You might also like
- Psychopathology in Adolescents and Adults with Autism Spectrum DisordersFrom EverandPsychopathology in Adolescents and Adults with Autism Spectrum DisordersRoberto KellerNo ratings yet
- Medications for autism spectrum disorder symptomsDocument2 pagesMedications for autism spectrum disorder symptomsMarissa AsimNo ratings yet
- Autism Revealed: All you Need to Know about Autism, Autistic Children and Adults, How to Manage Autism, and More!From EverandAutism Revealed: All you Need to Know about Autism, Autistic Children and Adults, How to Manage Autism, and More!No ratings yet
- Chapter 8 Childhood DisordersDocument6 pagesChapter 8 Childhood DisordersDessirie EnriquezNo ratings yet
- Autism Spectrum DisorderDocument22 pagesAutism Spectrum DisorderSABAHAT SHAHID BS Applied PsychologyNo ratings yet
- Concept MapDocument2 pagesConcept MapfaizaNo ratings yet
- Autism: Dr. Muhammad Mahbubur RahmanDocument28 pagesAutism: Dr. Muhammad Mahbubur RahmanMahbubur RahmanNo ratings yet
- Ttention Eficit Isorder: Definitions, Epidemiology, and PathophysiologyDocument15 pagesTtention Eficit Isorder: Definitions, Epidemiology, and Pathophysiologyzhe tempNo ratings yet
- ASDDocument9 pagesASDEmaan AtifNo ratings yet
- Dominica AutismDocument27 pagesDominica AutismAadeshMistryNo ratings yet
- Autism OverviewDocument29 pagesAutism Overviewah78 ab19No ratings yet
- Chapter 7 - Attention Deficit Disorder - 2018 - Integrative MedicineDocument15 pagesChapter 7 - Attention Deficit Disorder - 2018 - Integrative MedicineandreNo ratings yet
- Overcoming Autism Spectrum Disorder in children: Empowering Young Minds: A Holistic Approach to Navigating Autism Spectrum Disorder in ChildrenFrom EverandOvercoming Autism Spectrum Disorder in children: Empowering Young Minds: A Holistic Approach to Navigating Autism Spectrum Disorder in ChildrenNo ratings yet
- Neurodevelopmental DisordersDocument8 pagesNeurodevelopmental DisordersEunice CuñadaNo ratings yet
- Autismo 2003Document9 pagesAutismo 2003Victor EscobarNo ratings yet
- Research ProposalDocument17 pagesResearch Proposalmullamuskaan95No ratings yet
- Autism: Assessment and Management: Review ArticleDocument9 pagesAutism: Assessment and Management: Review ArticlemahamNo ratings yet
- Unlocking The Spectrum: Navigating The Complexity Of Autism With Advanced Strategies And InsightsFrom EverandUnlocking The Spectrum: Navigating The Complexity Of Autism With Advanced Strategies And InsightsNo ratings yet
- Developmental disorders in pediatrics: Global delay, autism, ADHD & moreDocument21 pagesDevelopmental disorders in pediatrics: Global delay, autism, ADHD & moreAnuj Pratap SinghNo ratings yet
- ALZHEIMERDocument2 pagesALZHEIMERLorelyn Santos CorpuzNo ratings yet
- Empowered Parenting: Practical Tips For Raising A Child With AutismFrom EverandEmpowered Parenting: Practical Tips For Raising A Child With AutismNo ratings yet
- Childhood Disorders GuideDocument18 pagesChildhood Disorders GuideDizon, Sharmaine L.No ratings yet
- Autism and Its Management in Pediatric Dentistry A ReviewDocument5 pagesAutism and Its Management in Pediatric Dentistry A Reviewstivensumual0701136055No ratings yet
- ASD, ADHD - Developmental Disorders in ChildrenDocument82 pagesASD, ADHD - Developmental Disorders in ChildrenOmar HamwiNo ratings yet
- Amaze Info Booklet 2017Document24 pagesAmaze Info Booklet 2017sugarycoffinNo ratings yet
- 2020 Art. Tratamiento AutismoDocument16 pages2020 Art. Tratamiento AutismoJohana AmayaNo ratings yet
- Unit-3 Autism Spectrum Disorder: Nature Needs and InterventionDocument81 pagesUnit-3 Autism Spectrum Disorder: Nature Needs and InterventionAlia SultanaNo ratings yet
- Medical Aspects of Autism Spectrum DisorderDocument12 pagesMedical Aspects of Autism Spectrum DisorderTimquannaNo ratings yet
- Alzheimer's Disease Nursing Care Plan & ManagementDocument6 pagesAlzheimer's Disease Nursing Care Plan & ManagementBryan NguyenNo ratings yet
