You might also like
- Chapter 2 - Electrocardiographs - 2021 - Medical Device TechnologiesDocument27 pagesChapter 2 - Electrocardiographs - 2021 - Medical Device TechnologiesPierre PradelNo ratings yet
- Case 37-2020: A 35-Year-Old Man With Lymphadenopathy and PetechiaeDocument11 pagesCase 37-2020: A 35-Year-Old Man With Lymphadenopathy and PetechiaePatriciaNo ratings yet
- Guardia LombardiDocument16 pagesGuardia LombardiCyrus Yu Shing ChanNo ratings yet
- Nejmcpc 2115850Document9 pagesNejmcpc 2115850masonicpgsNo ratings yet
- Caso Clinico NejDocument9 pagesCaso Clinico NejSilvina MartinezNo ratings yet
- Nej M CPC 2309382Document8 pagesNej M CPC 2309382mnf6bb2tckNo ratings yet
- Case 14-2020: A 37-Year-Old Man With Joint Pain and Eye RednessDocument9 pagesCase 14-2020: A 37-Year-Old Man With Joint Pain and Eye RednessWho's Alewii?No ratings yet
- Case 11 - FisiopatologiaDocument10 pagesCase 11 - FisiopatologiaSamuil MuralesNo ratings yet
- Case 14-2020: A 37-Year-Old Man With Joint Pain and Eye RednessDocument9 pagesCase 14-2020: A 37-Year-Old Man With Joint Pain and Eye RednessGénesis LeónNo ratings yet
- Case 15-2018: An 83-Year-Old Woman With Nausea, Vomiting, and ConfusionDocument8 pagesCase 15-2018: An 83-Year-Old Woman With Nausea, Vomiting, and ConfusionivanNo ratings yet
- Nejmcpc 2100283Document9 pagesNejmcpc 2100283Jonas DiazNo ratings yet
- Case 9-2021: A 16-Year-Old Boy With Headache, Abdominal Pain, and HypertensionDocument11 pagesCase 9-2021: A 16-Year-Old Boy With Headache, Abdominal Pain, and HypertensionPaulo Ricardo D. PereiraNo ratings yet
- Nej M CPC 1209935Document9 pagesNej M CPC 1209935drfmentNo ratings yet
- Caso 3Document12 pagesCaso 3Luanna DávilaNo ratings yet
- 2020 Case 23-2020, A 76-Year-Old Woman Who Died From Covid-19Document8 pages2020 Case 23-2020, A 76-Year-Old Woman Who Died From Covid-19alejandromfunes1749No ratings yet
- Nej M CPC 1900142Document11 pagesNej M CPC 1900142arthur andreNo ratings yet
- Nejmcpc 1909624Document10 pagesNejmcpc 1909624SrivarrdhiniNo ratings yet
- A 25-Year-Old Man With New-Onset Seizures PDFDocument8 pagesA 25-Year-Old Man With New-Onset Seizures PDFMr. LNo ratings yet
- Nejm CASODocument9 pagesNejm CASOJuan Esteban Rincon HuertasNo ratings yet
- Case 9-2017: A 27-Year-Old Woman With Nausea, Vomiting, Confusion, and HyponatremiaDocument9 pagesCase 9-2017: A 27-Year-Old Woman With Nausea, Vomiting, Confusion, and HyponatremiaLindia PrabhaswariNo ratings yet
- Nej M CPC 2115849Document13 pagesNej M CPC 2115849Dinesh KumaarNo ratings yet
- Mialgia e Fraqueza MuscularDocument8 pagesMialgia e Fraqueza MuscularCelia AlcantaraNo ratings yet
- Uso CorticoidesDocument9 pagesUso CorticoidesRolando Lopez ZegarraNo ratings yet
- Case Report: Severe Hyperbilirubinemia: A Rare Complication of Lyme DiseaseDocument4 pagesCase Report: Severe Hyperbilirubinemia: A Rare Complication of Lyme DiseaseDhruva PatelNo ratings yet
- Acute Kidney FailureDocument8 pagesAcute Kidney FailureJuan Diego Ferreyros ArroyoNo ratings yet
- Case 12-2020: A 24-Year-Old Man With Fever, Cough, and DyspneaDocument10 pagesCase 12-2020: A 24-Year-Old Man With Fever, Cough, and DyspneatabareeNo ratings yet
- Case 1-2010Document11 pagesCase 1-2010isravg94No ratings yet
