You might also like
- Patho 1 2Document5 pagesPatho 1 2KATHLEEN JOSOLNo ratings yet
- Pa Tho PhysiologyDocument3 pagesPa Tho PhysiologyMike GarciaNo ratings yet
- IV PathophysiologyDocument5 pagesIV PathophysiologyJanedear Pasal100% (1)
- Urolithiasis / Renal Calculi: Clinical Manifestation: Stones in The Renal PelvisDocument3 pagesUrolithiasis / Renal Calculi: Clinical Manifestation: Stones in The Renal PelvisErika ArceoNo ratings yet
- EngDiv Renal Pathophysiol 2023Document97 pagesEngDiv Renal Pathophysiol 2023Luis RomanosNo ratings yet
- 313 - Disorders of Renal and Urinary SystemsDocument8 pages313 - Disorders of Renal and Urinary SystemsChrissy Mendoza100% (2)
- Pathophysiology of NephrolithiasisDocument2 pagesPathophysiology of Nephrolithiasisanreilegarde80% (5)
- UrolithiasisDocument99 pagesUrolithiasisgeorgejobinputhenpurackalNo ratings yet
- Pathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsDocument4 pagesPathophysiology: Cholecystitis Non Modifiable Factors Modifiable FactorsLovely DaroleNo ratings yet
- Urine Physical Sediment1819Document23 pagesUrine Physical Sediment1819Anas ShwbkNo ratings yet
- Fdar For UtiDocument2 pagesFdar For UtiCARL ANGEL JAOCHICONo ratings yet
- Cholelithiasis CholecystitisDocument1 pageCholelithiasis Cholecystitissamliebareng77No ratings yet
- NUR 3032 Pancreatic, Biliary, and Hepatic Disorders Study PlanDocument6 pagesNUR 3032 Pancreatic, Biliary, and Hepatic Disorders Study PlanThalia FortuneNo ratings yet
- Diseases of Urinary SystemDocument39 pagesDiseases of Urinary SystemRupak PandeyNo ratings yet
- Obstruksi Uropati IrfanDocument43 pagesObstruksi Uropati IrfanirfanNo ratings yet
- Pathophysiology-Kni Ns PLZZZDocument8 pagesPathophysiology-Kni Ns PLZZZAnna Lira Manluyang MungcalNo ratings yet
- Pa Tho Physiology of Acute GastroentertisDocument1 pagePa Tho Physiology of Acute GastroentertisHassan Bj MarabongNo ratings yet
- 2106 UtiDocument2 pages2106 UtishimiNo ratings yet
- Pathophysiology CholelithiasisDocument2 pagesPathophysiology CholelithiasisLovely DaroleNo ratings yet
- Cholelithiasis: Shoofii Dzakiyyah Ulhaq Preceptor: Dr. Liza Nursanty, SP.B, M.Kes, FinacsDocument40 pagesCholelithiasis: Shoofii Dzakiyyah Ulhaq Preceptor: Dr. Liza Nursanty, SP.B, M.Kes, FinacsShofiDzakiyahUlhaqNo ratings yet
- Renal DisordersDocument60 pagesRenal DisordersENJELAH RAIKA NEYRANo ratings yet
- Pathophysiology of Nephrolithiasis, Struvites Stone (Staghorn Calculi)Document2 pagesPathophysiology of Nephrolithiasis, Struvites Stone (Staghorn Calculi)Floyd100% (2)
- Pharmacology: Drug Therapy of GoutDocument81 pagesPharmacology: Drug Therapy of GoutYousef JafarNo ratings yet
- Disorders of GallbladderDocument65 pagesDisorders of Gallbladdernuguitnorelyn30No ratings yet
- Gout 131015051453 Phpapp01 PDFDocument26 pagesGout 131015051453 Phpapp01 PDFReny Rony BersaudaraNo ratings yet
- Ms Reviewer Renal UrinaryDocument5 pagesMs Reviewer Renal UrinaryAlyssa Nicole CajayonNo ratings yet
- Urinary Tract StoneDocument17 pagesUrinary Tract StoneWilko WilliamNo ratings yet
- Pathophysiology CholeDocument3 pagesPathophysiology CholeClyde AleczandreNo ratings yet
- Abnormal UrineDocument28 pagesAbnormal UrinemujeebNo ratings yet
- Gastrointestinal OsmosisDocument174 pagesGastrointestinal OsmosisfabicontrerasenarmNo ratings yet
- Benign Prostatic Hyperplasia Concept MapDocument1 pageBenign Prostatic Hyperplasia Concept MapSarah RonquilloNo ratings yet
- Pendekatan Dan Diagnosis DispepsiaDocument16 pagesPendekatan Dan Diagnosis DispepsiaJual Beli PromosiNo ratings yet
