Hospital: A Practical Guide To Subcutaneous Insulin Use in The Non-Critically Ill, Adult PatientRani Dwi NNo ratings yet
- Management Terapi CairanDocument60 pagesManagement Terapi Cairanpeter singalNo ratings yet
- Ulcera EndovascDocument4 pagesUlcera EndovascGustavo DolinskyNo ratings yet
- 2007bg 11Document6 pages2007bg 11souq alkanzNo ratings yet
- PDF DIR 456Document6 pagesPDF DIR 456Fauzan MaulanaNo ratings yet
- Varicose Vein Treatment Tips and Trick - Ablation or GlueDocument30 pagesVaricose Vein Treatment Tips and Trick - Ablation or GlueNata NakamuraNo ratings yet
- Endovasc VV MXDocument9 pagesEndovasc VV MXdrrochanNo ratings yet
- Microsoft Word - UM001ENG Rev 09 - 1 Cover FRONTDocument4 pagesMicrosoft Word - UM001ENG Rev 09 - 1 Cover FRONTaillNo ratings yet
- Drager Fabius - Technical Documentation PDFDocument205 pagesDrager Fabius - Technical Documentation PDFDronNo ratings yet
- Infinosis T4 IN017703 CEDocument2 pagesInfinosis T4 IN017703 CEaillNo ratings yet
- A-Dec 200 Service Guide 1Document66 pagesA-Dec 200 Service Guide 1aillNo ratings yet
- Hydraulic System: Used On Units With Serial Number AN1000 Thru AN1874Document1 pageHydraulic System: Used On Units With Serial Number AN1000 Thru AN1874aillNo ratings yet
- Fabius GS Premium: SupplementDocument46 pagesFabius GS Premium: SupplementaillNo ratings yet
- Vitamin D Total DS167701 CEDocument2 pagesVitamin D Total DS167701 CEaillNo ratings yet
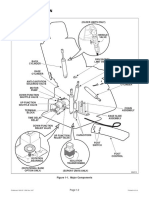
- Section I General Information: Figure 1-1. Major ComponentsDocument1 pageSection I General Information: Figure 1-1. Major ComponentsaillNo ratings yet
- Graduation Projects of 5 Year Students 2018/2019 1-Nameer Afaat Nassar Title: Approaches For The Treatment of Neuropathic PainDocument3 pagesGraduation Projects of 5 Year Students 2018/2019 1-Nameer Afaat Nassar Title: Approaches For The Treatment of Neuropathic PainaillNo ratings yet
- Hydraulic System: Used On Units With Serial Number AN1000 Thru AN1874Document1 pageHydraulic System: Used On Units With Serial Number AN1000 Thru AN1874aillNo ratings yet
- Canon IR 1133 PC PDFDocument56 pagesCanon IR 1133 PC PDFColeaRautuNo ratings yet
- 6328 4136 PDFDocument8 pages6328 4136 PDFsari udinNo ratings yet
- iDE - 1.0.2 - User's ManualDocument9 pagesiDE - 1.0.2 - User's ManualaillNo ratings yet
- Availability Procurement Training Usage MaintenancDocument6 pagesAvailability Procurement Training Usage MaintenancaillNo ratings yet
- 1254 3 Guide KMi KM2i en Bas DefDocument21 pages1254 3 Guide KMi KM2i en Bas DefaillNo ratings yet
- A-Dec Performer Service GuideDocument61 pagesA-Dec Performer Service GuideaillNo ratings yet
- Application Form For Driving License For Saudis Dallah Driving SchoolDocument1 pageApplication Form For Driving License For Saudis Dallah Driving SchoolaillNo ratings yet
- 119 (-001-016) ChairDocument164 pages119 (-001-016) ChairaillNo ratings yet
- Brochure Safer English 2012 ADocument2 pagesBrochure Safer English 2012 AaillNo ratings yet
- Whole Blood Analysis (Full Blood Count-FBC) Using SYSMEX XE-2100 Haematology Automated AnalyserDocument16 pagesWhole Blood Analysis (Full Blood Count-FBC) Using SYSMEX XE-2100 Haematology Automated AnalyserFULGENCE RUHARARANo ratings yet
- User+And+Service+Manual-+BSC NC2 V.B April+2013-1 PDFDocument70 pagesUser+And+Service+Manual-+BSC NC2 V.B April+2013-1 PDFCarlos VillanuevaNo ratings yet
- Comp Pocket Guide FABIUS PDFDocument80 pagesComp Pocket Guide FABIUS PDFrahim iqbalNo ratings yet
- Repair Instructions: EBA 20 Eba 20 CDocument31 pagesRepair Instructions: EBA 20 Eba 20 CDian Gusti RamadhonaNo ratings yet
- Hydraulic System: Used On Units With Serial Number AN1000 Thru AN1874Document1 pageHydraulic System: Used On Units With Serial Number AN1000 Thru AN1874aillNo ratings yet
- DownloadDocument1 pageDownloadaillNo ratings yet
- CoolBlue Duet - Cooltouch - PDF Catalogs - Technical DocumentationDocument6 pagesCoolBlue Duet - Cooltouch - PDF Catalogs - Technical DocumentationaillNo ratings yet
- Cypress Catalog EngDocument33 pagesCypress Catalog EngTunone Julius0% (1)
- SB MembershipDocument7 pagesSB MembershipaillNo ratings yet
- A-Dec Performer Service GuideDocument61 pagesA-Dec Performer Service GuideaillNo ratings yet