- DiagnosisDocument6 pagesDiagnosisZackNo ratings yet
- Case Report DSSDocument3 pagesCase Report DSSVivi DeviyanaNo ratings yet
- Morris 2018Document9 pagesMorris 2018AdrianNo ratings yet
- New England PancreatiteDocument9 pagesNew England PancreatiteLauren ReckNo ratings yet
- Arvika R 2019Document11 pagesArvika R 2019Lucas BrasilNo ratings yet
- Hari-3 - 02 - Dr. Alindina - Demam TifoidDocument33 pagesHari-3 - 02 - Dr. Alindina - Demam TifoidmodrsbmNo ratings yet
- Nejmcpc 2300910Document9 pagesNejmcpc 2300910carb0ne14rNo ratings yet
- A 26-Year-Old White Man With A Systemic Lupus Erythematosus Flare and Acute Multiorgan Ischemia: Vasculitis or Thrombosis?Document9 pagesA 26-Year-Old White Man With A Systemic Lupus Erythematosus Flare and Acute Multiorgan Ischemia: Vasculitis or Thrombosis?Wendy SetiawanNo ratings yet
- Nejmcpc 1904048Document10 pagesNejmcpc 1904048luca.win92No ratings yet
- XcaretDocument9 pagesXcaretmubarek abdurohemanNo ratings yet
- Case 3-2019 - A 70-Year-Old Woman With Fever, Headache, and Progressive Encephalopathy - Zachary Et Al - 2019Document8 pagesCase 3-2019 - A 70-Year-Old Woman With Fever, Headache, and Progressive Encephalopathy - Zachary Et Al - 2019nejdNo ratings yet
- Cabot 2007Document10 pagesCabot 2007Luis Andres Villar InfanteNo ratings yet
- Hepatit Kaj SkarlatinaDocument2 pagesHepatit Kaj SkarlatinaIrena PopovaNo ratings yet
- Hiding in The Water: Clinical Problem-SolvingDocument6 pagesHiding in The Water: Clinical Problem-SolvingtabareeNo ratings yet
- Case 22-2017: A 21-Year-Old Woman With Fever, Headache, and MyalgiasDocument11 pagesCase 22-2017: A 21-Year-Old Woman With Fever, Headache, and MyalgiasMaria Dolores Herrero MendozaNo ratings yet
- Case 11-2009 - A 47-Year-Old Man With Fever, Headache, Rash, and VomitingDocument9 pagesCase 11-2009 - A 47-Year-Old Man With Fever, Headache, Rash, and VomitingcmirceaNo ratings yet
- Mortality Report April 25th 2019Document12 pagesMortality Report April 25th 2019ramotNo ratings yet
- Case 18 - 2009Document9 pagesCase 18 - 2009Gustavo AngelesNo ratings yet
- Case 17-2020: A 68-Year-Old Man With Covid-19 and Acute Kidney InjuryDocument10 pagesCase 17-2020: A 68-Year-Old Man With Covid-19 and Acute Kidney Injurymichal ben meronNo ratings yet
- RF Students Guide Revised 2020 - CBB - MDCDocument3 pagesRF Students Guide Revised 2020 - CBB - MDCFranclem TecsonNo ratings yet
- Marine-Lenhart Syndrome Case ReportDocument5 pagesMarine-Lenhart Syndrome Case ReportEliana InsaurraldeNo ratings yet
- Case 35-2021: A 50-Year-Old Woman With Pain in The Left Upper Quadrant and HypoxemiaDocument7 pagesCase 35-2021: A 50-Year-Old Woman With Pain in The Left Upper Quadrant and HypoxemiaRaul DoctoNo ratings yet
- Caso Clinico New England.Document35 pagesCaso Clinico New England.CarolinaNo ratings yet
- 10 1056@NEJMcpc1913468 PDFDocument10 pages10 1056@NEJMcpc1913468 PDFAbdelkader HociniNo ratings yet
- Caso Especial Grupo 1Document18 pagesCaso Especial Grupo 1Josè BermúdezNo ratings yet
- Caso 1Document14 pagesCaso 1Luanna DávilaNo ratings yet
- NCP 1Document5 pagesNCP 1Butchie's ParadiseNo ratings yet
- Dengue Hemorrhagic Fever Complicated by PancreatitisDocument3 pagesDengue Hemorrhagic Fever Complicated by PancreatitisLaras SetyowatiNo ratings yet
