You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Periodic Table of ElementsDocument1 pagePeriodic Table of ElementsRintuNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Biological MacromoleculesDocument8 pagesBiological MacromoleculesRintuNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
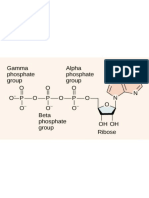
- 0 0 0 o P-0-P-0-P-0 - : Gamma Alpha Phosphate Phosphate Group Group I II IDocument10 pages0 0 0 o P-0-P-0-P-0 - : Gamma Alpha Phosphate Phosphate Group Group I II IRintuNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Counseling PsychologyDocument25 pagesCounseling PsychologyRintuNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Myers Treatment of Abnormal Behavior NotesDocument9 pagesMyers Treatment of Abnormal Behavior NotesRintuNo ratings yet
- Historical Antecedents of OBDocument10 pagesHistorical Antecedents of OBRintuNo ratings yet
- Psychological Capital Self-Efficacy Motivation: 1. Positive Leadership TheoryDocument6 pagesPsychological Capital Self-Efficacy Motivation: 1. Positive Leadership TheoryRintuNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Classification in DSM-5Document7 pagesClassification in DSM-5RintuNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Challenges in OBDocument9 pagesChallenges in OBRintuNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Developmental DisordersDocument6 pagesDevelopmental DisordersRintuNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Social Influence On BehaviorDocument4 pagesSocial Influence On BehaviorRintuNo ratings yet
- Psychology 1000 StressDocument27 pagesPsychology 1000 StressjohnNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Janet Am J PsychiatDocument13 pagesJanet Am J PsychiatMaria CarolinaNo ratings yet
- Dissociative DisordersDocument6 pagesDissociative Disordersramkumar kirubaharanNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- CH 14 Psych DisordersDocument9 pagesCH 14 Psych Disordersюрий локтионовNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- MaryamNawaz Final Paper-1Document50 pagesMaryamNawaz Final Paper-1Hadeeba SadafNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Somatic Symptom and Related Disorders and Dissociative DisordersDocument3 pagesSomatic Symptom and Related Disorders and Dissociative DisordersCalli AndersonNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Annotated BibliographyDocument7 pagesAnnotated Bibliographyapi-340360607No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Study On Clinical Presentations, Level of Stress & Role of Family Environment Among Dissociative Disorder PatientsDocument10 pagesStudy On Clinical Presentations, Level of Stress & Role of Family Environment Among Dissociative Disorder PatientsIJAR JOURNALNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Study of Criminals and Criminal BehaviorDocument5 pagesThe Study of Criminals and Criminal BehaviorBianca CatasioNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- NURSING PRACTICE TEST I - Foundation of PROFESSIONAL Nursing Practice General InstructionsDocument9 pagesNURSING PRACTICE TEST I - Foundation of PROFESSIONAL Nursing Practice General InstructionsjcruzadaNo ratings yet
- Multiple Personality and Channeling - Rayna L. Rogers, D.O.Document11 pagesMultiple Personality and Channeling - Rayna L. Rogers, D.O.XScribderNo ratings yet
- Dissociative DisorderDocument44 pagesDissociative DisorderKiaraMaeRhiasNo ratings yet
- ACross CulturalTestoftheTraumaModelofDissociation2Document24 pagesACross CulturalTestoftheTraumaModelofDissociation2Fulop NoemiNo ratings yet
- TulpaDocument13 pagesTulpaRoberto QuirozNo ratings yet
- TB1 Chapter 15 - Multiple ChoiceDocument36 pagesTB1 Chapter 15 - Multiple ChoiceMonicaNo ratings yet
- Social Media As An Incubator of Personality and Behavioral Psychopathology: Symptom and Disorder Authenticity or Psychosomatic Social Contagion?Document5 pagesSocial Media As An Incubator of Personality and Behavioral Psychopathology: Symptom and Disorder Authenticity or Psychosomatic Social Contagion?IndScenNo ratings yet
- 1991-92 San Diego County Grand Jury, Report 8, Child Sexual Abuse, Assault, and Molest IssuesDocument25 pages1991-92 San Diego County Grand Jury, Report 8, Child Sexual Abuse, Assault, and Molest IssuesRick Thoma100% (1)
- Abnormal PsikologiDocument20 pagesAbnormal PsikologiShalma MisbahulNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Too Soon Old, Too Late Smart - Thirty True Things You Need To Know NowDocument101 pagesToo Soon Old, Too Late Smart - Thirty True Things You Need To Know NowGodhavari83% (6)
- A Fractured Mind by Robert BDocument5 pagesA Fractured Mind by Robert Bapi-4550416880% (4)
- Psychopathology Unit - 1: Abnormality and NormalityDocument37 pagesPsychopathology Unit - 1: Abnormality and NormalityNehaNo ratings yet
- Eve Lorgen - Trauma Based Mind ControlDocument3 pagesEve Lorgen - Trauma Based Mind ControlEU-MindControl67% (3)
- Psychology 3E: Saundra K. Ciccarelli, J. Noland WhiteDocument40 pagesPsychology 3E: Saundra K. Ciccarelli, J. Noland WhiteJansen WongNo ratings yet
- Alters in Dissociative Identity Disorder (MPD) and DDNOSDocument14 pagesAlters in Dissociative Identity Disorder (MPD) and DDNOSSamanta Aryadevi TanNo ratings yet
- Norman Bates-Assessment and DiagnosisDocument16 pagesNorman Bates-Assessment and DiagnosisDiana-Luisa AvramNo ratings yet
- Judith Herman 1992 Complex - PTSDDocument15 pagesJudith Herman 1992 Complex - PTSDverlon100% (5)
- Dissociative Amnesia Case ReportDocument3 pagesDissociative Amnesia Case ReportJon MaciejewskiNo ratings yet
- Abnormal Psych Question 1Document10 pagesAbnormal Psych Question 1Ronald Jacob Picorro100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Reviewer in Ab PsychDocument8 pagesReviewer in Ab PsychMica MoradaNo ratings yet
- Unshackled - A Survivors Story of Mind ControlDocument467 pagesUnshackled - A Survivors Story of Mind ControlOpenEye100% (15)