You might also like
- 2021 YRBS National HS QuestionnaireDocument24 pages2021 YRBS National HS Questionnairermconvidhya sri2015No ratings yet
- IndianJContNsgEdn17169-1808062 050120Document6 pagesIndianJContNsgEdn17169-1808062 050120rmconvidhya sri2015No ratings yet
- OSPE - Child HN - Station BankDocument245 pagesOSPE - Child HN - Station Bankrmconvidhya sri2015No ratings yet
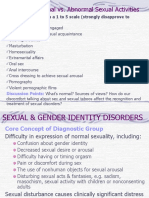
- Sexual & Gender Identity DisordersDocument41 pagesSexual & Gender Identity Disordersrmconvidhya sri2015No ratings yet
- Appleby Uta 2502D 12845Document240 pagesAppleby Uta 2502D 12845rmconvidhya sri2015No ratings yet
- PM CARES UPI Receipt 010021238073 10112020 754Document1 pagePM CARES UPI Receipt 010021238073 10112020 754rmconvidhya sri2015No ratings yet
- Wa0022.Document2 pagesWa0022.rmconvidhya sri2015No ratings yet
- Prototype File For Staff NursesDocument10 pagesPrototype File For Staff Nurseskrishnasree71% (14)
- AIIMS Delhi Technician Radiology ResultDocument6 pagesAIIMS Delhi Technician Radiology Resultrmconvidhya sri2015No ratings yet
- C4D Vac CS 2021Document18 pagesC4D Vac CS 2021rmconvidhya sri2015No ratings yet
- Drug ComplianceDocument30 pagesDrug Compliancermconvidhya sri2015No ratings yet
- WFP 0000102103Document119 pagesWFP 0000102103rmconvidhya sri2015No ratings yet
- School of Nursi-Wps OfficeDocument1 pageSchool of Nursi-Wps Officermconvidhya sri2015No ratings yet
- Clinical Teaching MethodsDocument13 pagesClinical Teaching Methodsrmconvidhya sri2015No ratings yet
- Neurotransmitte-WPS OfficeDocument5 pagesNeurotransmitte-WPS Officermconvidhya sri2015No ratings yet
- Abhasa Is situa-WPS OfficeDocument10 pagesAbhasa Is situa-WPS Officermconvidhya sri2015No ratings yet
- Data Analysis MHN - 1Document14 pagesData Analysis MHN - 1rmconvidhya sri2015No ratings yet
- Effectiveness of BCC program on adolescent risk awarenessDocument8 pagesEffectiveness of BCC program on adolescent risk awarenessrmconvidhya sri2015No ratings yet
- Happy Minds, R-WPS OfficeDocument4 pagesHappy Minds, R-WPS Officermconvidhya sri2015No ratings yet
- Requirements 6Document1 pageRequirements 6rmconvidhya sri2015No ratings yet
- ESsAy Type TestDocument6 pagesESsAy Type Testrmconvidhya sri2015No ratings yet
- Supply and Inst-Wps OfficeDocument1 pageSupply and Inst-Wps Officermconvidhya sri2015No ratings yet
- Code of EthicsDocument17 pagesCode of EthicsSundaraBharathi100% (2)
- Open navigation-WPS OfficeDocument22 pagesOpen navigation-WPS Officermconvidhya sri2015No ratings yet
- Scientific Research PresentationDocument2 pagesScientific Research Presentationrmconvidhya sri2015No ratings yet
- PHYSICAL LAYOUT-WPS OfficeDocument18 pagesPHYSICAL LAYOUT-WPS Officermconvidhya sri2015No ratings yet
- University VisitDocument10 pagesUniversity Visitrmconvidhya sri2015No ratings yet
- Competence-based learning: Core skills for 21st century successDocument7 pagesCompetence-based learning: Core skills for 21st century successrmconvidhya sri2015No ratings yet
- One of The feat-WPS OfficeDocument12 pagesOne of The feat-WPS Officermconvidhya sri2015No ratings yet
- Requirements 3-WPS OfficeDocument1 pageRequirements 3-WPS Officermconvidhya sri2015No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Emotional and Psychological Aspects of Therapeutic CommunityDocument20 pagesEmotional and Psychological Aspects of Therapeutic CommunityAlexander RamosNo ratings yet
- Therapeutic Modalities (Ca3) : Week 2 Topic: Therapeutic Community PrinciplesDocument11 pagesTherapeutic Modalities (Ca3) : Week 2 Topic: Therapeutic Community PrinciplesKate Serrano ManlutacNo ratings yet
