You might also like
- Self Help CBT Cognitive Behavior Therapy Training Course & Toolbox: Cognitive Behavioral Therapy Book for Anger Management, Depression, Social Anxiety, OCD, Sleep Disorders, Addictions, Fears & moreFrom EverandSelf Help CBT Cognitive Behavior Therapy Training Course & Toolbox: Cognitive Behavioral Therapy Book for Anger Management, Depression, Social Anxiety, OCD, Sleep Disorders, Addictions, Fears & moreRating: 3 out of 5 stars3/5 (1)
- The Mindbody Workbook - Mar 2013Document7 pagesThe Mindbody Workbook - Mar 2013paul lukawski100% (6)
- Neuroticism: Volatility & Withdrawal: Lecture Notes 4Document7 pagesNeuroticism: Volatility & Withdrawal: Lecture Notes 4Danilo PesicNo ratings yet
- Color Atlas of Emergency TraumaDocument314 pagesColor Atlas of Emergency TraumaIacob Razvan75% (8)
- Cognitive TheoryDocument14 pagesCognitive TheoryRiya Joy100% (4)
- HESI Study Guide Psychiatric NursingDocument26 pagesHESI Study Guide Psychiatric NursingDean Winchester100% (4)
- 31 Hypnosis TechniquesDocument13 pages31 Hypnosis TechniquesJohannes Williem100% (2)
- James S. Grotstein - But at The Same Time and On Another Level... - Volume 2, Clinical Applications in The Kleinian - Bionian Mode-Karnac Books (2009)Document305 pagesJames S. Grotstein - But at The Same Time and On Another Level... - Volume 2, Clinical Applications in The Kleinian - Bionian Mode-Karnac Books (2009)Paul FengNo ratings yet
- Psychology Test 3 NotesDocument14 pagesPsychology Test 3 NotesAndrew HoffNo ratings yet
- Psychology Slides Section EDocument50 pagesPsychology Slides Section ERao ZeeshanNo ratings yet
- Psychoanalysis TheoryDocument10 pagesPsychoanalysis TheoryRico mwaiNo ratings yet
- Managerial Counselling Module IIDocument50 pagesManagerial Counselling Module IIPrerana AroraNo ratings yet
- General Psyc-All in One-2013Document237 pagesGeneral Psyc-All in One-2013Galoo LagesseNo ratings yet
- Chapter 13 Treatment of Psychological DisordersDocument4 pagesChapter 13 Treatment of Psychological DisordersAfiya KhanNo ratings yet
- Psychoanalytic Paradigm and Sigmund Freud's ViewsDocument37 pagesPsychoanalytic Paradigm and Sigmund Freud's Viewsmay angNo ratings yet
- Lecture 3 - Therapy and TreatmentDocument61 pagesLecture 3 - Therapy and TreatmentUkraineNo ratings yet
- PerspectivesDocument50 pagesPerspectivesDeanne YsabelleNo ratings yet
- Lesson 4Document3 pagesLesson 4Jayson PalisocNo ratings yet
- HYPNOSIS AND HYPNOTHERAPY: A PRACTICAL GUIDEDocument142 pagesHYPNOSIS AND HYPNOTHERAPY: A PRACTICAL GUIDETeodora-Aurora Brebenaru100% (1)
- Comparative Analysis SOC SCIDocument15 pagesComparative Analysis SOC SCIiccdolotallas.csrlNo ratings yet
- U1 Class Note OutlinesDocument13 pagesU1 Class Note OutlinesTiffany AustinNo ratings yet
- Stress Management For Life A Research Based Experiential Approach 4Th Edition Olpin Solutions Manual Full Chapter PDFDocument51 pagesStress Management For Life A Research Based Experiential Approach 4Th Edition Olpin Solutions Manual Full Chapter PDFleonardedanah7lkhe100% (6)
- NCERT Solutions For Class 11 Psychology Chapter 1: WWW - Ncrtsolutions.inDocument4 pagesNCERT Solutions For Class 11 Psychology Chapter 1: WWW - Ncrtsolutions.inchetnaNo ratings yet
- NCERT Solutions For Class 11 Psychology Chapter 1Document4 pagesNCERT Solutions For Class 11 Psychology Chapter 1Shah FaisalNo ratings yet