- Clinical Features.: EPIDEMIOLOGY. The Prevalence Rate of All Pervasive DevelopmentalDocument10 pagesClinical Features.: EPIDEMIOLOGY. The Prevalence Rate of All Pervasive DevelopmentalWawan BwNo ratings yet
- UNIT 3 Study Guide NursingDocument12 pagesUNIT 3 Study Guide NursingkiinggdrewNo ratings yet
- Autism Spectrum DisorderDocument10 pagesAutism Spectrum Disordersobs sajadNo ratings yet
- Week 11 Ncm 109 Lecture PptxDocument49 pagesWeek 11 Ncm 109 Lecture PptxPolicarpio AprilNo ratings yet
- Sensory Processing Disorder vs. Autism UnderstanDocument2 pagesSensory Processing Disorder vs. Autism UnderstanlizamariNo ratings yet
- Neur OddsDocument102 pagesNeur Oddsalteahmae31No ratings yet
- Fs AutismDocument4 pagesFs AutismSuzana NikolovskaNo ratings yet
- (PEDIA) Developmental ConditionsDocument8 pages(PEDIA) Developmental ConditionsPAULINE VIVIEN ACLANNo ratings yet
- Pervasive Developmental DisordersDocument11 pagesPervasive Developmental Disordersapi-3797941No ratings yet
- Neurocognitve Developmet DisordersDocument53 pagesNeurocognitve Developmet DisordersMUZE TELANo ratings yet
- Decoding Love: Navigating Dating and Relationships on the Autism SpectrumFrom EverandDecoding Love: Navigating Dating and Relationships on the Autism SpectrumNo ratings yet
- What Is Autism?: 3.2. Autism and Idiot SavantsDocument5 pagesWhat Is Autism?: 3.2. Autism and Idiot SavantsAnonymous sSR6x6VC8aNo ratings yet
- SENSORY PROCESSING DISORDER: Understanding, Managing, and Thriving with Sensory Processing Challenges (2024 Beginner Guide)From EverandSENSORY PROCESSING DISORDER: Understanding, Managing, and Thriving with Sensory Processing Challenges (2024 Beginner Guide)No ratings yet
- Autism Is Characterized by Delays or Abnormal Functioning Before The Age of ThreeDocument7 pagesAutism Is Characterized by Delays or Abnormal Functioning Before The Age of ThreeCaracel Cabrera SobionoNo ratings yet
- AutismDocument26 pagesAutismminangsung minangnengNo ratings yet
- Artifact Intro and Ed IdDocument4 pagesArtifact Intro and Ed Idapi-253984664No ratings yet
- Autism PPTDocument55 pagesAutism PPTTadesse TedlaNo ratings yet
- File 1663148139 0005620 AUTISMDocument45 pagesFile 1663148139 0005620 AUTISM2022824838.pasangNo ratings yet
- Autism Spectrum Disorder: A guide with 10 key points to design the most suitable strategy for your childFrom EverandAutism Spectrum Disorder: A guide with 10 key points to design the most suitable strategy for your childNo ratings yet
- Autism B Theory: The Cause, Development and Support of AutismFrom EverandAutism B Theory: The Cause, Development and Support of AutismNo ratings yet
- Autism: Autism Diagnosis DSM IV MatchDocument6 pagesAutism: Autism Diagnosis DSM IV MatchReyhan VivaldyNo ratings yet
- Pervasive Developmental Disorders: Autisic DisorderDocument10 pagesPervasive Developmental Disorders: Autisic DisorderBinu MathewNo ratings yet
- Periodic Table of ElementsDocument1 pagePeriodic Table of ElementsRintuNo ratings yet
- Subjective Happiness ScaleDocument2 pagesSubjective Happiness ScaleRintuNo ratings yet
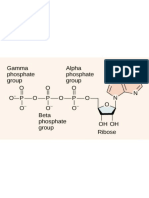
- Biological Macromolecules: Proteins, Nucleic Acids and LipidsDocument8 pagesBiological Macromolecules: Proteins, Nucleic Acids and LipidsRintuNo ratings yet
- Community Psychology - 1Document16 pagesCommunity Psychology - 1RintuNo ratings yet
- 0 0 0 o P-0-P-0-P-0 - : Gamma Alpha Phosphate Phosphate Group Group I II IDocument10 pages0 0 0 o P-0-P-0-P-0 - : Gamma Alpha Phosphate Phosphate Group Group I II IRintuNo ratings yet
- Psychology theories applied to workplace behaviorDocument6 pagesPsychology theories applied to workplace behaviorRintuNo ratings yet
- Counseling PsychologyDocument25 pagesCounseling PsychologyRintuNo ratings yet
- Myers Treatment of Abnormal Behavior NotesDocument9 pagesMyers Treatment of Abnormal Behavior NotesRintuNo ratings yet