- FINALPATHOADENOCARCINOMADocument1 pageFINALPATHOADENOCARCINOMAjahtolentinoNo ratings yet
- PATHOPHYSIOLOGYofDocument3 pagesPATHOPHYSIOLOGYofRose Si CheeksNo ratings yet
- Physical Examination and Health Assessment: Genitourinary SystemDocument134 pagesPhysical Examination and Health Assessment: Genitourinary Systemmesfin DemiseNo ratings yet
- Benign Prostatic Hyperplasia Is A BenignDocument4 pagesBenign Prostatic Hyperplasia Is A BenignZeinab SrourNo ratings yet
- Cholelithiasis PathophysiologyDocument2 pagesCholelithiasis PathophysiologyShinrin SukehiroNo ratings yet
- Benign Prostatic HyperplasiaDocument5 pagesBenign Prostatic Hyperplasiatabangin_hilario100% (1)
- 10 - Urological DiordersDocument47 pages10 - Urological Diordersgozali189 biringNo ratings yet
- Concept Map Liver CirrhosisssDocument2 pagesConcept Map Liver CirrhosisssAsniah Hadjiadatu Abdullah92% (12)
- Cholelithiasis - Knowledge at AMBOSSDocument1 pageCholelithiasis - Knowledge at AMBOSSManar AlahmadiNo ratings yet
- Chronic Inflammation of The Gallbladder Eventually The Bile DuctDocument2 pagesChronic Inflammation of The Gallbladder Eventually The Bile DuctYeshaa MiraniNo ratings yet
- 3.1.3.2 Batu Saluran KemihDocument64 pages3.1.3.2 Batu Saluran Kemihwinda musliraNo ratings yet
- Cholecystitis Pathophysiology Schematic DiagramDocument2 pagesCholecystitis Pathophysiology Schematic DiagramChristyl CalizoNo ratings yet
- Uro Spots SummaryDocument25 pagesUro Spots Summarynthabiseng maboganaNo ratings yet
- CirrhosisDocument55 pagesCirrhosisFUTURE DOCTORNo ratings yet
- ISK Komplek: Infeksi Saluran KemihDocument51 pagesISK Komplek: Infeksi Saluran Kemihtriska antonyNo ratings yet
- UrologyDocument36 pagesUrologyakufahaba100% (2)
- Submitted To:-Presented By:-: Miss Avneet Madam DMC&H Navkiranjot Kaur B.Sc. (N) Iind Year Roll No - 102Document59 pagesSubmitted To:-Presented By:-: Miss Avneet Madam DMC&H Navkiranjot Kaur B.Sc. (N) Iind Year Roll No - 102Harpal Singh HansNo ratings yet
- Stones GuidelinesDocument5 pagesStones GuidelinesRaza MughalNo ratings yet
- 5.9.8. Lecture Urinary Syndromes GM 2020Document93 pages5.9.8. Lecture Urinary Syndromes GM 2020Natalie AlcântaraNo ratings yet
- Acute Renal Failure SymptomsDocument10 pagesAcute Renal Failure SymptomsEdwin Delos Reyes AbuNo ratings yet
- VI. Patho-Physiology: Removal of The Gallbladder?Document3 pagesVI. Patho-Physiology: Removal of The Gallbladder?Maui ReyesNo ratings yet
- Benign Prostatic Hyperplasia (BPH)Document26 pagesBenign Prostatic Hyperplasia (BPH)DR-Somalaraju Sateesh Kumar RajuNo ratings yet
- The Perfect Pancreatitis Diet Cookbook; The Complete Nutrition Guide To Managing And Healing Pancreatitis With Delectable And Nourishing Recipes;From EverandThe Perfect Pancreatitis Diet Cookbook; The Complete Nutrition Guide To Managing And Healing Pancreatitis With Delectable And Nourishing Recipes;No ratings yet
- The Perfect Kidney Stone Diet Cookbook:The Complete Nutrition Guide To Treating And Managing Kidney Problem With Delectable And Nourishing RecipesFrom EverandThe Perfect Kidney Stone Diet Cookbook:The Complete Nutrition Guide To Treating And Managing Kidney Problem With Delectable And Nourishing RecipesNo ratings yet
- Hematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesFrom EverandHematuria, (Blood in Urine) A Simple Guide to The Condition, Related Diseases And Use in Diagnosis of DiseasesRating: 5 out of 5 stars5/5 (2)