- Disciplines and Ideas in The Social Sciences: Perceived Human Personality and Rationality Towards SolidDocument23 pagesDisciplines and Ideas in The Social Sciences: Perceived Human Personality and Rationality Towards SolidArjane Grace SullanoNo ratings yet
- Psycho-analysis and Analytical TheoryDocument10 pagesPsycho-analysis and Analytical TheoryEverything newNo ratings yet
- DISS Module Week 8Document11 pagesDISS Module Week 8Airene NopalNo ratings yet
- Chapter17therapy 150214191420 Conversion Gate01Document66 pagesChapter17therapy 150214191420 Conversion Gate01John Carlo Fariñas SuyuNo ratings yet
- 8704182982Document7 pages8704182982Juliah ShchekleinaNo ratings yet
- Behaviours in HypnosisDocument3 pagesBehaviours in HypnosismichelleanousNo ratings yet
- Psychiatric and Psychological Theories - Sir NicoDocument35 pagesPsychiatric and Psychological Theories - Sir NicoNico PelomianoNo ratings yet
- Psychological Perspectives of the SelfDocument9 pagesPsychological Perspectives of the SelfKimberly Pascua ArizNo ratings yet
- HED 487 - Defense Mechanisms Such As DID As A Result of Child AbuseDocument9 pagesHED 487 - Defense Mechanisms Such As DID As A Result of Child AbuseMadelyn O'ConnellNo ratings yet
- Psychoanalytic TherapyDocument6 pagesPsychoanalytic TherapyPrincessCapitalNo ratings yet
- MPCE 023 All BlockDocument229 pagesMPCE 023 All BlockMohit DabasNo ratings yet
- Mpce 023 Block 1Document67 pagesMpce 023 Block 1Mohit DabasNo ratings yet
- Psychology: An Overview: Chapter ObjectivesDocument94 pagesPsychology: An Overview: Chapter ObjectivesMing MingNo ratings yet
- Demophobia: Causes, Symptoms and Methods of Crowd Fear CureDocument16 pagesDemophobia: Causes, Symptoms and Methods of Crowd Fear CureSCrIbdNo ratings yet
- PsychotherapieDocument11 pagesPsychotherapieIvana PisanoNo ratings yet
- 15 PsychiatricDocument35 pages15 PsychiatricSami Ullah Khan NiaziNo ratings yet
- Abnormal PsychologyWEEKLY NOTESDocument73 pagesAbnormal PsychologyWEEKLY NOTESMelanie WaltersNo ratings yet
- Assignment of Clinical PsychologyDocument26 pagesAssignment of Clinical PsychologyPramjeet SinghNo ratings yet
- Psychiatric Nursing: Presented By:kevinDocument37 pagesPsychiatric Nursing: Presented By:kevinKevin RaiyaniNo ratings yet
- Michael Macasaet Personality Punishment Defense MechanismsDocument4 pagesMichael Macasaet Personality Punishment Defense MechanismsKevin MacasaetNo ratings yet
- Cuestionario Contestado de InglesDocument10 pagesCuestionario Contestado de InglesJesus Arturo Ramirez OchoaNo ratings yet
- Lesson 1 Fundamental Concepts in Ethics Part 2Document60 pagesLesson 1 Fundamental Concepts in Ethics Part 2DACANAY, SHAMER D.No ratings yet
- Theories of PersonalityDocument89 pagesTheories of PersonalityLance Fuentes100% (6)
- HALUSINATIONDocument10 pagesHALUSINATIONdwiNo ratings yet
- CBT Insight: Origins and TechniquesDocument2 pagesCBT Insight: Origins and TechniquesShreya VermaNo ratings yet
- Chapter 4Document3 pagesChapter 4YZEL ALFECHENo ratings yet
- Uncover Repressed Thoughts with PsychoanalysisDocument7 pagesUncover Repressed Thoughts with PsychoanalysispamNo ratings yet
- Neuroticism: Volatility & Withdrawal: Lecture Notes 4Document7 pagesNeuroticism: Volatility & Withdrawal: Lecture Notes 4Danilo PesicNo ratings yet
- Defense Mechanism, Psychological Perspective and Fields of PsychologyDocument46 pagesDefense Mechanism, Psychological Perspective and Fields of PsychologyVince Dulay100% (1)
- Defense Mechanism, Psychological Perspective and Fields of PsychologyDocument46 pagesDefense Mechanism, Psychological Perspective and Fields of PsychologyVince DulayNo ratings yet