- Typhoid FeverDocument17 pagesTyphoid FeverKyle Margaret Flores100% (1)
- 65-Year-Old Man With Persistent FeverDocument4 pages65-Year-Old Man With Persistent FeverZé Da SilvaNo ratings yet
- Clinical Communications: Pediatric: Pediatric Sepsis Secondary To An Occult Dental Abscess: A Case ReportDocument5 pagesClinical Communications: Pediatric: Pediatric Sepsis Secondary To An Occult Dental Abscess: A Case Reportdelfi simatupangNo ratings yet
- Thornton 2016Document5 pagesThornton 2016AfdhalRuslanNo ratings yet
- Case 2-2019 - A 36-Year-Old Man With Rash, Abdominal Pain, and Lymphadenopathy - Chen Et Al - 2019Document9 pagesCase 2-2019 - A 36-Year-Old Man With Rash, Abdominal Pain, and Lymphadenopathy - Chen Et Al - 2019nejdNo ratings yet
- A Gene Primer for Health Care Providers: The Genomics of Cirs and Associated Molecular PathwaysFrom EverandA Gene Primer for Health Care Providers: The Genomics of Cirs and Associated Molecular PathwaysNo ratings yet
- Atomic Clocks PredictionsDocument4 pagesAtomic Clocks PredictionsPierre PradelNo ratings yet
- Aragao 2020 Many Shades of Wrong What GovernmenDocument27 pagesAragao 2020 Many Shades of Wrong What GovernmenPierre PradelNo ratings yet
- A Blue Sky HistoryDocument9 pagesA Blue Sky HistoryPierre PradelNo ratings yet
- 22 of The Most Incredible - First - Pictures From HistoryDocument23 pages22 of The Most Incredible - First - Pictures From HistoryPierre PradelNo ratings yet
- High AltitudeDocument10 pagesHigh AltitudePierre PradelNo ratings yet
- Cranial Nerves in Health and Disease (2nd Edition) - (XI. Accessory Nerve)Document11 pagesCranial Nerves in Health and Disease (2nd Edition) - (XI. Accessory Nerve)Pierre PradelNo ratings yet
- 02 Pedros1999Document10 pages02 Pedros1999Pierre PradelNo ratings yet
- The Doctor's Oldest Tool: PerspectiveDocument3 pagesThe Doctor's Oldest Tool: PerspectivePierre PradelNo ratings yet
- 04 Tena2000Document4 pages04 Tena2000Pierre PradelNo ratings yet
- Cochlear Implants: Chapter OutlineDocument24 pagesCochlear Implants: Chapter OutlinePierre PradelNo ratings yet
- Electrocardiograph Filtering Lab: Chapter OutlineDocument6 pagesElectrocardiograph Filtering Lab: Chapter OutlinePierre PradelNo ratings yet
- Chapter 13 Electroencephalographs 2021 Medical Device TechnologiesDocument21 pagesChapter 13 Electroencephalographs 2021 Medical Device TechnologiesPierre PradelNo ratings yet
- Cranial Nerves: in Health and DiseaseDocument2 pagesCranial Nerves: in Health and DiseasePierre PradelNo ratings yet
- 01 Hartley99Document19 pages01 Hartley99Pierre PradelNo ratings yet
- CHAPTER 1 - Biochemistry & Amp MedicineDocument6 pagesCHAPTER 1 - Biochemistry & Amp MedicinePierre PradelNo ratings yet
- Morphological Properties of Atmospheric Aerosol Aggregates: C. Xiong and S. K. FriedlanderDocument6 pagesMorphological Properties of Atmospheric Aerosol Aggregates: C. Xiong and S. K. FriedlanderPierre PradelNo ratings yet
- Extended Log-Normal Method of Moments For Solving The Population Balance Equation For Brownian CoagulationDocument13 pagesExtended Log-Normal Method of Moments For Solving The Population Balance Equation For Brownian CoagulationPierre PradelNo ratings yet