- Nization and Behavior Afects The Organization's PerformanceDocument1 pageNization and Behavior Afects The Organization's PerformanceRintuNo ratings yet
- Early Management Approaches and TheoriesDocument10 pagesEarly Management Approaches and TheoriesRintuNo ratings yet
- Organizational behavior insights for managing through changeDocument9 pagesOrganizational behavior insights for managing through changeRintuNo ratings yet
- Conversion & Dissociative Identity DisordersDocument2 pagesConversion & Dissociative Identity DisordersRintu100% (1)
- Social Influence On BehaviorDocument4 pagesSocial Influence On BehaviorRintuNo ratings yet
- Classification in DSM-5Document7 pagesClassification in DSM-5RintuNo ratings yet
- Messer, S. - Behavioral and Psychoanalytic Perspectives at Therapeutic Choice PointsDocument12 pagesMesser, S. - Behavioral and Psychoanalytic Perspectives at Therapeutic Choice PointsFrancisca Monsalve C.No ratings yet
- Background Info.Document3 pagesBackground Info.Moses V. GonzalesNo ratings yet
- Eric BerneDocument5 pagesEric BerneJohn Sebastian CumpstonNo ratings yet
- Volkert Et Al - 2018Document7 pagesVolkert Et Al - 2018dallaNo ratings yet
- Adult ADHD Screening Checklist GuideDocument3 pagesAdult ADHD Screening Checklist GuideFAKESIGNUPACCOUNTNo ratings yet
- Activity 7, NSTPDocument3 pagesActivity 7, NSTPZam-zamNo ratings yet
- Alfano, Ginsburg, & Kingery (2007) SleepDocument9 pagesAlfano, Ginsburg, & Kingery (2007) SleepJanuaryska SaraswatiNo ratings yet
- Stuttering and HomeopathyDocument2 pagesStuttering and Homeopathyosso_lesNo ratings yet
- David Rosenhan's Study ExperimentDocument8 pagesDavid Rosenhan's Study Experimenttala el haririNo ratings yet
- Thesis Statement For Bipolar Disorder Research PaperDocument7 pagesThesis Statement For Bipolar Disorder Research Paperfvja66n5No ratings yet
- A Psychoanalytic Reading of The Works of Paulo CoheloDocument5 pagesA Psychoanalytic Reading of The Works of Paulo Coheloanishkrishnannayar100% (1)
- Ess 7Document4 pagesEss 7api-582020074No ratings yet
- Psychotic WebDocument49 pagesPsychotic WebPrerogative GreenNo ratings yet
- Brief Evaluation of Executive DysfunctionDocument2 pagesBrief Evaluation of Executive DysfunctionIon Arrieta ValeroNo ratings yet
- Amets ZurutuzaDocument3 pagesAmets ZurutuzaMaitane ArrietaNo ratings yet
- Freud's concept of mourningDocument4 pagesFreud's concept of mourningbooksarefunNo ratings yet
- Practical Research 1 Group 6 1Document18 pagesPractical Research 1 Group 6 1Danielle EvangelistaNo ratings yet
- Applied Social Science HandoutsDocument6 pagesApplied Social Science HandoutsQuinn AvrilNo ratings yet
- Introduction To The Case of StanDocument6 pagesIntroduction To The Case of StanApple Esmenos100% (2)
- AnxietyDocument3 pagesAnxietyStephen MillsNo ratings yet
- Biblio Engl From 2000Document95 pagesBiblio Engl From 2000degetica5No ratings yet
- Assignment 3Document5 pagesAssignment 3bettyboop1312100% (1)
- Techniques For Disputing Irrational BeliefsDocument3 pagesTechniques For Disputing Irrational Beliefshappylifesancheti@No ratings yet
- National Mental Health Programme, IndiaDocument27 pagesNational Mental Health Programme, Indiadrguptavivek1978No ratings yet
- Ganser Syndrome: A Case Report From ThailandDocument4 pagesGanser Syndrome: A Case Report From ThailandYuyun Ayu ApriyantiNo ratings yet
- Mental Illness The Care 1Document4 pagesMental Illness The Care 1api-241658113No ratings yet
- Test Bank For Psychiatric and Mental Health Nursing For Canadian Practice 2nd Edition AustinDocument7 pagesTest Bank For Psychiatric and Mental Health Nursing For Canadian Practice 2nd Edition AustinBilly Riddle100% (29)
- Popis LiteratureDocument3 pagesPopis LiteraturesuyijaaNo ratings yet
- Ies RDocument3 pagesIes RIvana OzzNo ratings yet
- Dihs-SlrcpDocument48 pagesDihs-SlrcpOLGA SORIANONo ratings yet