- Psychology QuizDocument14 pagesPsychology QuizsasisimhadriiiNo ratings yet
- Week 2Document54 pagesWeek 2MAHALI DUMAGSANo ratings yet
- Psychotherapeutic Traditions HandoutDocument5 pagesPsychotherapeutic Traditions HandoutTina Malabanan CobarrubiasNo ratings yet
- Insight TherapiesDocument17 pagesInsight Therapiesapi-287575009No ratings yet
- C5 - Glen O. Gabbard - Long-Term Psychodynamic Psychotherapy - A Basic Text (Core Competencies in Psychotherapy) (2004) Páginas 1 - 40Document40 pagesC5 - Glen O. Gabbard - Long-Term Psychodynamic Psychotherapy - A Basic Text (Core Competencies in Psychotherapy) (2004) Páginas 1 - 40JOAN LEWINNo ratings yet
- Bruce Bonnett Forming SuggestionsDocument27 pagesBruce Bonnett Forming SuggestionsRajesh S VNo ratings yet
- Chapter 1 Psych NotesDocument13 pagesChapter 1 Psych Notesjovilla100% (1)
- The Defence MechanismsDocument12 pagesThe Defence MechanismsShikhar Dhawan FoundationNo ratings yet
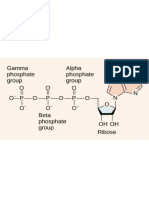
- 0 0 0 o P-0-P-0-P-0 - : Gamma Alpha Phosphate Phosphate Group Group I II IDocument10 pages0 0 0 o P-0-P-0-P-0 - : Gamma Alpha Phosphate Phosphate Group Group I II IRintuNo ratings yet
- Subjective Happiness ScaleDocument2 pagesSubjective Happiness ScaleRintuNo ratings yet
- Periodic Table of ElementsDocument1 pagePeriodic Table of ElementsRintuNo ratings yet
- Biological Macromolecules: Proteins, Nucleic Acids and LipidsDocument8 pagesBiological Macromolecules: Proteins, Nucleic Acids and LipidsRintuNo ratings yet
- Community Psychology - 1Document16 pagesCommunity Psychology - 1RintuNo ratings yet
- Psychology theories applied to workplace behaviorDocument6 pagesPsychology theories applied to workplace behaviorRintuNo ratings yet
- Counseling PsychologyDocument25 pagesCounseling PsychologyRintuNo ratings yet
- Early Management Approaches and TheoriesDocument10 pagesEarly Management Approaches and TheoriesRintuNo ratings yet
- Organizational behavior insights for managing through changeDocument9 pagesOrganizational behavior insights for managing through changeRintuNo ratings yet
- Social Influence On BehaviorDocument4 pagesSocial Influence On BehaviorRintuNo ratings yet
- Nization and Behavior Afects The Organization's PerformanceDocument1 pageNization and Behavior Afects The Organization's PerformanceRintuNo ratings yet
- Classification in DSM-5Document7 pagesClassification in DSM-5RintuNo ratings yet
- Developmental DisordersDocument6 pagesDevelopmental DisordersRintuNo ratings yet
- Conversion & Dissociative Identity DisordersDocument2 pagesConversion & Dissociative Identity DisordersRintu100% (1)
- Nikolas Rose - Neurochemical SelvesDocument15 pagesNikolas Rose - Neurochemical Selveslc49No ratings yet
- Conduct Disorder Diagnosis and Treatment in Primar PDFDocument11 pagesConduct Disorder Diagnosis and Treatment in Primar PDFhopeIshanzaNo ratings yet
- Constructing Therapeutic Metaphors and Stories: Betty Alice Erickson, M.S., L.P.C., L.M.F.TDocument6 pagesConstructing Therapeutic Metaphors and Stories: Betty Alice Erickson, M.S., L.P.C., L.M.F.TRajesh100% (1)
- Amniotic Fluid EmbolismDocument19 pagesAmniotic Fluid EmbolismStar Alvarez100% (1)
- Annotated BibliographyDocument6 pagesAnnotated Bibliographyapi-316369815No ratings yet
- Мелкоклеточная карциномаDocument250 pagesМелкоклеточная карциномаBertramVrellingNo ratings yet
- Bag Technique-BenedictDocument6 pagesBag Technique-BenedictAriel Delos ReyesNo ratings yet