- Stoma CareFrom EverandStoma CareJennie BurchNo ratings yet
- The Ideal Acute Pancreatitis Diet Cookbook; The Superb Diet Guide To Manage And Treat Pancreatitis And Reduce Inflammation With Nutritious RecipesFrom EverandThe Ideal Acute Pancreatitis Diet Cookbook; The Superb Diet Guide To Manage And Treat Pancreatitis And Reduce Inflammation With Nutritious RecipesNo ratings yet
- Josol Disaster Nursing RolesDocument1 pageJosol Disaster Nursing RolesKATHLEEN JOSOLNo ratings yet
- The Casualties in The Caraga Region. (2 PTS)Document2 pagesThe Casualties in The Caraga Region. (2 PTS)KATHLEEN JOSOLNo ratings yet
- Pabulario CASEDocument1 pagePabulario CASEKATHLEEN JOSOLNo ratings yet
- Flood Events in The PhilippinesDocument2 pagesFlood Events in The PhilippinesKATHLEEN JOSOLNo ratings yet
- DisasterNursing SemifinalsDocument2 pagesDisasterNursing SemifinalsKATHLEEN JOSOLNo ratings yet
- Ivf ProcedureDocument4 pagesIvf ProcedureKATHLEEN JOSOLNo ratings yet
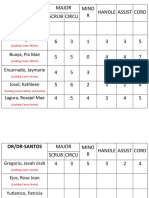
- Or/Dr-Bmc: Major Mino R Handle Assist Cord Scrub CircuDocument3 pagesOr/Dr-Bmc: Major Mino R Handle Assist Cord Scrub CircuKATHLEEN JOSOLNo ratings yet
- Self-Introduction Letter (JOSOL)Document1 pageSelf-Introduction Letter (JOSOL)KATHLEEN JOSOLNo ratings yet
- Portfolio IN Science: Father Urios Academy of Magallanes IncDocument8 pagesPortfolio IN Science: Father Urios Academy of Magallanes IncKATHLEEN JOSOLNo ratings yet
- Ics UreterolithiasisDocument10 pagesIcs UreterolithiasisKATHLEEN JOSOLNo ratings yet
- PRELIM - SESSION 1 - Historical Antecedent of Science and TechnologyDocument51 pagesPRELIM - SESSION 1 - Historical Antecedent of Science and TechnologyKATHLEEN JOSOLNo ratings yet
- Self-Introduction Letter (JOSOL)Document1 pageSelf-Introduction Letter (JOSOL)KATHLEEN JOSOLNo ratings yet
- Junve ReportDocument1 pageJunve ReportKATHLEEN JOSOLNo ratings yet
- Nanay Lily BiographyDocument2 pagesNanay Lily BiographyKATHLEEN JOSOLNo ratings yet
- Referral Letter EduardoDocument1 pageReferral Letter EduardoKATHLEEN JOSOLNo ratings yet
- Final Requirement (FINAL EXAM)Document4 pagesFinal Requirement (FINAL EXAM)KATHLEEN JOSOLNo ratings yet
- Mga Tala NG Aking BuhayDocument1 pageMga Tala NG Aking BuhayKATHLEEN JOSOLNo ratings yet
- Compare and Contrast (Group-3)Document4 pagesCompare and Contrast (Group-3)KATHLEEN JOSOLNo ratings yet
- Ge 107 Topic OutlineDocument2 pagesGe 107 Topic OutlineKATHLEEN JOSOLNo ratings yet
- FSUU Parents Consent New NormalDocument1 pageFSUU Parents Consent New NormalKATHLEEN JOSOLNo ratings yet
- Butuan or Limasawa:: The Site of The First Mass in The PhilippinesDocument31 pagesButuan or Limasawa:: The Site of The First Mass in The PhilippinesJomar ColumbaNo ratings yet
- Final RequirementDocument2 pagesFinal RequirementKATHLEEN JOSOLNo ratings yet
- Laudato SiDocument3 pagesLaudato SiKATHLEEN JOSOLNo ratings yet
- Reflection On Laudato SiDocument1 pageReflection On Laudato SiKATHLEEN JOSOLNo ratings yet
- Duties of The FamilyDocument15 pagesDuties of The FamilyKATHLEEN JOSOLNo ratings yet
- Act On Primary Vs SecondaryDocument1 pageAct On Primary Vs SecondaryFlorence LapinigNo ratings yet
- Final Requirement (FINAL EXAM)Document4 pagesFinal Requirement (FINAL EXAM)KATHLEEN JOSOLNo ratings yet
- DocxDocument12 pagesDocxKATHLEEN JOSOLNo ratings yet
- iSF EClassRecord - NewNormal AdviserDocument254 pagesiSF EClassRecord - NewNormal AdviserYanara Delarama DayapNo ratings yet
- Labor To DigestDocument32 pagesLabor To Digestphoenix rogueNo ratings yet