- Function Description Fabius GS: 3 Battery BackupDocument1 pageFunction Description Fabius GS: 3 Battery BackupaillNo ratings yet
- AeglemarmelosDocument4 pagesAeglemarmelosKrutika SNo ratings yet
- Bermuda GrassDocument20 pagesBermuda GrassFurious AssassinNo ratings yet
- Clinical Manifestations and Diagnosis of Rotavirus InfectionDocument21 pagesClinical Manifestations and Diagnosis of Rotavirus Infectiondaniso12No ratings yet
- Parent Brochure PDFDocument2 pagesParent Brochure PDFUme NaomiNo ratings yet
- PLE Practice Exam Day 4Document7 pagesPLE Practice Exam Day 4Sanielle Karla Garcia LorenzoNo ratings yet
- Drugs Used in AneasthesiaDocument73 pagesDrugs Used in AneasthesiaCabdiladif Ahmed McrfNo ratings yet
- New Home of The Divine Intervention Step 2 Podcast NotesDocument399 pagesNew Home of The Divine Intervention Step 2 Podcast NotespavithraNo ratings yet
- Neuritis OpticDocument13 pagesNeuritis OpticBimo Nugroho saktiNo ratings yet
- Test Bank For Health Psychology Biopsychosocial Interactions 9th Edition Edward P Sarafino Timothy W SmithDocument17 pagesTest Bank For Health Psychology Biopsychosocial Interactions 9th Edition Edward P Sarafino Timothy W SmithMary Bartolomeo100% (34)
- Final Synopsis Format Sample ACNDocument25 pagesFinal Synopsis Format Sample ACNAbhijit DasNo ratings yet
- Pleural Effusion - ClinicalKeyDocument13 pagesPleural Effusion - ClinicalKeyWialda Dwi rodyahNo ratings yet
- Chapter 7 Deaths From AsphyxiaDocument12 pagesChapter 7 Deaths From AsphyxiaJm Lanaban0% (1)
- Cold Sinus Sore Throat Tonsillitis Fever and Flu PDFDocument4 pagesCold Sinus Sore Throat Tonsillitis Fever and Flu PDFAnna GalánNo ratings yet
- Jadavpur University: CollegeDocument22 pagesJadavpur University: CollegekuntaljuNo ratings yet
- Quiz 17 - Cancer-Emergencies-Toxicology Básicos e Intermedios (Hoja Alumno) CortoDocument3 pagesQuiz 17 - Cancer-Emergencies-Toxicology Básicos e Intermedios (Hoja Alumno) CortoCynthia Argüelles GuzmánNo ratings yet
- Health Social Care Comm - 2021 - Sarabia Cobo - Comparison Between Attention and Experiences of Chronic Complex Patients ADocument12 pagesHealth Social Care Comm - 2021 - Sarabia Cobo - Comparison Between Attention and Experiences of Chronic Complex Patients AGabriel MoraguesNo ratings yet
- 118A - Chapter 1 - CRITICAL CARE NURSING LEC (EDITED) Handout #1Document14 pages118A - Chapter 1 - CRITICAL CARE NURSING LEC (EDITED) Handout #1Joanna Taylan100% (5)
- C40-203 c40-203 Dalmau SyllabiDocument8 pagesC40-203 c40-203 Dalmau SyllabiserftyNo ratings yet
- ReferenceDocument7 pagesReferenceElsa Christy GumayNo ratings yet
- Application of The Ecological Framework in Depression 2013Document7 pagesApplication of The Ecological Framework in Depression 2013Laura Larrea MantillaNo ratings yet
- TE2 - 15 JunDocument186 pagesTE2 - 15 JunPTchongNo ratings yet
- CITY OF BACOOR - BeGIn CEIRDocument3 pagesCITY OF BACOOR - BeGIn CEIRfrance dicenNo ratings yet
- Machine Learning Approach For Acute Respiratory Infections (ISPA) Prediction: Case Study IndonesiaDocument5 pagesMachine Learning Approach For Acute Respiratory Infections (ISPA) Prediction: Case Study IndonesiaSasmita DewiNo ratings yet
- 1st - ICNHT - Paper - 112 Irene Hutagalung, Revisi 3Document7 pages1st - ICNHT - Paper - 112 Irene Hutagalung, Revisi 3Veronika HutagalungNo ratings yet
- RSP Exam-PracticeDocument8 pagesRSP Exam-PracticeJoe JohnNo ratings yet
- Pulmonary Embolism: Amina Adel Al-QaysiDocument37 pagesPulmonary Embolism: Amina Adel Al-QaysiJasleen Kaur100% (2)
- LANCET LOCKDOWN NO MORTALITY BENEFIT A Country Level Analysis Measuring The Impact of Government ActionsDocument8 pagesLANCET LOCKDOWN NO MORTALITY BENEFIT A Country Level Analysis Measuring The Impact of Government ActionsRoger EarlsNo ratings yet
- Skills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCDocument7 pagesSkills Assessment Checklist: MODULE 6: Massive Hemorrhage Control in TFCSae TumNo ratings yet
- Media Hypes Moderna's COVID Vaccine, Downplays Risks - Children's Health DefenseDocument10 pagesMedia Hypes Moderna's COVID Vaccine, Downplays Risks - Children's Health DefenseDMDONo ratings yet
- MARFANDocument17 pagesMARFANfdgrgNo ratings yet