- Copyright 2021 Medical-Device-TechnologiesDocument1 pageCopyright 2021 Medical-Device-TechnologiesPierre PradelNo ratings yet
- Free AgentsDocument5 pagesFree AgentsPierre PradelNo ratings yet
- Change of Particle Size Distribution During Brownian CoagulationDocument11 pagesChange of Particle Size Distribution During Brownian CoagulationPierre PradelNo ratings yet
- New Microsoft Office Word DocumentDocument9 pagesNew Microsoft Office Word DocumentGaurav JaiswalNo ratings yet
- Well Stimulation ServicesDocument6 pagesWell Stimulation ServicesAfzal AktharNo ratings yet
- Simple Annuities FinalDocument95 pagesSimple Annuities FinalMae Ann KongNo ratings yet
- Environmental Engineering IDocument8 pagesEnvironmental Engineering ICharan ReddyNo ratings yet
- BrochureDocument20 pagesBrochuresitaNo ratings yet
- Module 4 - Lateral Force Procedure-Design Base ShearDocument6 pagesModule 4 - Lateral Force Procedure-Design Base ShearClarize MikaNo ratings yet
- 14 StatisticsDocument15 pages14 StatisticsDROZON GAMING YTNo ratings yet
- PAT TestDocument20 pagesPAT TestLuffy11No ratings yet
- Guwahati Conference Circular 1Document5 pagesGuwahati Conference Circular 1Phyoben S OdyuoNo ratings yet
- Sandy Point Brochure 2016Document7 pagesSandy Point Brochure 2016miller999No ratings yet
- Near Field Communication Based College CanteenDocument5 pagesNear Field Communication Based College CanteenJunaid M FaisalNo ratings yet
- The Phantom of The OperaDocument272 pagesThe Phantom of The OperaJames Andrew CurtisNo ratings yet
- EHB - en - File - 9.7.3 Equivalent ASME EN Materials PDFDocument3 pagesEHB - en - File - 9.7.3 Equivalent ASME EN Materials PDFks2000n1No ratings yet
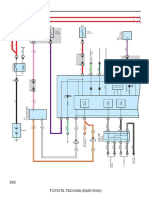
- Combination Meter: 262 Toyota Tacoma (Em01D0U)Document6 pagesCombination Meter: 262 Toyota Tacoma (Em01D0U)hamayunNo ratings yet
- Ef 2000 TestingDocument12 pagesEf 2000 TestingLeiser HartbeckNo ratings yet
- Polar Coordinates NotesDocument15 pagesPolar Coordinates NotesEnzo OoiNo ratings yet
- Case of Paper BoatDocument11 pagesCase of Paper BoatAshiqnavaz ShaikhNo ratings yet
- Mba Group ActivityDocument14 pagesMba Group ActivitySHERYL SHEKINAH E ARCH-2019 BATCHNo ratings yet
- Tion PaperDocument15 pagesTion PaperSachin ChakradharNo ratings yet
- Rayo X Protable XFM ITALRAYDocument18 pagesRayo X Protable XFM ITALRAYaplicacionista.imagenesNo ratings yet
- L4 - Structure of Metals - EMPDocument8 pagesL4 - Structure of Metals - EMPkopkash123No ratings yet
- Proline Promass 83 Profibus Dp/Pa: Description of Device FunctionsDocument182 pagesProline Promass 83 Profibus Dp/Pa: Description of Device FunctionsHectorNo ratings yet
- Group1 OB Ward-Case StudyDocument10 pagesGroup1 OB Ward-Case StudyAnthony Seth AguilandoNo ratings yet
- Aujeszky's DiseaseDocument30 pagesAujeszky's DiseaseFrances ChewNo ratings yet
- Curriculum Vitae: Personal InformationDocument10 pagesCurriculum Vitae: Personal InformationBehairy AhmedNo ratings yet
- Cybernetic Tradition 1Document15 pagesCybernetic Tradition 1Jenina CuevasNo ratings yet
- Area of A CircleDocument2 pagesArea of A CircleHandri eko100% (1)
- The LEGO Adventure BookDocument194 pagesThe LEGO Adventure BookBenjamin De AlexandrisNo ratings yet
- K ServerDocument11 pagesK Serveraryatel26No ratings yet