- Substation Off Line and Hot Line CommissioningDocument3 pagesSubstation Off Line and Hot Line CommissioningMohammad JawadNo ratings yet
- Community-Based Disaster Risk Reduction and Management Plan: Poblacion Sur, Carmen, BoholDocument6 pagesCommunity-Based Disaster Risk Reduction and Management Plan: Poblacion Sur, Carmen, BoholMarah RabinaNo ratings yet
- Tutorial SessionDocument5 pagesTutorial SessionKhánh LinhNo ratings yet
- Final Report On WaterproofingDocument35 pagesFinal Report On WaterproofingAlOk100% (2)
- Paper 4 Nov 2000Document2 pagesPaper 4 Nov 2000MSHNo ratings yet
- Grandma StoriesDocument38 pagesGrandma StoriesSita Rani Devi DasiNo ratings yet
- QTR-2 2023 Meeting Format Nov.23Document45 pagesQTR-2 2023 Meeting Format Nov.23skumar31397No ratings yet
- Logiq e BT11 User Guide PDFDocument192 pagesLogiq e BT11 User Guide PDFprofesorbartolomeo0% (1)
- Project PPT Spot WeldingDocument19 pagesProject PPT Spot WeldingMehul BariyaNo ratings yet
- Zinc Silicate or Zinc Epoxy As The Preferred High Performance PrimerDocument10 pagesZinc Silicate or Zinc Epoxy As The Preferred High Performance Primerbabis1980100% (1)
- Grade 12 - Biology Resource BookDocument245 pagesGrade 12 - Biology Resource BookMali100% (6)
- Social Science Assignment Class 8 CBSEDocument3 pagesSocial Science Assignment Class 8 CBSEgurdeepsarora8738No ratings yet
- New Approaches To Cryopreservation of Cells, Tissues, and OrgansDocument19 pagesNew Approaches To Cryopreservation of Cells, Tissues, and OrgansLaura CursaruNo ratings yet
- First Communion: You Are The VoiceDocument10 pagesFirst Communion: You Are The VoiceErnesto Albeus Villarete Jr.No ratings yet
- Evolve Reach - Powered by HESIDocument7 pagesEvolve Reach - Powered by HESIangelsarerare14% (7)
- Kyocera Fs 1118mfpKm1820Document200 pagesKyocera Fs 1118mfpKm1820Jane VinuyaNo ratings yet
- Science Quarter 1 Lesson 10 Day 1Document20 pagesScience Quarter 1 Lesson 10 Day 1Lizbeth Edralinda-martinezNo ratings yet
- IR Beam LaunchingDocument2 pagesIR Beam LaunchingalfredoNo ratings yet
- PERDEV FIRST Periodical Test (2022)Document5 pagesPERDEV FIRST Periodical Test (2022)jeadryl LinatocNo ratings yet
- EVVO 10-15KW-G2 - IEC 61727 - ReportDocument25 pagesEVVO 10-15KW-G2 - IEC 61727 - ReportRadhwen ZayoudNo ratings yet
- A Rare Peripheral Odontogenic Keratocyst in Floor of Mouth: A Case ReportDocument6 pagesA Rare Peripheral Odontogenic Keratocyst in Floor of Mouth: A Case ReportIJAR JOURNALNo ratings yet
- Ccii Proposal EssayDocument4 pagesCcii Proposal Essayapi-456307983No ratings yet
- Rozdział 12 Słownictwo Grupa BDocument1 pageRozdział 12 Słownictwo Grupa BBartas YTNo ratings yet
- WWW CDC Gov/malaria/about/biologyDocument2 pagesWWW CDC Gov/malaria/about/biologyFiik FiikNo ratings yet
- A Systematic Review of Electromyography Studies in Normal Shoulders To Inform Postoperative Rehabilitation Following Rotator Cuff RepairDocument14 pagesA Systematic Review of Electromyography Studies in Normal Shoulders To Inform Postoperative Rehabilitation Following Rotator Cuff Repairshsh ShshsshNo ratings yet
- Batch Records HandoDocument39 pagesBatch Records HandoNiranjan SinghNo ratings yet
- Invoice, packing list mẫuDocument2 pagesInvoice, packing list mẫuPHI BUI MINHNo ratings yet
- Syntheis Writing 2 How Do Fear and Desire For Personal Acceptance Influence Human BehaviorDocument2 pagesSyntheis Writing 2 How Do Fear and Desire For Personal Acceptance Influence Human Behaviorapi-463684021No ratings yet