- Randomized Control Trial To Real World Evidence of Ultra Long Acting Insulin Basal Glargine-300: What Big Clinical Data Teaching Us ?Document27 pagesRandomized Control Trial To Real World Evidence of Ultra Long Acting Insulin Basal Glargine-300: What Big Clinical Data Teaching Us ?Yaumil FitriNo ratings yet
- Complete Brain RechargeDocument4 pagesComplete Brain RechargeNourish and Revive Holistic Health and NutritionNo ratings yet
- MIS 310 ProjectDocument8 pagesMIS 310 Projectumma marzinaNo ratings yet
- HELLP Syndrome: Guide to the Rare Pregnancy ComplicationDocument2 pagesHELLP Syndrome: Guide to the Rare Pregnancy ComplicationAnonymous EA9uILwJ08No ratings yet
- Mechanism of Action, Indications, Administration and Side Effects of RisperidoneDocument2 pagesMechanism of Action, Indications, Administration and Side Effects of RisperidoneLanzen DragneelNo ratings yet
- MCQ Sample QuestionsDocument4 pagesMCQ Sample QuestionsNaveen Vachipalli100% (1)
- Key Partners Key Activities Value Propositions Customer Relationships Customer SegmentsDocument2 pagesKey Partners Key Activities Value Propositions Customer Relationships Customer SegmentsheiseiNo ratings yet
- Hygiene and Sanitary Practices in The Fruit JuiceDocument19 pagesHygiene and Sanitary Practices in The Fruit JuiceJoyce Marian BelonguelNo ratings yet
- Theory and Practice of Counseling and Psychotherapy 9th Edition Corey Test BankDocument13 pagesTheory and Practice of Counseling and Psychotherapy 9th Edition Corey Test BankGregoryGreenroyak100% (12)
- Comfort Room PDFDocument1 pageComfort Room PDFPixaaaNo ratings yet
- 4.1 Drug Related MortalityDocument3 pages4.1 Drug Related Mortalityvalery HERMOZANo ratings yet
- Kajian Teknis IncenDocument9 pagesKajian Teknis Incenagun bebenNo ratings yet
- Jejunostomy FeedingDocument13 pagesJejunostomy FeedingAdith Fileanugraha40% (5)
- Osteoplastic Reconstruction of Severely Resorbed Maxilla by Stack Plasty: Combining Sinus Augmentation With Lateral and Vertical Onlay Bone GraftingDocument5 pagesOsteoplastic Reconstruction of Severely Resorbed Maxilla by Stack Plasty: Combining Sinus Augmentation With Lateral and Vertical Onlay Bone GraftingAnonymous Qt31LLO1lNo ratings yet
- Feline Diabetes Mellitus-Nutritional StrategiesDocument42 pagesFeline Diabetes Mellitus-Nutritional StrategiesAsghar ShahNo ratings yet
- Hospital Licensing Rules CH 133Document334 pagesHospital Licensing Rules CH 133Ytamar Visbal PerezNo ratings yet
- Department of AYUSH: (Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy)Document3 pagesDepartment of AYUSH: (Ayurveda, Yoga and Naturopathy, Unani, Siddha and Homoeopathy)Sreedhar TirunagariNo ratings yet
- NCLEX Sample Questions For Psychiatric Nursing 2: JUNE 23, 2009 BYDocument8 pagesNCLEX Sample Questions For Psychiatric Nursing 2: JUNE 23, 2009 BYbabykhoNo ratings yet
- Genetic Engineering: Genetic Engineering Is Defined As The Deliberate Modification of Genes in Order To AlterDocument4 pagesGenetic Engineering: Genetic Engineering Is Defined As The Deliberate Modification of Genes in Order To AlterChris Cgc PettingaNo ratings yet
- An Adhd Epidemic and Other Misdiagnosed Mental Illnesses in Children Final ReportDocument108 pagesAn Adhd Epidemic and Other Misdiagnosed Mental Illnesses in Children Final Reportapi-350787181100% (1)
- Ibogaine Treatment Outcomes For Opioid DependenceDocument11 pagesIbogaine Treatment Outcomes For Opioid DependenceAkbar ShakoorNo ratings yet