- 1 1KimHarveyGroupDocument41 pages1 1KimHarveyGroupashNo ratings yet
- Therapeutic Modality Treatment Models RehabilitationDocument4 pagesTherapeutic Modality Treatment Models RehabilitationjohnpaulacostaNo ratings yet
- TC Modalities Help RehabilitationDocument5 pagesTC Modalities Help RehabilitationMarco Paolo PasnoNo ratings yet
- ErminaDocument32 pagesErminaMichael John Canare GloriaNo ratings yet
- Time Space Power and The Liminal TransfoDocument38 pagesTime Space Power and The Liminal TransfoGonzaloNo ratings yet
- M. KOOYMAN The Therapeutic Community and The Medical Model PDFDocument12 pagesM. KOOYMAN The Therapeutic Community and The Medical Model PDFLagusNo ratings yet
- CA 3 Therapeutic Modalities 1Document10 pagesCA 3 Therapeutic Modalities 1Alfred Louis Salivia DizonNo ratings yet
- UntitledDocument32 pagesUntitledAsmaa AyadNo ratings yet
- Lesson 3. Underlying Therapeutic Community PrinciplesDocument2 pagesLesson 3. Underlying Therapeutic Community PrinciplesBrielle Shai CruzNo ratings yet
- Psych - Chapter 23 Into To Milieu ManagementDocument4 pagesPsych - Chapter 23 Into To Milieu ManagementKaren かれんNo ratings yet
- Therapeuti C Modalities: Prepared By: John Patrick B. de JesusDocument183 pagesTherapeuti C Modalities: Prepared By: John Patrick B. de JesusJohnpatrick Dejesus100% (2)
- Introduction To Therapeutic Community Program in The Philippines Effectiveness of Therapeutic Community Modality ProgramDocument10 pagesIntroduction To Therapeutic Community Program in The Philippines Effectiveness of Therapeutic Community Modality ProgramJehad AntaoNo ratings yet
- TC OverviewDocument20 pagesTC OverviewFear Neuj ZhelmiNo ratings yet
- Therapeutic Community RelationshipsDocument5 pagesTherapeutic Community RelationshipsGesler Pilvan SainNo ratings yet
- TherapeuticDocument55 pagesTherapeuticmaredelledemillo2002No ratings yet
- Aa Dindu KavaliDocument87 pagesAa Dindu KavaliSajanChandra50% (16)
- Rehabilitation Through Community IntegrationDocument5 pagesRehabilitation Through Community IntegrationJoseph renz AndayaNo ratings yet
- MILIEU THERAPY-THE THERAPEUTIC ENVIRONMENTDocument2 pagesMILIEU THERAPY-THE THERAPEUTIC ENVIRONMENTsivagiri.pNo ratings yet
- Deacon Patricio Torres-Lisboa, M.D., Is Originally From Chile. He Graduated From TheDocument17 pagesDeacon Patricio Torres-Lisboa, M.D., Is Originally From Chile. He Graduated From Theotorres@med.puc.clNo ratings yet
- Group 4 Therapeutic ModalitiesDocument4 pagesGroup 4 Therapeutic ModalitiesChinky IbarraNo ratings yet
- Milieu TherapyDocument22 pagesMilieu TherapyAnusikta PandaNo ratings yet
- Milieu Therapy & Therapeutic CommunityDocument30 pagesMilieu Therapy & Therapeutic CommunitySaritha SvNo ratings yet
- Ca3 Week1 ModuleDocument16 pagesCa3 Week1 ModuleKate Serrano ManlutacNo ratings yet
- Therapeutic Modalities: Prepared By: John Patrick B. de JesusDocument55 pagesTherapeutic Modalities: Prepared By: John Patrick B. de JesusAngelie Regie EstorqueNo ratings yet
- LEC 2015 Pre-Test in Correctional Ad (CA 101-102) For FBDocument10 pagesLEC 2015 Pre-Test in Correctional Ad (CA 101-102) For FBcriminologyallianceNo ratings yet
- Frontline Services Correction and Rehabilitation of Penitent OffendersDocument11 pagesFrontline Services Correction and Rehabilitation of Penitent OffendersMichael Egot88% (17)
- Topic 1. Concept of Therapeutic ModalityDocument44 pagesTopic 1. Concept of Therapeutic ModalityKaneki Ken100% (1)
- The Role of Horticultural Therapy in The Therapeutic CommunityDocument5 pagesThe Role of Horticultural Therapy in The Therapeutic CommunityKritikou1547No ratings yet